Translate this page into:
Rare manifestations of sarcoidosis in modern era of new diagnostic tools
Reprint requests: Dr. S.K. Sharma, Head, Department of Medicine, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110 029, India e-mail: sksharma.aiims@gmail.com sksharma.aiims@yahoo.com
-
Accepted: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Growing body of literature on sarcoidosis in India has led to an increased awareness of the disease. With the advent of better imaging tools hitherto under-recognized manifestations of sarcoidosis are likely to be better recognized. We sought to study the rare clinical and radiological manifestations (<5%) in patients with sarcoidosis.
Methods:
Retrospective review of records of 164 patients with histopathologically proven sarcoidosis seen over six years in a tertiary care centre in north India, was done.
Results:
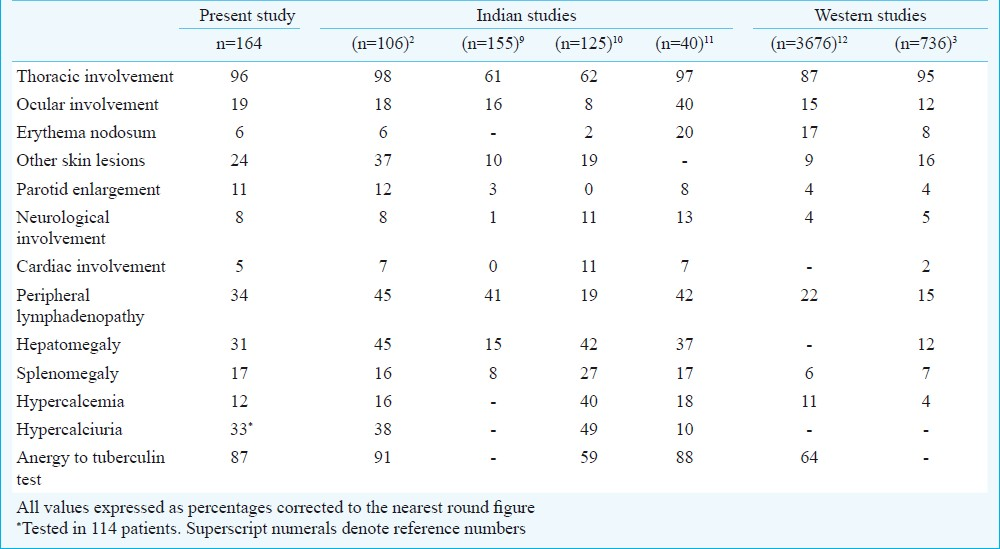
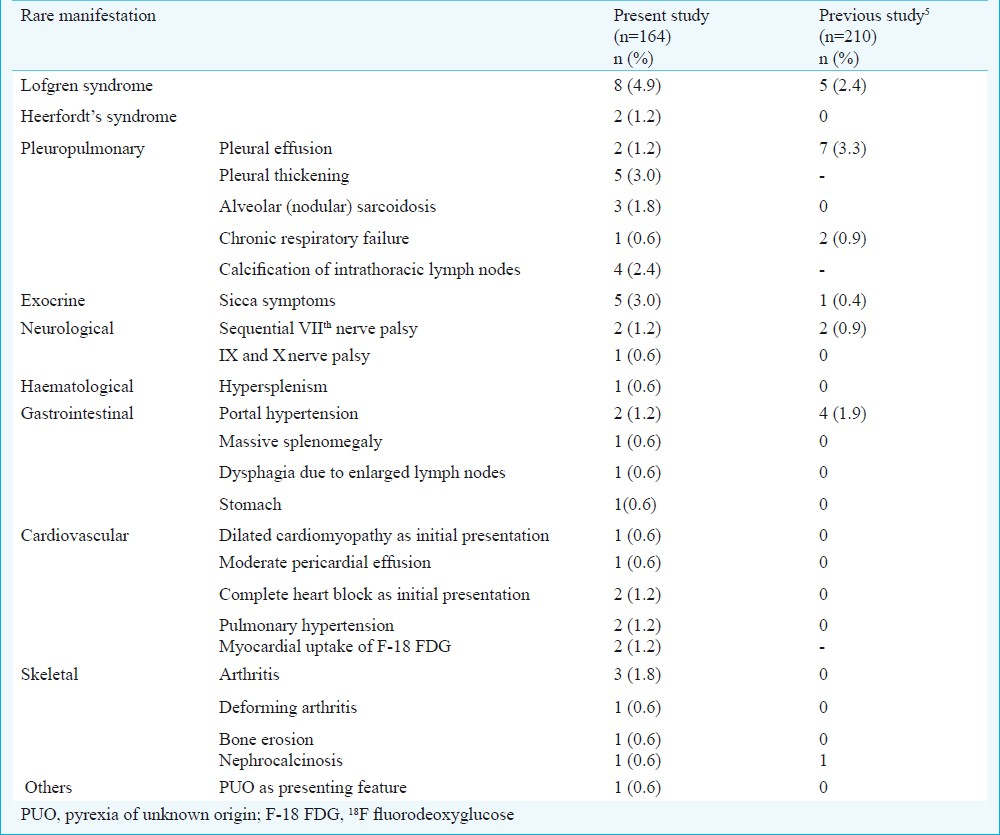
Fifty four rare manifestations were observed in 164 patients. Acute presentation in the form of Lofgren syndrome was seen in eight (4.9%) and Heerfordt's syndrome in two (1.2%) patients. Musculoskeletal manifestations included chronic sarcoid arthritis in three (1.8%), deforming arthritis and bone erosion in one (0.6%) each. Rare initial presentation with dilated cardiomyopathy in one (0.6%), complete heart block in two (1.2%), bilateral sequential facial nerve palsy in two (1.2%), and pyrexia of unknown origin was seen in one (0.6%) patient. Other rare manifestations included chronic respiratory failure in one (0.6%), dysphagia in one (0.6%), sicca syndrome in five (3%), massive splenomegaly in one (0.6%), portal hypertension in two (1.2%), hypersplenism, gastric sarcoidosis, ninth and tenth cranial nerve palsies, moderate pericardial effusion and nephrocalcinosis in one (0.6%) each, and pulmonary artery hypertension in two (1.2%) patients. Rare radiological manifestations included moderate pleural effusion in two (1.2%), pleural thickening in five (3%), calcification of intrathoracic lymph nodes in four (2.4%), alveolar (nodular) sarcoidosis in three (1.8%), and myocardial uptake of 18F-fluorodeoxyglucose (F-18 FDG) in two (1.2%) patients. Fourteen patients had airways obstruction and behaved typically like seasonal bronchial asthma with excellent response to corticosteroids.
