Translate this page into:
Unenhanced low-dose versus standard-dose CT localization in patients with upper urinary calculi for minimally invasive percutaneous nephrolithotomy (MPCNL)
*Jiang LC and Fan YD contributed equally to the work.
Reprint requests: Dr Xu Zhonghua, Department of Urology, Qilu Hospital, Shandong University, 44#, Wenhua Xi Road, Jinan, 250 012, P.R. China e-mail: xuzhonghua001@163.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
With the ethical concern about the dose of CT scan and wide use of CT in protocol of suspected renal colic, more attention has been paid to low dose CT. The aim of the present study was to make a comparison of unenhanced low-dose spiral CT localization with unenhanced standard-dose spiral CT in patients with upper urinary tract calculi for minimally invasive percutaneous nephrolithotomy (MPCNL) treatment.
Methods:
Twenty eight patients with ureter and renal calculus, preparing to take MPCNL, underwent both abdominal low-dose CT (25 mAs) and standard-dose CT (100 mAs). Low-dose CT and standard-dose CT were independently evaluated for the characterization of renal/ureteral calculi, perirenal adjacent organs, blood vessels, indirect signs of renal or ureteral calculus (renal enlargement, pyeloureteral dilatation), and the indices of localization (percutaneous puncture angulation and depth) used in the MPCNL procedure.
Results:
In all 28 patients, low-dose CT was 100 per cent coincidence 100 per cent sensitive and 100 per cent specific for depicting the location of the renal and ureteral calculus, renal enlargement, pyeloureteral dilatation, adjacent organs, and the presumptive puncture point and a 96.3 per cent coincidence 96 per cent sensitivity and 93 per cent specificity for blood vessel signs within the renal sinus, and with an obvious lower radiation exposure for patients when compared to standard-dose CT (P<0.05). The indices of puncture depth, puncture angulation, and maximum calculus transverse diameter on the axial surface showed no significant difference between the two doses of CT scans, with a significant variation in calculus visualization slice numbers (P<0.05).
Interpretation & conclusions:
Our findings show that unenhanced low-dose CT achieves a sensitivity and accuracy similar to that of standard-dose CT in assessing the localization of renal ureteral calculus and adjacent organs conditions and identifying the maximum calculus transverse diameter on the axial surface, percutaneous puncture depth, and angulation in patients, with a significant lower radiation exposure, who are to be treated by MPCNL, and can be used as an alternative localization method.
Keywords
Low-dose CT
minimally invasive percutaneous nephrolithotomy (MPCNL)
puncture localization
unenhanced spiral CT scan
upper urinary tract calculus

With the development of spiral CT and multi-slice CT technique, not only is the scan time shortened, the interference and influence of breathing factors on figures can also be avoided123. Because of the unique and powerful post-processing function, the use in spiral CT in percutaneous nephrolithotomy (PCNL) attracts more attention, especially in the design of percutaneous renal access building4567. Spiral CT localization has become the standard imaging tool for PCNL after X-ray and ultrasound8. Because of the administered radiation, an ethical concern about the dose CT scan has been raised910, and more attention has been paid to low-dose CT111213. Several studies have shown that low-dose CT can be applied in the screening of patients with suspected renal colic141516171819. Further, low-dose CT might achieve a sensitivity and specificity close to standard-dose CT in detecting ureteral stones with lower-dose exposure2021. No reports are available about the use of low-dose spiral CT scan in localization for MPCNL treatment.
The purpose of this study was to approach the probability of unenhanced low-dose CT application in MPCNL for upper urinary tract calculus treatment. In the present study, unenhanced low-dose CT was compared with standard-dose CT localization for MPCNL in patients with upper urinary calculi by evaluating the stone slice numbers, maximum size on the axial surface, location, obstructive signs, perirenal adjacent organs’ conditions, puncture point determination and percutaneous access design, percutaneous puncture depth and angulation measuring.
