
Translate this page into:
Unusual aortic rupture: What is cold can become catastrophic!
*For correspondence: sanjeevradio@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
An 18 yr old male† patient with spinal tuberculosis presented to the department of Cardiovascular Radiology and Endovascular Interventions, All India Institute of Medical Sciences, New Delhi, India, in September 2018, with acute aortic rupture (Figure A-D). This was successfully managed with endovascular stent graft (Figure E). Follow up computed tomography angiogram done after one month showed patent aortic stent graft with no leak (Figure F). The patient is stable with patent aortic graft now. The patent was given anti-tuberculosis therapy (ATT) one month prior to the aortic stenting and continued for six months following the procedure. Pott's spine is one of the most common skeletal sites of extra-pulmonary tuberculosis, which can cause significant complications. The associated large para-vertebral abscess often erodes adjacent structures and rarely involves the aortic wall causing its dehiscence. The treatment of such devastating complications is controversial. Surgery, along with ATT, may be beneficial. However, it is quite challenging due to intra-operative complications and poor functional status of these patients.
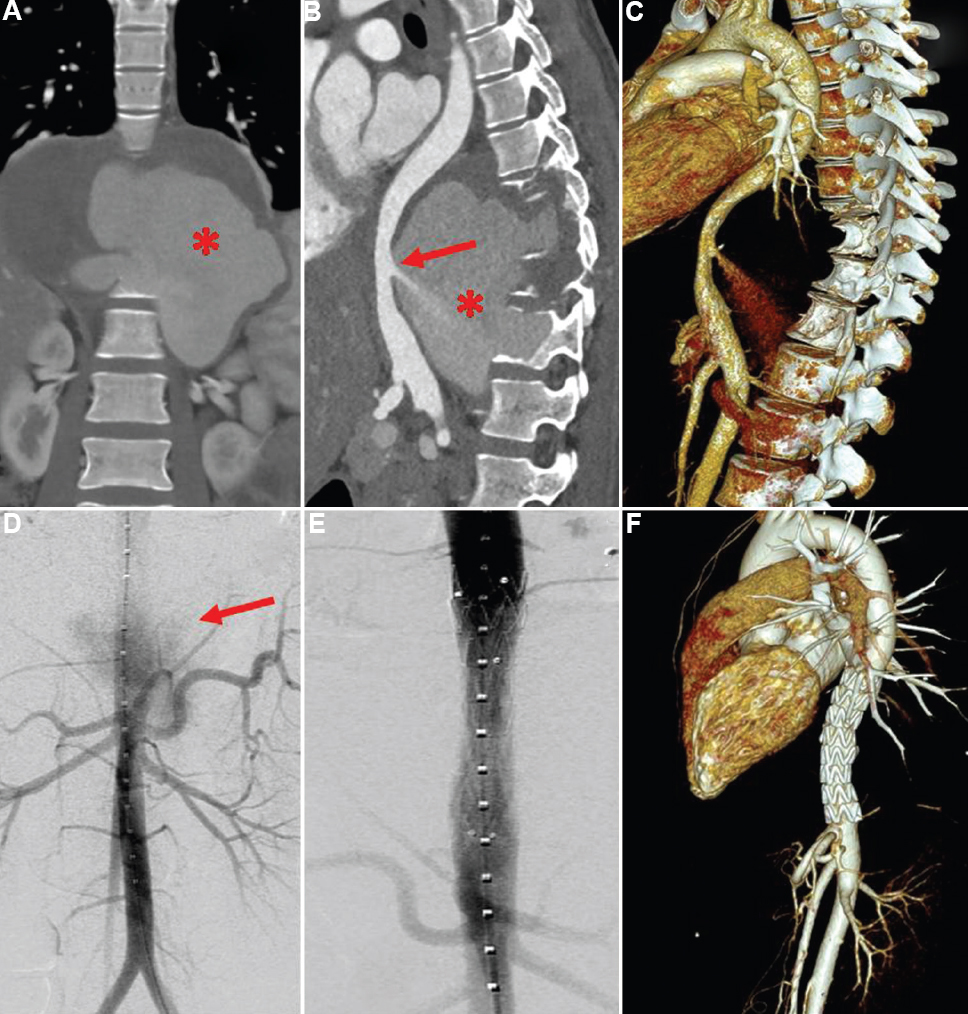
- Computed tomography (CT) showing abdominal aortic rupture into the tubercular paravertebral abscess. (A) Coronal view. (B) Sagittal view. (C) Volume-rendered CT reconstructions showing active contrast extravasation from the posterior wall of juxtadiaphragmatic aorta into the large paravertebral abscess (red arrow). Hyperdense contents (blood) noted in the abscess (asterisks). (D) Digital subtraction angiogram revealing active contrast extravasation from the abdominal aorta (red arrow). (E) Abdominal aortic stent graft was deployed with no contrast leak. (F) Follow up computed tomography after one month showing aortic stent graft with no leak.
Conflicts of Interest: None.