Interpretation & conclusions:
Increased awareness of rare manifestations will facilitate better management of these patients. With increasing use of modern diagnostic tools, manifestations hitherto considered rare, are likely to be recognized more frequently in the future.
Keywords
India
rare manifestations
sarcoidosis

Sarcoidosis is a protean disease characterized pathologically by the formation of non-caseating granulomas. While involvement of virtually every tissue and organ has been described, the usual sites are lymph nodes, lungs, skin, spleen, liver, and the uveo-parotid region1–4. Rare manifestations of sarcoidosis include unusual patterns of organ involvement, or are the result of granulomatous inflammation developing in unusual locations for sarcoidosis.
There is only sparse information available from India on rare manifestations of sarcoidosis56. We reported a series with 93 uncommon manifestations in 210 biopsy proven patients previously5. Although the frequency of rare manifestations is low, lack of awareness leads to late diagnosis and management often leading to permanent sequelae. Awareness of rare manifestations will facilitate an early diagnosis and better management of these patients.
Here we present findings of a retrospective review of patient records to study the rare clinical and radiological manifestations of sarcoidosis. Rare manifestations were defined as clinical and radiological features occurring in less than 5 per cent of patients. The study also aimed to enumerate the clinical and laboratory profile of the patients, and compare them with that of the available data for Indian and western population.
Material & Methods
The study included a retrospective review of records of 164 histopathologically proven patients of sarcoidosis seen by us over six years between 2005 and 2010 at the All India Institute of Medical Sciences hospital, New Delhi. The protocol was approved by the Institute's ethics committee.