Material & Methods
From July to October 2010, 28 adult patients (19 men, 9 women; aged 32-76 yr, mean age, 50 ± 11 yr) with upper urinary tract calculus evaluated for treatment in the department of Urology, Qilu Hospital, Jinan, P.R. China, by MPCNL were involved in the study (renal pelvis stones in 7 cases, left in 1, right, 6; simple calyceal stones in 4, left in 2 cases, right side in 2; pelvis renal calyceal stones in 7, left in 4, 3 cases of right; ureteral stones in 10 cases, left in 4, the right side in 6). Body mass index (BMI) was <18.5 kg/m2 in 3, 18.5 - 24.9 in 11, 25 - 29.9 in 10, and >30 in four patients. All patients underwent B-ultrasound, kidney, ureter and bladder radiograph (KUB), and intravenous pyelogram (IVP) inspection before localization. The study protocol was approved by the ethical committee of Qilu Hospital, Shandong University Jinan. Informed written consent was obtained from all patients.
Localizing method and scan parameters: All patients routinely underwent an unenhanced spiral CT localization scan in a prone position, completely analogous to the intraoperative body posture pre-operation, with a pre-set flat plate on the examining table of the spiral CT and two cushions under the chest and abdomen, respectively. The roughly percutaneous renal puncture points were designed at the area between the posterior axillary line and scapular line under or above the twelfth rib according to the plain abdominal radiograph and intravenous IVP. The CT scan was taken in a breath-holding state at the end of inspiration. The puncture depth and angulation were measured on the CT image when the slice was determined for puncture use (Fig. 1), and all the calculations were made by MPR and 3D reconstruction simultaneously for identifying the stone size, shape, branch condition, and spatial distribution, as well as hydronephrosis and hydrocalycosis.
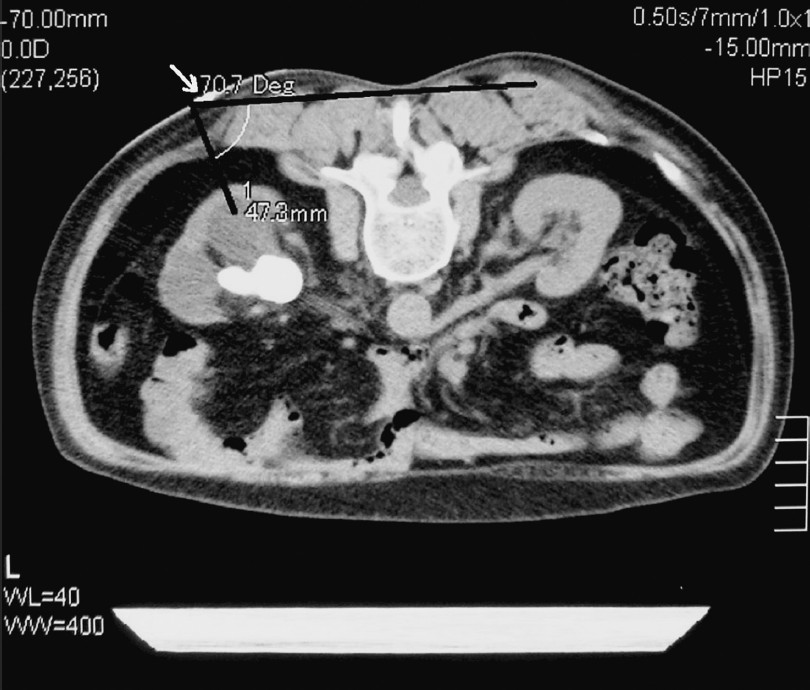
- The presumed percutaneous puncture point, puncture depth, and angulation were determined on the right axial surface slice. A 65-year-old women with left renal stone: the puncture depth from the DTZ-coated fabric particle (the presumed puncture point, white arrow) to dilatate the post-calyx is 47.3 mm, and the puncture angulation, which means the included angle between puncture route and human back body plane, is 70.7 degree.
The CT scan was performed from the lung bases to the superior border of the pelvis using a 16-MDCT scanner (Aquilion, Toshiba, Japan). The low-dose CT scan followed the standard-dose CT scan immediately. Standard-dose CT was obtained with 7-mm contiguous sections, a table speed of 5 mm/sec (pitch = 1), 120 kV, and 100 milliampere second. Low-dose CT was performed with the following parameters: reconstruction slice thickness, 7.0 mm; pitch, 1.00; gantry rotation speed, 0.5 second; tube potential, 120 kV; and tube charge per gantry rotation, 25 mAs (50 mA x 0.5 sec /1.00 = 25 mAs).
