
Translate this page into:
Myeloid sarcoma of the joint: A rare presentation
*For correspondence: mbhattyacharyya@yahoo.co.in
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 17 yr old female† attended the Orthopaedics outpatient department (OPD) of the Medical College & Hospital, Kolkata, India, in April 2019, with progressive left elbow painful swelling and fever for the preceding one month (Figure A). Her complete haemogram was within normal limits. Magnetic resonance imaging of the left elbow joint showed a large lesion involving the articular cartilage and synovium and infiltrating the joint cavity (Figure B). Following no response to empirical antibiotics, fine-needle aspiration was done which showed atypical cells with blastoid morphology (Figure C). The patient was referred to the Haematology OPD. On identifying Auer rods in the blastoid cells (Figure C), bone marrow aspiration was done which showed 25 per cent of the blasts with myeloid immunophenotype. Diagnosed as acute myeloid leukaemia with myeloid sarcoma of the joint, the patient was treated with standard induction chemotherapy following which the joint swelling regressed. Myeloid sarcomas of joints are rare and in this case no blasts were observed in the peripheral blood. Fever with joint swelling not responding to antibiotics was the only clue for diagnosis.
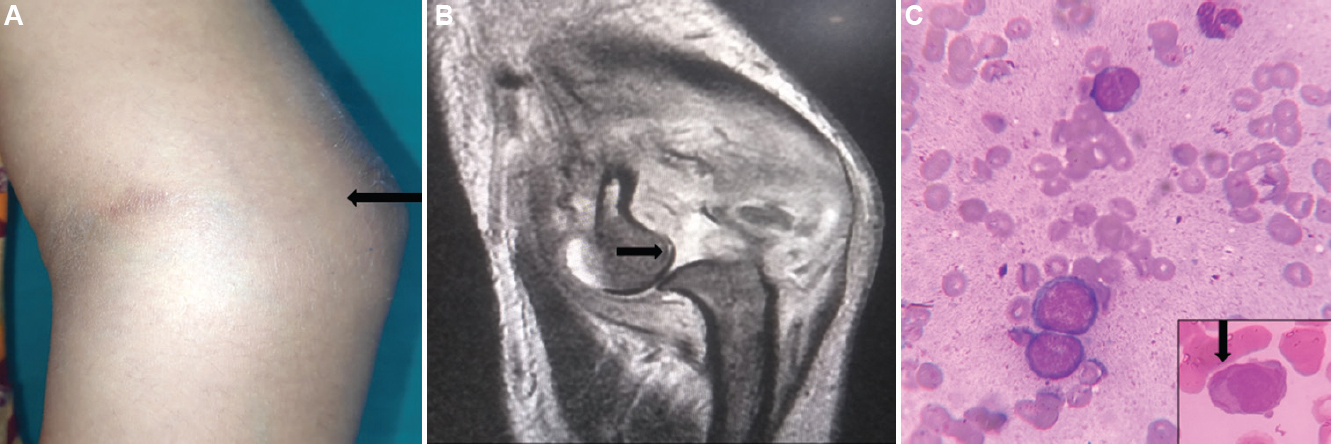
- (A) Photograph showing the left elbow swelling (arrow). (B) T2-weighted magnetic resonance image (coronal section) of the left elbow joint showing a large lesion impinging onto the articular surface and destruction of the joint along with the posterior subluxation of radius (arrow). (C) Fine-needle aspiration from the swelling showing blasts (LG, ×40); inset showing a blast with the Auer rods (arrow) (LG, ×100). LG, Leishman Giemsa stain.
Acknowledgment:
Authors acknowledge Dr Aniruddha Dey, department of Orthopedics, for referring the patient to the Hematology OPD for further diagnosis and management.
Conflicts of Interest: None.




