
Translate this page into:
The fifth cardiac chamber: Case of a huge left atrial appendage aneurysm
*For correspondence: akapoor65@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 35 year old female was referred to the Cardiology department of Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India in May 2014 for evaluation of shortness of breath which she had for the last two years. The patient was in sinus rhythm and cardiovascular examination was normal. Chest X-ray revealed a normal sized heart with a prominent bulge in the mid left cardiac border (Fig. 1, Panel A).
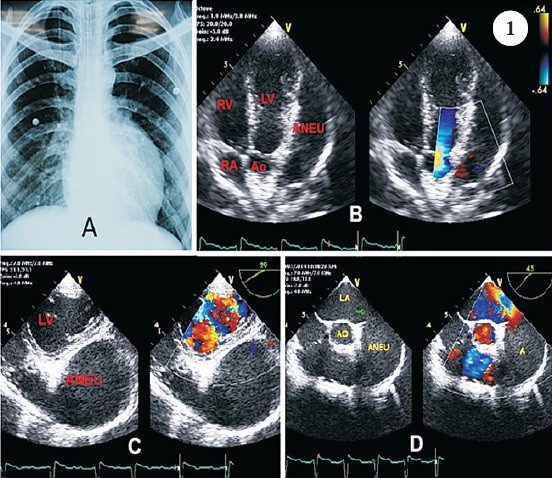
- Chest X-ray showing prominent bulge in the mid left cardiac border (Panel A), Modified apical 5-chamber view showing aneurysmal cavity (ANEU) along with normal 4 chambers (Panel B), Transgastric short axis view by trans-oesophageal echocardiography showing compression of left ventricle by aneurysm (Panel C), Trans-oesophageal short axis view demonstrating origin of aneurysm (Arrow) from left atrium (Panel D).
Trans-thoracic echocardiography with 3-D reconstruction revealed a large, elliptical left atrial appendage (LAA) aneurysm compressing the left ventricle (LV); the appearance of the large aneurysm extending along the LV lateral wall simulating a five-chambered heart on the modified apical and para-sternal short-axis views (Fig. 1, Panels B-D, Videos 1 & 2). The aneurysm was devoid of any thrombus, mitral and tricuspid valves were normal without any rheumatic involvement and bi-ventricular function was normal. A large, isolated LAA aneurysm arising from the left atrium was confirmed on trans-oesophageal echocardiography; pulse Doppler interrogation revealed preserved appendage filling and emptying pattern (Video 3). A 64-slice multidetector cardiac CT imaging with volume reconstruction was performed which clearly delineated a 51 x 66 mm LAA aneurysm extending antero-superiorly and to the left of the LV cavity (Fig. 2, Panels A-D). The patient was diagnosed to have an LAA aneurysm. She declined any surgical intervention; despite appendage flow being preserved, oral anticoagulation (OAC) was started to prevent any future thrombo-embolic events. The patient remained asymptomatic at the last six month follow up.
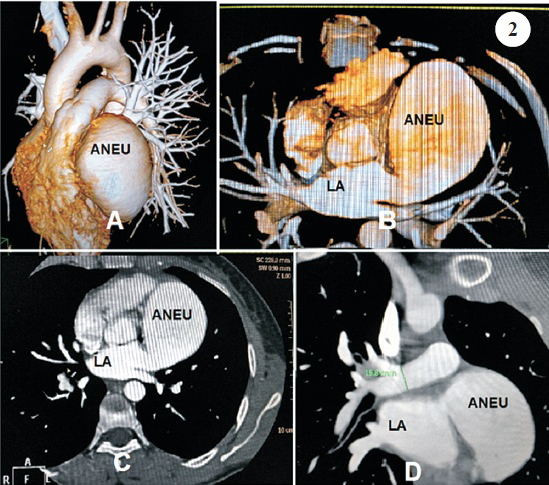
- Volume reconstruction of a 64-slice multidetector cardiac CT imaging showing location of aneurysm antero-superior and left to the left ventricle (Panels A & B), A 64-slice multidetector cardiac CT imaging measurements of aneurysm size of 51 x 66 mm (Panel C & D).
Video available at ijmr.org.in
Conflicts of Interest: None.