Index observation and data collection: In all 28 patients, standard-dose CT images were interpreted immediately by an associate chief or chief physician, and the interpretation of low-dose CT images was done by two other attending radiologists who were blinded to the standard-dose CT findings, patients’ names, and demographics. The slices for puncture use on both standard-dose and low-dose CT images were determined by the same surgeon with 4-5 years of experience on MPCNL, and then the puncture depths and angulations were measured by two attending urologists independently. In our study, only the unenhanced CT images were interpreted.
The recorded information for both low-dose and standard-dose CT examination included: (i) The numbers of stone slices and the size and location of calculi in the urinary tract and diatrizoate (DTZ)-coated fabric particle. Location was reported as ureter, renal pelvic, and calyceal, the slice of fabric particle coated with DTZ. (ii) Indirect or secondum signs of proximate urinary obstruction (renal enlargement, pyeloureteral dilatation, or periureteral or perirenal stranding). (iii) Puncture depth and puncture angulation. (iv) Blood vessels within the renal sinus, perirenal adjacent organs’ conditions. (v) The volume CT dose index (CTDIvol) (which can be read from the CT workstation), and scan length (L) (scanned from the superior border of T12 to inferior border of L3).
The effective dose (E) of CT scan was obtained by the following formula: E= CTDIvol×L×f (where f is a specific conversion factor, and for which the f of abdominal region is 0.015)2223.
Statistical analysis: Statistical software SPSS (version 17.0, USA), was used for the data analyses. A paired t-test was used for mean comparisons for measurement data, and Wilcoxon signed rank test for numeration data. Two-tailed Fisher's exact test was used for group comparison, and student's t test was used for mean comparisons.
Results
Low-dose CT was the same (100% sensitive) as the unenhanced standard-dose CT for identifying one direct or indirect sign showing a renal and ureteral calculus and the adjacent organs’ conditions. All 28 patients were shown on low-dose CT with a direct or indirect sign of calculus. No significant difference was seen between the two groups at puncture depths and angulations for patients with various BMIs, except calculus visualization slice number (P<0.05), and the same for the identification of a direct or indirect sign of a calculus (100% sensitivity and 100% specificity), except for blood vessels within the renal sinus (shown in 26 kidney in low-dose CT and 27 in standard-dose CT) (96% sensitivity and 93% specificity) (Figs 2-5). The conditions (sensitivity) of low-dose CT for detecting direct or indirect signs of a renal or ureteral calculus, signs of DTZ-coated fabric particles, and blood vessels within the renal sinus and adjacent organs with a definite relationship in patients are shown in Table I. The comparison of radiation exposure (E), calculus sizes (numbers of stone slices, maximum diameter on the axial plane), puncture depths, and angulations is shown in Table II.