The inclusion criteria included the presence of typical clinical and radiological findings, histological evidence of noncaseating epithelioid cell granulomas from at least one site, and exclusion of other known causes of granulomatous disease. Patients with evidence of mycobacterial, fungal or parasitic infections and those with a history of exposure to organic and inorganic material known to cause granulomatous disease were excluded. Of the 205 patients seen during this period, 164 fulfilled the inclusion criteria and were included in the study.
All patients gave medical history and underwent a complete physical examination. Investigations included complete blood counts, serum biochemistry, liver function tests, kidney function tests, urine routine, 24-h urinary calcium excretion (on a restricted milk and calcium diet), serum angiotensin-converting enzyme (ACE) levels, chest radiograph, tuberculin skin test (TST) with intradermal injection of 0.1 ml purified protein derivative containing 5 tuberculin units (Span Diagnostic Ltd., Surat, India), pulmonary function tests and a detailed ocular examination including fundus evaluation. The serum ACE (SACE) level was used for diagnosis and monitoring the disease course. SACE activity was measured in all the subjects using the method described by Cushman and Cheung7. Pulmonary function tests (PFT) were studied in 86 patients at presentation. The lung volumes and their subdivisions were measured using a constant volume variable pressure body plethysmograph (PK Morgan, Chatham, Kent, UK).
The disease was staged by the traditional radiographic criteria8. Spiral computed tomography (CT) examination was performed from thoracic inlet to pubic symphysis after intravenous contrast administration. Axial 5 mm sections in mediastinal and lung window were reconstructed. Sequential axial high resolution computed tomography (HRCT) images of chest were separately acquired using 1.25 mm collimation. F-18 FDG (18-F-fluoro deoxyglucose) Positron emission tomography-computed tomography (PET-CT) was done in selected patients. The most accessible tissue and least invasive methods were used for histological diagnosis according to the clinical features.
Results
The mean age was 43.5 ± 9.3 yr with 79 (48.2%) males. The mean duration of symptoms was 29 ± 15 wk. Anergy to tuberculin test was seen in 143 (87.2%) patients. The most common methods of diagnosis were transbronchial lung biopsy in 54 (32.9%) and peripheral lymph node biopsy in 41 (25%) patients. Thoracic involvement was seen in 157 (96.3%) patients. At presentation, six (3.7%) had stage 0, 50 (30.5%) had stage I, 105 (64.0.%) had stage II, and three (1.8%) patients had stage III disease. Table I compares the clinical profile and laboratory characteristics with selected Indian and western series239–12.
Fifty four rare manifestations were seen in the 164 histopathologically proven patients of sarcoidosis (Table II). Acute sarcoidosis in the form of fever, bilateral hilar adenopathy, erythema nodosum and arthralgias (Lofgren syndrome) was seen in eight patients (Fig. 1 A & B); whereas, two patients had features of Heerfordt syndrome. Three patients had chronic sarcoid arthritis and one developed deforming arthritis of the knee joint.
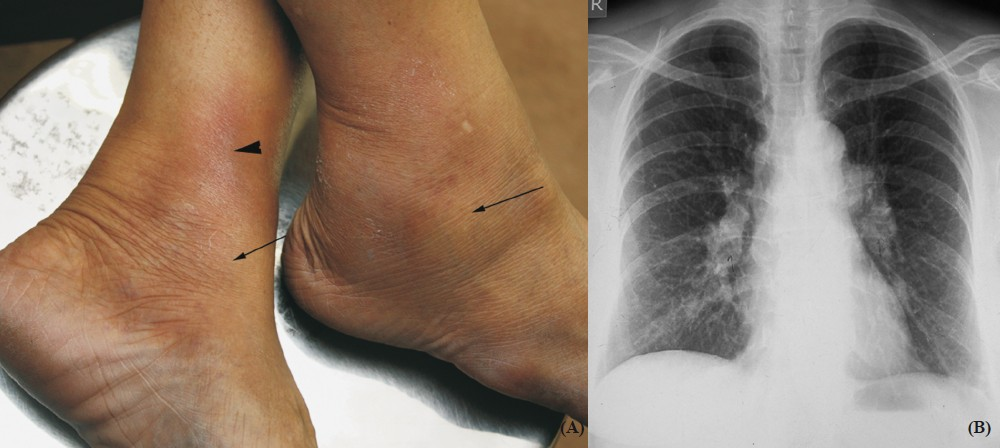
- Lofgren syndrome. (A) Middle-aged lady presented with bilateral ankle arthritis (arrows) and erythema nodosum (arrow head). (B) Chest radiograph of the same patient showing bilateral hilar adenopathy. Acute sarcoidosis in the form of Lofgren's syndrome is rare in India.
