Translate this page into:
Unusual localization of parathyroid carcinoma in anterior chest wall
*For correspondence: cvhari5endo@rediffmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 36-year old male presented to Endocrinology OPD, Fortis Hospitals, Bangalore, India, with low serum 25-hydroxy vitamin D levels, normal calcium and parathyroid hormone (PTH) levels (Fig. 1) a year after endoscopic excision of left inferior parathyroid adenoma. With calcium and vitamin D supplementation he developed hypercalcaemia. After stopping supplementation, he presented with hypercalcaemia and high PTH levels. Routine nuclear scanning (MIBI scan) did not reveal any increased uptake in the region of neck or ectopic sites for parathyroid gland. Ga68 DOTANOC whole body PETCT scan revealed two well defined lesions in the right upper anterior chest wall (Fig. 2a, b). Histology confirmed it to be parathyroid carcinoma (Fig. 3). Post-operatively serum biochemistry was normalized. The unusual location of parathyroid gland is probably due to migration of right parathyroid gland down to the anterior chest wall during previous endoscopic surgery which has gone for migtogenic change1. Clinical presentation of adenoma on one side and later occurrence of carcinoma on the other gland is rare2.
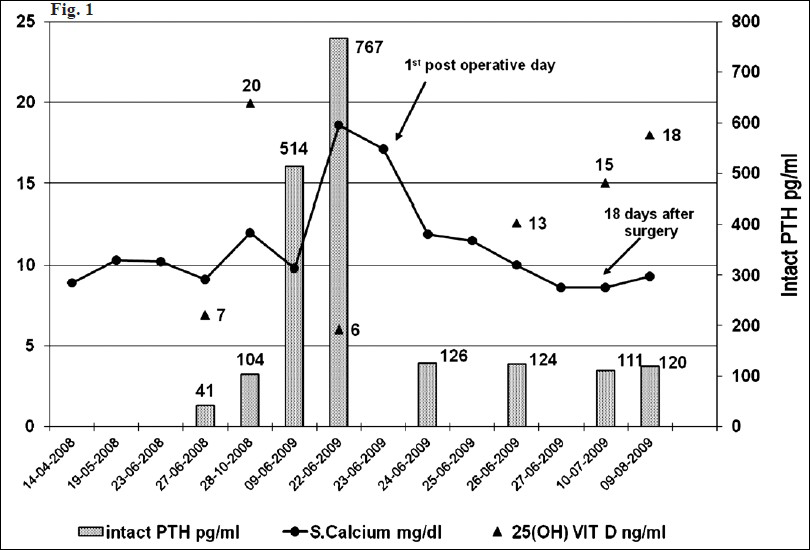
- Graphical representation of serum calcium (normal 8.5 to 10.5 mg/dl); 25(OH) vitamin D (normal >32 ng/ml) and intact parathyroid hormone (normal 32 to 75 pg/ml) in the patient from the time of presentation till post-operative period.
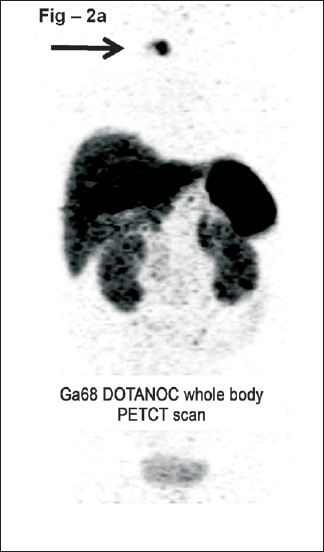
- Ga68 Dotanoc whole body PETCT scan. Two well defined smoothly marginated slightly lobulated soft tissue lesions in the right upper anterior chest wall just above the level of jugular notch to the right of midline which are Ga68 Dotanoc avid (arrow).
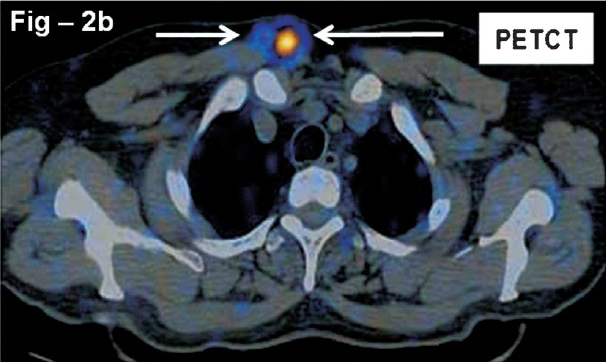
- Fused PET CT image. There are two well defined smoothly marginated slightly lobulated soft tissue dense lesions measuring 1.6 × 1.5 cm and 1.2 × 1.2 cm in the right upper anterior chest wall just above the level of jugular notch (arrows).
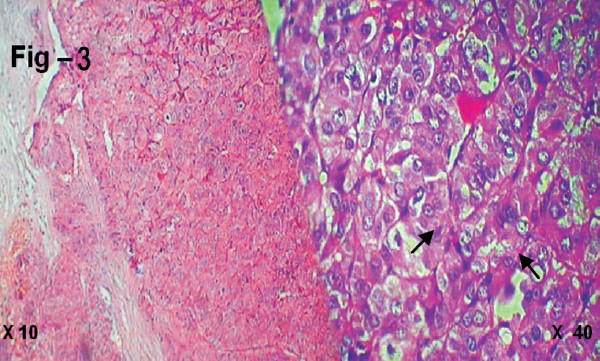
- Histology of the excised lesion (×10 and ×40) (weight 5 g) showing cells arranged in trabeculae and nests separated by fibrovascular septae. The cells show moderate to abundant granular cytoplasm, large vesicular nuclei and prominent nucleoli with little mitosis and no necrosis (arrows).
Acknowledgment
The authors acknowledge Dr M.G. Bhat, Minimal access surgeon and Drs Shantha Krishnamurthy and Kshithija Kulkarni for their kind support in this case.
References
- Synchronous parathyroid carcinoma, parathyroid adenoma, and papillary thyroid carcinoma in a patient with severe and long-standing hyperparathyroidism. Endocr Pract. 2009;15:463-8.
- [Google Scholar]
- Synchronous occurrence of parathyroid carcinoma and adenoma in an elderly woman. Surgery. 1989;106:929-33.
- [Google Scholar]