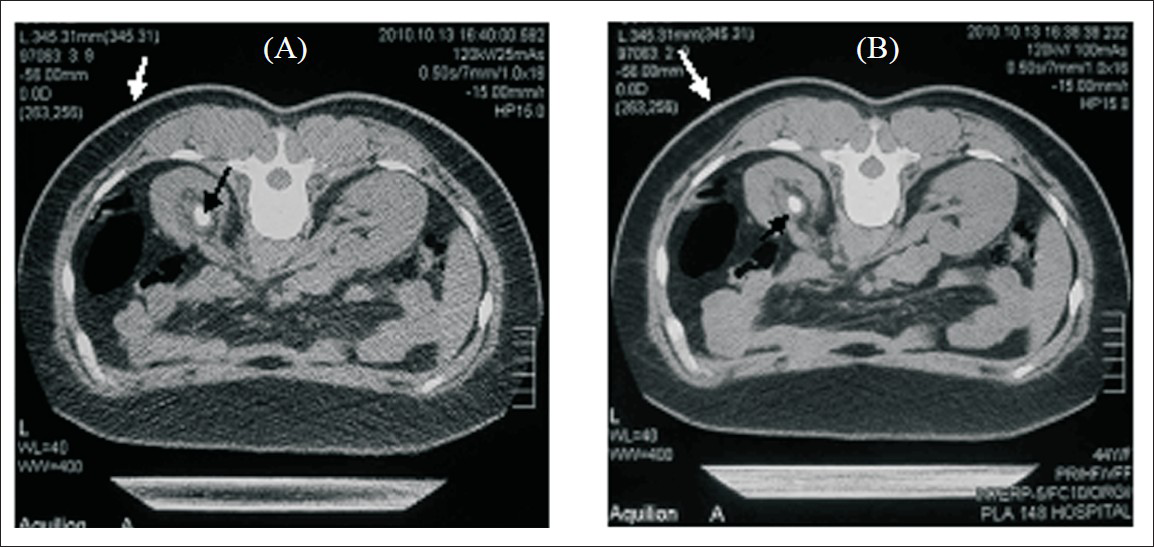
- Direct signs of renal calculi and DTZ-coated fabric particles were detected in patients on both low-dose CT and standard-dose CT images. A 28-year-old woman with left renal calculus: upper abdomen axial low-dose CT image (120 kV, 25 mAs, pitch of 1.00, 7-mm collimation) (A) shows a pelvic stone (black arrow) and DTZ-coated fabric particle (white arrow). Same findings are shown on standard-dose CT image (120 kV, 100 mAs, pitch of 1, 7-mm collimation) (B).
- Indirect signs of upper urinary tract calculus were detected in all 28 patients on both low-dose CT and standard-dose CT images, with 28 cases of nephrohydrosis; of which 20 cases showed renal enlargement on some different degrees. A 63-year-old man with left upper ureteral calculus: upper abdomen axial low-dose CT image (120 kV, 25 mAs, pitch of 1.00, 7-mm collimation) shows a ureteral stone (black arrow), renal enlargement, and nephrohydrosis (white arrow) (A). The same findings are shown on the standard-dose CT image (120 kV, 100 mAs, pitch of 1, 7-mm collimation) (B).

- The puncture depths and angulations were measured on both low-dose CT and standard-dose CT images, without significant differences of the two indices in all 28 patients. A 60-year-old woman with right renal calculus: upper abdomen axial low-dose CT image (120 kV, 25 mAs, pitch of 1.00, 7-mm collimation) (A) shows that the puncture depth and angulation were 65.5 mm and 46.2 degrees, which were shown on the standard-dose CT image (120 kV, 100 mAs, pitch of 1, 7-mm collimation) to be 65.5 mm and 45.8 degrees (B).

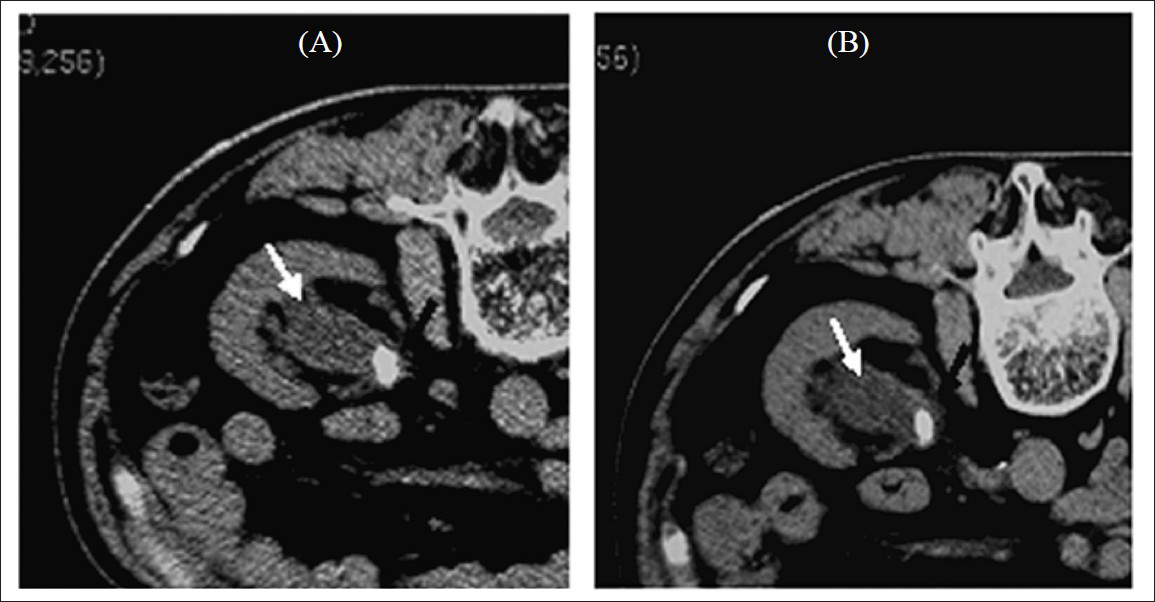
- The signs of blood vessels within renal sinus were shown in 26 cases on low-dose CT of which shown in 27 cases on standard-dose CT of all the 28 cases. A 53-year-old man with right upper ureteral calculus, upper abdomen axial low-dose CT image (120 kV, 25 mAs, pitch of 1.00, 7-mm collimation) (A) shows renal vein and its branch (white arrow). Same findings are shown on standard-dose CT image (120 kV, 100 mAs, pitch of 1, 7-mm collimation) (B)


Discussion
Characterization of stone morphology and location are the major advantages of CT over other imaging techniques (abdominal radiography, sonography) commonly used in the initial evaluation of patients with suspected renal colic2425, but the increased radiation dose delivered with CT, low-dose CT is a cause of concern. Researchers have suggested that low-dose CT protocols delivering a radiation dose close to that of an abdominal radiograph may be comparable to standard-dose CT for detecting ureteral stones132021. According to their results, the dose delivered by low-dose CT of 25 mAs was an estimated one-fourth of the standard-dose CT (100 mAs) for the same scanning area132223.