Neurological involvement was seen in 13 patients and two of them had presented initially with bilateral sequential facial nerve palsy. One patient had involvement of glossopharyngeal and vagus nerves. One patient with cardiac involvement had congestive heart failure as initial presentation due to dilated cardiomyopathy related to sarcoidosis. A 44 yr old female previously diagnosed with sarcoidosis had life-threatening thrombocytopenia refractory to medical treatment and required splenectomy for hypersplenism as a life saving measure. Dyspnoea with audible wheezing mimicking bronchial asthma was seen in 14 patients (Fig. 2), and one patient with advanced stage III disease had chronic respiratory failure. No significant differences were noted in the lung function tests between patients with and without rare manifestations.
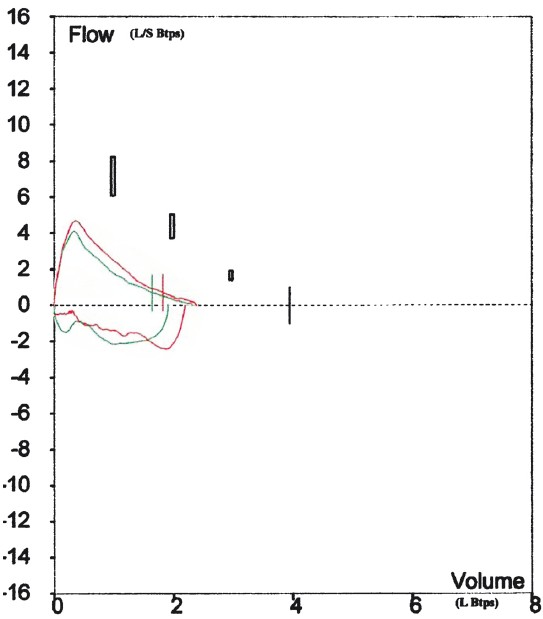
- Flow volume loops showing reversible airways obstruction in patient with sarcoidosis.
One patient died during the study period due to cardiac complications. One patient developed chronic respiratory failure and is on domiciliary oxygen therapy. The remaining patients with rare manifestations had good response to treatment. Selected clinical, radiological and histopathology images are shown in Figs 3,4 and 5, respectively.

- Clinical images in sarcoidosis. Bilateral lacrimal gland enlargement seen in a patient with sarcoidosis, right eye (A) and left eye (B). (C) Multiple erythematous plaques with superficial epidermal atrophy on exposed areas and sparing of nasolabial folds. The differentials include rosacea and lupus erythematosus. (D) Swollen left knee joint (thick arrow), synovial thickening of right knee joint (thin arrow). Synovial biopsy revealed non-caseating granulomas compatible with sarcoidosis. (E) Erythematous, tender nodules over extensor aspect of both legs suggestive of erythema nodosum, a non-specific cutaneous lesion in sarcoidosis, (F) Erythematous barely elevated plaque with well-defined margins developed on a scar over forehead (arrow). Skin biopsy revealed non-caseating granulomas. This condition is known as scar sarcoidosis and may be mistaken for keloids.
