
Translate this page into:
Hiatus hernia resulting in interstitial lung fibrosis due to repeated gastro-oesophageal aspirations
* For correspondence: sksharma.aiims2@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 67 yr old female† presented to the All India Institute of Medical Sciences, New Delhi, India, in 2010 with shortness of breath, which was attributed to interstitial lung fibrosis due to usual interstitial pneumonia. She was obese (body mass index: 39 kg/m2) and tachypnoeic (respiratory rate 34/min). Auscultation revealed classic ‘velcro’ crepitations. She had restrictive ventilatory defect: [forced vital capacity (FVC) 41 per cent of the predicted; forced expiration volume in one second (FEV1)/FVC 101 per cent; FEV1 41 per cent of the predicted; forced expiratory flow 25-75 per cent, 35 per cent of the predicted]. Arterial blood gas analysis (off O2 for 30 min) revealed type I respiratory failure; electrocardiogram: P pulmonale; on Doppler echocardiography, there was pulmonary hypertension (49 mmHg). Chest X-ray (Figure A) and computed tomography (Figure B and C) revealed hiatus hernia, interstitial lung fibrosis and scoliosis. She was treated with the following: continuous low-flow (2 l/min) domiciliary oxygen inhalation at least for ≥15 h/day, influenza and pneumococcal vaccinations, upright posture while sleeping, prompt treatment of infections whenever required and avoidance of exposure to environmental pollutants. She was doing well on follow up. Surgical intervention at this stage of illness was not possible.
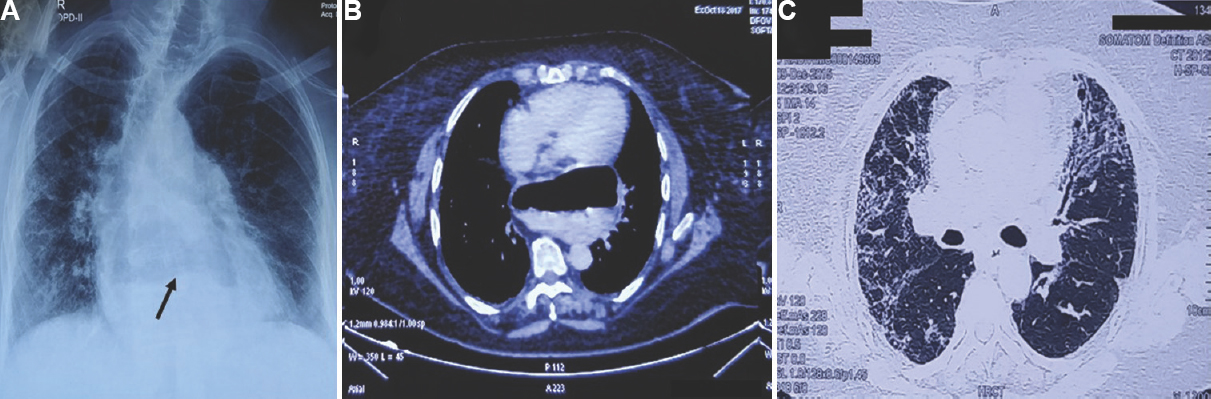
- (A) Chest radiograph (postero-anterior view) showing scoliosis and hiatus hernia. Arrows point to the air–fluid level in the stomach on the chest (A) X-ray and (B) computed tomography (CT) chest and changes of bilateral lung fibrosis (A and C). (C) CT chest (pulmonary window) showing changes of interstitial lung fibrosis (lingula on the left side, middle and lower lobes on the right side).
Conflicts of Interest: None.