In our study, the low-dose CT achieved excellent coincidence sensitivity (100%) and specificity (100%) in evaluating renal and ureteral calculi on the basis of direct (detection of calculus) and indirect CT signs, perirenal adjacent organs’ conditions, percutaneous renal access design, puncture point localization, and puncture depth and angulation measuring, using standard-dose CT as the reference standard. The low dose could reduce 75 per cent of the radiation exposure along with the low-dose CT use of 25 mAs, as compared to 100 mAs, being consistent according to the literature reports132223.
For stone size, it has been shown that low-dose CT is equivalent to standard-dose CT for detecting stones ≥3 mm in the ureters of patients with a BMI <30 kg/m2; low-dose CT does not miss any calculus ≥3 mm in patients with a BMI <30 kg/m213. Some researchers consider that patients with a BMI >31 kg/m2 should not undergo a low-dose CT examination for the assessment of ureteral calculi15. These may not be applicable for the upper urinary calculi prepared for MPCNL.
In our study, there was excellent coincidence between patients with a BMI <30 and >31 kg/m2 for direct or indirect signs in localization for MPCNL use, except for signs of blood vessels within the renal sinus. Despite the excellent sensitivity and specificity, a major drawback of low-dose CT is the limitation in the determination of the exact stone size, when compared to standard-dose CT. Therefore, clinicians should be clearly informed, before MPCNL treatment that the size of calculi on low-dose CT may vary by ± 20 per cent compared with standard-dose CT results13.
In the current study, the direct and indirect signs of upper urinary calculi and perirenal adjacent organ information of low-dose CT were competent enough for percutaneous access design for MPCNL or PCNL treatment, to get information, such as stone size, location, pyeloureteral dilatation, and renal enlargement, as well as the puncture point determination, puncture depth and angulation, and even the anterior or posterior branches of renal blood vessel conditions. But, for the detailed and accurate blood vessel information, advanced angiographic CT (ACT) should be included262728.