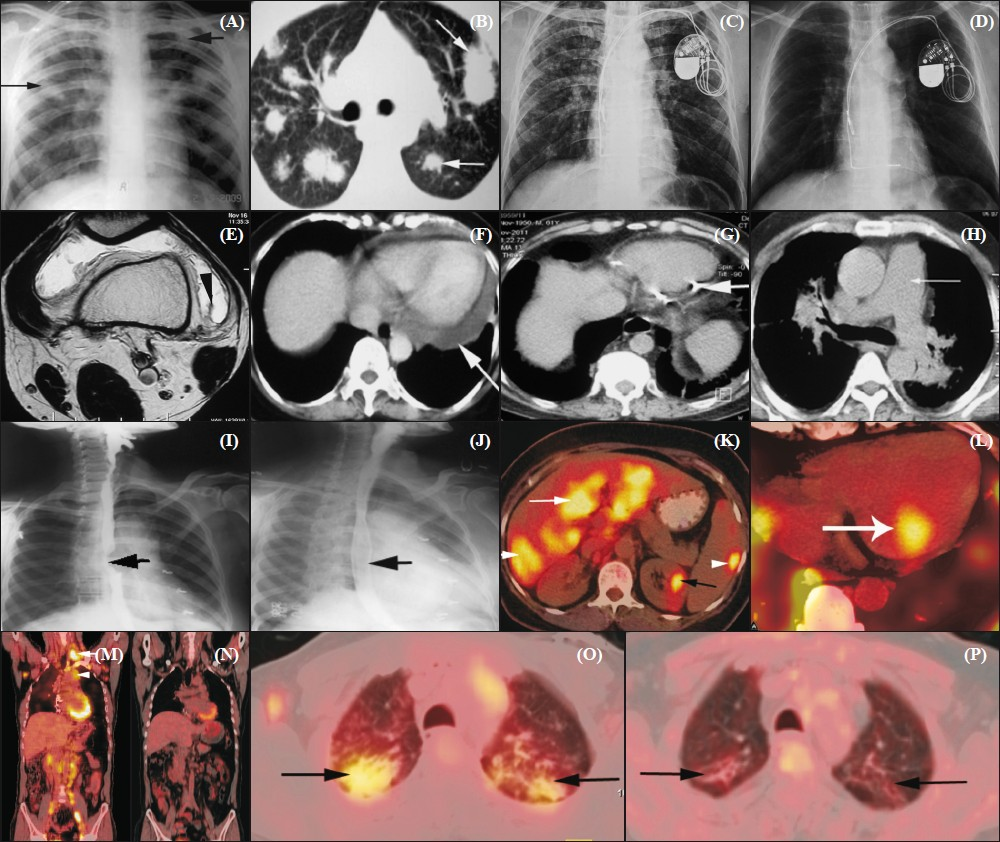
- Imaging in sarcoidosis. (A) Chest radiograph showing multiple poorly defined nodular shadows (arrows) in bilateral lung fields (B) HRCT scan axial section of the same patient showing large, discrete nodules (arrows) with fluffy margins in both lungs compatible with alveolar form of sarcoidosis. (C) Chest radiograph showing bilateral upper zone reticulonodular shadows; permanent pacemaker is also noted. Supraclavicular lymph node biopsy showed noncaseating epithelioid granulomas. The patient was referred with a possible diagnosis of MDR-TB. (D) Chest radiograph of the same patient after 6 months of corticosteroid therapy showing good response to treatment. (E) Axial T2W MR image of knee joint showing effusion in the joint space with synovial hypertrophy (arrow head). Synovial biopsy revealed non-caseating granulomas. (F) Axial CECT section showing pericardial effusion (arrow). There was good response to corticosteroids. (G) Axial CT scan of the chest showing pericardial calcification (arrow). (H) Axial CECT section showing significantly dilated main pulmonary artery (arrow). The diameter is more than adjacent aorta suggesting pulmonary hypertension. There is also marked peribronchovascular interstitial thickening. (I) Barium swallow image showing a localized filling defect (arrow) in mid-thoracic esophagus in a patient complaining of dysphagia for 3 months. CT revealed a subcarinal lymph nodal mass compressing the thoracic esophagus. (J) There was significant improvement in symptoms and radiographic appearance (arrow) after 3 months of corticosteroid treatment. (K) FDG PET-CT axial section showing increased focal uptake in liver (white arrow), spleen (arrow head) and kidney (black arrow). (L) FDG PET-CT axial section shows increased focal uptake in myocardium in a patient with cardiac sarcoidosis. (M) Coronal section FDG PET-CT scan showing increased FDG uptake in supraclavicular (arrow), mediastinal (arrow head), axillary and multiple mediastinal nodes in a patient with sarcoidosis. (N) Follow-up image after 6 months in the same patient shows good response with no abnormal uptake noted. (O) FDG PET-CT axial section showing increased uptake in parenchymal lesions (arrows) at initiation of therapy. (P) The parenchymal lesion showing no FDG uptake (arrows) in the same patient after 6 months of corticosteroid therapy.