In conclusion, the results of this study suggest that a low-dose CT protocol in the prone position can be used as the first-line imaging tool in the unenhanced CT localization for patients with upper urinary calculi who are to be treated by MPCNL or PCNL with lower radiation exposure for patient.
References
- Spiral volumetric CT with single-breath-hold technique, continuous transort, and continuos scanner rotation. Radiology. 1990;176:181-3.
- [Google Scholar]
- Computerized tomography guided access for percutaneous nephrostolithotomy. J Urol. 2003;170:45-7.
- [Google Scholar]
- Planning percutaneous nephrolithotomy using multidetector computed tomography urography, multiplanar reconstruction and three-dimensional reformatting. BJU Int. 2005;95:1280-4.
- [Google Scholar]
- Should PCNL patients have a CT in the prone position preoperatively? Can J Urol. 2010;17:5082-6.
- [Google Scholar]
- Diagnosis and management of postpercutaneous nephrolithotomy residual stone fragments. J Endourol. 2009;23:1751-5.
- [Google Scholar]
- Evaluation of the patient with flank pain and possible ureteral calculus. Radiology. 2003;228:319-29.
- [Google Scholar]
- Radiation dose associated with unenhanced CT for suspected renal colic: impact of repetitive studies. AJR Am J Roentgenol. 2006;186:1120-4.
- [Google Scholar]
- Low-dose chest CT: optimizing radiation protection for patients. AJR Am J Roentgenol. 2004;183:809-16.
- [Google Scholar]
- low-dose versus standard-dose CT protocol in patients with clinically suspected renal colic. AJR Am J Roentgenol. 2007;188:927-33.
- [Google Scholar]
- Low dose computed tomography in suspected acute renal colic. Clin Radiol. 2001;56:873-6.
- [Google Scholar]
- Low dose unenhanced helical computerized tomography for the evaluation of acute flank pain. J Urol. 2002;167:1687-91.
- [Google Scholar]
- Low-dose and standard-dose unenhanced helical computed tomography for the assessment of acute renal colic: prospective comparative study. Acta Radiol. 2005;46:756-63.
- [Google Scholar]
- Low-dose nonenhanced helical CT of renal colic: assessment of ureteric stone detection and measurement of effective dose equivalent. Radiology. 2000;215:51-4.
- [Google Scholar]
- Unenhanced helical CT using increased pitch for suspected renal colic: an effective technique for radiation dose reduction? J Comput Assist Tomogr. 2000;24:795-80.
- [Google Scholar]
- Abdominal plain film in patients admitted with clinical suspicion of renal colic: should it be replaced by low-dose computed tomography? Urology. 2006;67:64-8.
- [Google Scholar]
- Low-dose unenhanced multidetector CT of patients with suspected renal colic. AJR Am J Roentgenol. 2003;180:305-11.
- [Google Scholar]
- Does ultra-low-dose CT with a radiation dose equivalent to that of KUB suffice to detect renal and ureteral calculi? J Comput Assist Tomogr. 2006;30:44-50.
- [Google Scholar]
- International Electrotechnical Commission. Particular requirements for the safety of X-ray equipment for computed tomography: amendment I, 2002-09. Geneva, Switzerland: International Electrotechnical Commission; IEC 60601-2-44;
- [Google Scholar]
- Effective dose equivalents, HE, in diagnostic radiology. Med Phys. 1990;17:998-1003.
- [Google Scholar]
- The value of unenhanced helical computerized tomography in the management of acute flank pain. J Urol. 1998;159:735-40.
- [Google Scholar]
- Clinical practice: acute renal colic from ureteral calculus. N Engl J Med. 2004;350:684-93.
- [Google Scholar]
- Preoperative evaluation of live renal donors using multislice CT angiography. Clin Radiol. 2005;60:771-7.
- [Google Scholar]
- The pattern of renal vessels in live related potential donors pool. A multislice computed tomography angiography review. Saudi Med J. 2006;27:841-4.
- [Google Scholar]
- Three-dimensional synchronized multidirectional renal pyelo-angiography: a new imaging concept to facilitate percutaneous nephrolithotomy in technically challenging cases. J Endourol. 2009;23:1937-9.
- [Google Scholar]