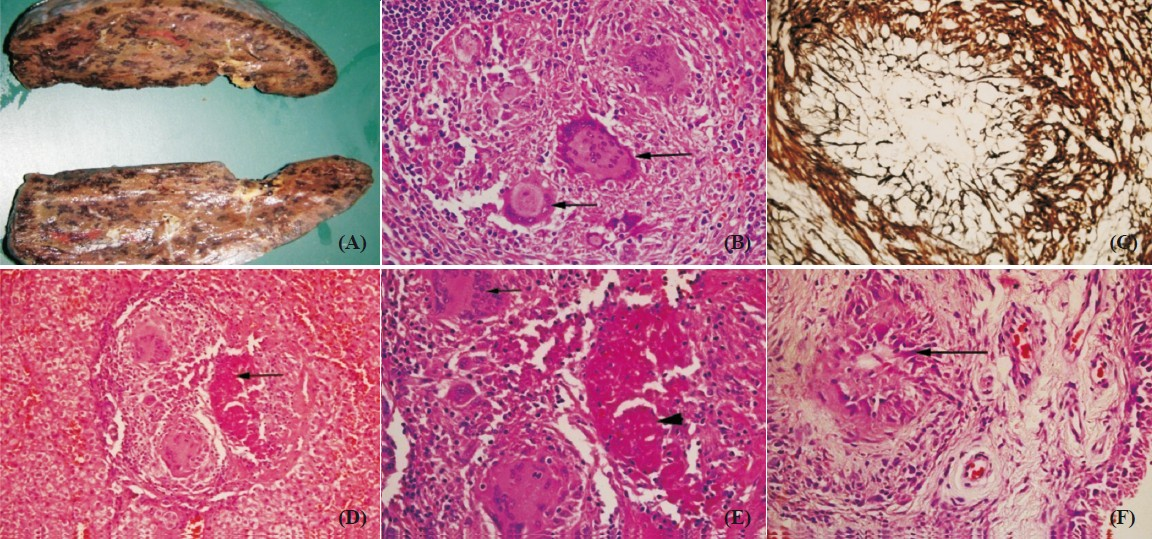
- Histopathological images. (A) Cut surface of spleen showing nodular lesions. (B) Microscopic examination from the lesions showing necrotizing granulomatous reaction with Langhans giant cells (arrows) on H&E stain; 400×. (C) These granulomas are rich in reticulin fibers as seen on silver stain; 200×. (D & E) Liver biopsy showing granulomatous reaction in the portal tract with Langhans giant cells and areas of necrosis (arrow in D and arrow head in E) on H&E stain at 100 & 200x respectively. (F) Arthroscopic synovial biopsy showing non-caseating granulomas (arrow) on H&E stain; 100×.
Discussion
Majority of the patients were in their fourth and fifth decade of life with a mean age of 43.6 yr, in contrast to western population, where 70 per cent of the patients were less than 40 yr of age. Pattern of organ involvement observed was similar to that described from other studies in India and western countries212. Anergy to TST was seen in 87 per cent of patients, consistent with previous observation in India2. The TST is frequently used to distinguish it from tuberculosis since a negative TST is highly sensitive for sarcoidosis. A positive TST in a patient suspected to suffer from sarcoidosis should be an absolute indication for a thorough work-up for tuberculosis1314. Incidence of hypercalcemia reported in sarcoidosis varies widely (2-63%) with higher figures reported in studies from North America15. However, the incidence of hypercalcemia in India is lower and the related complications like nephrocalcinosis, renal stones, and renal failure are rare, probably due to the prevalent vitamin D deficiency in the population.
Acute sarcoidosis in the form of Lofgren and Heerfordt's syndromes remains rare in India, as evident from the present study and previously reported literature from India15610. All patients with Lofgren syndrome showed a good response to steroids and had an excellent prognosis. None of these patients had relapse of the disease. This is in contrast to western literature where Lofgren syndrome has been reported in 20-30 per cent of white population4. Arthralgias were reported in 41.4 per cent patients; three patients had evidence of chronic sarcoid arthritis and one had deforming arthritis of the knee joint. While joint pains are reported in 25 to 39 per cent of patients with sarcoidosis, deforming arthritis is rare16.
Five patients had sicca symptoms with positive Schirmer's test; one of them having these features as presenting symptoms along with bilateral lacrimal and parotid gland enlargement (Mikulicz's syndrome). Sarcoidosis affects the lacrimal and salivary glands in 3 and 6 per cent cases, respectively17. Primary Sjögren's syndrome needs to be ruled out in these patients with a serology for detection of autoantibodies (anti-Ro/SS-A and anti-La/SS-B) and minor salivary gland biopsy. Future studies are warranted to look at association of sarcoidosis with autoantibodies and overlap with autoimmune diseases.
Two patients (1.2%) had pleural effusion and one had moderate-massive pericardial effusion. Serosal involvement has been thought to be unusual in sarcoidosis. Pleural effusion has been reported in less than 3 per cent of cases18, and asymptomatic minimal pericardial effusion in 20 per cent of cases19, though massive pericardial effusion is rare20. Presence of cardiomegaly in setting of sarcoidosis should prompt the physician to perform an echocardiography. Two patients developed sarcoidosis-associated pulmonary hypertension (SAPH) in the course of the disease. PH is now being recognized as a relatively common complication of sarcoidosis21; however, it is not commonly reported from India. Transthoracic Doppler echocardiography (TDE) is a useful non-invasive screening tool and should be a part of routine assessment in patients with long standing stage II and III disease. One patient had dilated cardiomyopathy at diagnosis; a rare presenting feature of sarcoidosis22. One patient had paroxysmal supraventricular tachycardia (PSVT) and the heart rate was controlled with amiadarone and by stepping up the dose of corticosteroids. He developed steroid induced severe diabetes mellitus. He was switched over to oral methotrexate (15 mg weekly), and is now stable with weekly methotrexate. Additionally, five other patients who had rare manifestations of sarcoidosis were treated with oral weekly methotrexate due to side-effects of steroids. Overall 140 of 164 patients received systemic corticosteroids and all of them showed good response to treatment. Severe thrombocytopenia due to hypersplenism is a rare complication in sarcoidosis23 which was seen in one patient.
Reversible airflow obstruction was observed in 14 patients. We had reported obstructive pattern to be the commonest finding in pulmonary function tests of patients with sarcoidosis in our previous series2. In a subsequent series we reported reversible airflow obstruction in 30 out of 210 patients (14.3%)5. These patients presented with seasonal deterioration of dyspnoea with wheezing and invariably associated with worsening of chest radiograph findings and features of reversible obstruction in pulmonary function tests. The episodes tend to be clustered around season change in March/April (after Holi, an Indian festival of colours) and ‘Deepawali’, a festival in India when crackers are burst, and the emitted smoke/“haze” in the atmosphere acts as an air-pollutant and precipitates airways obstruction in some of the patients with bronchial hyper-reactivity. These patients had excellent response to a short-course of inhaled corticosteroids and only occasionally required a short-course of systemic steroids for the control of symptoms; a subset of these patients may have bronchial asthma. Triggering agent for such events and host-genetic response are interesting areas for future research. Airway involvement with physiological obstruction has been documented in western literature24–26.
Three patients (1.8%) had features of alveolar (nodular) sarcoidosis, a rare radiological feature reported in 1-4 per cent of patients27. These patients had bilateral, multifocal, ill-defined nodules mimicking airspace disease. These lesions when present peri-pherally may be amenable to CT-guided biopsy. Four patients had nodal calcification on CT scan. Calcification is less common in chest radiographs in sarcoidosis compared to tuberculosis, its common differential28. The occurrence of lymph node calcification in sarcoidosis is closely related to the duration of disease and reported in 3 per cent of patients after 5 yr and in 20 per cent after 10 yr29. Increased use of HRCT chest has led to more frequent recognition of mild pleural effusion, pleural thickening and abnormalities of subpleural region.
Advances in technology have led to increasing use of less invasive methods for diagnosis and management of these patients. Endoscopic ultrasound-guided (EUS) FNAC from subcarinal lymph nodes was useful for diagnosis in two patients. Wider availability of endobronchial ultrasound (EBUS) in near future will obviate the need for more invasive diagnostic procedures. PET-CT was useful in detecting myocardial uptake in two patients with no clinical evidence of cardiac sarcoidosis. It also helped in detecting occult sites of disease involvement which were not evident on CT scan (Fig. 4K). PET scanning has provided physicians a valuable non invasive tool for locating occult sites of active disease and to evaluate previously under-recognized areas of sarcoidosis involvement3031. Increasing availability of PET-CT and introduction of PET-MRI in future will be useful in understanding the disease extent and its activity and change the way we understand and recognize rare manifestations at present.
Growing body of literature on sarcoidosis in India has increased awareness of the disease132; however, it is yet to emerge from shadows of the menace of tuberculosis in the country. Awareness of rare manifestations of sarcoidosis will help in better understanding of the disease, prompt pursuit of appropriate investigations for confirming the diagnosis and better management of these patients.
References
- Sarcoidosis: global scenario & Indian perspective. Indian J Med Res. 2002;116:221-47.
- [Google Scholar]
- Clinical characteristics, pulmonary function abnormalities and outcome of prednisolone treatment in 106 patients with sarcoidosis. J Assoc Physicians India. 2001;49:697-704.
- [Google Scholar]
- Clinical characteristics of patients in a case control study of sarcoidosis. Am J Respir Crit Care Med. 2001;164:1885-9.
- [Google Scholar]
- Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999. Am J Respir Crit Care Med. 1999;160:736-55.
- [Google Scholar]
- Spectrophotometric assay and properties of the angiotensin-converting enzyme of rabbit lung. Biochem Pharmacol. 1971;20:1637-48.
- [Google Scholar]
- Sarcoidosis in india: practical issues and difficulties in diagnosis and management. Sarcoidosis Vasc Diffuse Lung Dis. 2002;19:176-84.
- [Google Scholar]
- Sarcoidosis in India: a review of 125 biopsy-proven cases from eastern India. Sarcoidosis. 1990;7:43-9.
- [Google Scholar]
- Sarcoidosis in north India: the clinical profile of 40 patients. Sarcoidosis. 1987;4:155-8.
- [Google Scholar]
- Tuberculin skin test among pulmonary sarcoidosis patients with and without tuberculosis: its utility for the screening of the two conditions in tuberculosis endemic regions. Sarcoidosis Vasc Diffuse Lung Dis. 2006;23:130-4.
- [Google Scholar]
- Pleural effusions in a series of 181 outpatients with sarcoidosis. Chest. 2006;129:1599-604.
- [Google Scholar]
- Pericardial effusion concomitant with specific heart muscle disease in systemic sarcoidosis. Postgrad Med J. 1994;70(Suppl 1):S8-12.
- [Google Scholar]
- Association of sarcoidosis and immune thrombocytopenia: presentation and outcome in a series of 20 patients. Medicine (Baltimore). 2011;90:269-78.
- [Google Scholar]
- Pulmonary function in patients with endobronchial sarcoidosis. Acta Med Scand. 1984;215:121-6.
- [Google Scholar]
- Airway function in stage I and stage II pulmonary sarcoidosis. Respiration. 1984;46:17-25.
- [Google Scholar]
- Small airways function in pulmonary sarcoidosis. Scand J Respir Dis. 1978;59:37-43.
- [Google Scholar]
- Pulmonary sarcoidosis with an alveolar radiographic pattern. Thorax. 1982;37:448-52.
- [Google Scholar]
- The pattern and distribution of calcified mediastinal lymph nodes in sarcoidosis and tuberculosis: a CT study. Clin Radiol. 1996;51:263-7.
- [Google Scholar]
- Thoracic sarcoidosis: radiologic-pathologic correlation. RadioGraphics. 1995;15:421-37.
- [Google Scholar]




