
Translate this page into:
Tuberculosis - The usual suspect
*For correspondence: drmalli_arjun@yahoo.co.in
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 45 year old female patient presented to the Gastroenterology outpatient department at St John's Medical College Hospital, Bengaluru, India, in May 2013 with a history of progressive dysphagia for solids since one month. The clinical examination was unremarkable. Investigations revealed haemoglobin 10 g/dl, ESR of 95 mm/h, and normal chest X-ray. Endoscopy showed an ulcer with undermined edges and fistulous opening in the mid oesophagus. (Fig. 1). Histopathology of oesophageal ulcer showed confluent granulomas with acid fast bacilli (AFB) (Fig. 2). CT scan chest showed mediastinal lymph nodes with fistulous tract into the oesophagus (Figs 3, 4). The patient was treated with antituberculosis drugs, and became asymptomatic after two months. Oesophageal tuberculosis masquerades as carcinoma at presentation, which often occurs due to spread from adjacent structures. Endoscopic biopsies usually demonstrate classic granulomas in about half of the cases.
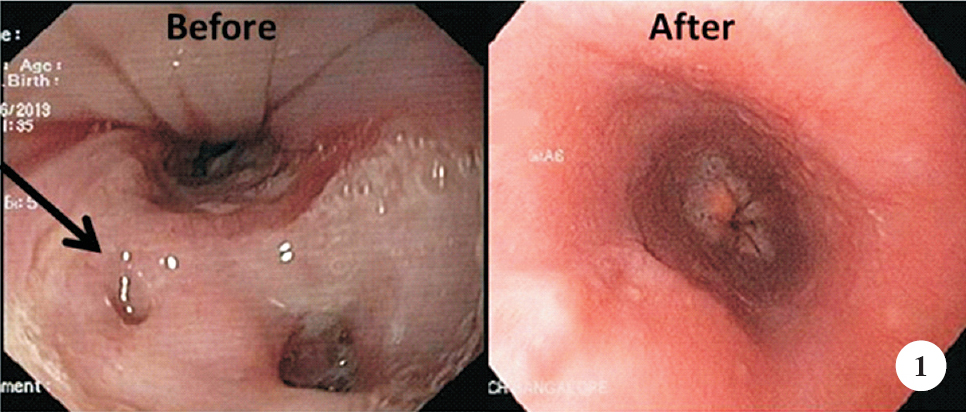
- Endoscopy showing a linear clean based ulcer with undermined edges and fistulous opening in the mid oesophagus (arrow) before treatment and a later image showing completely healed ulcer.
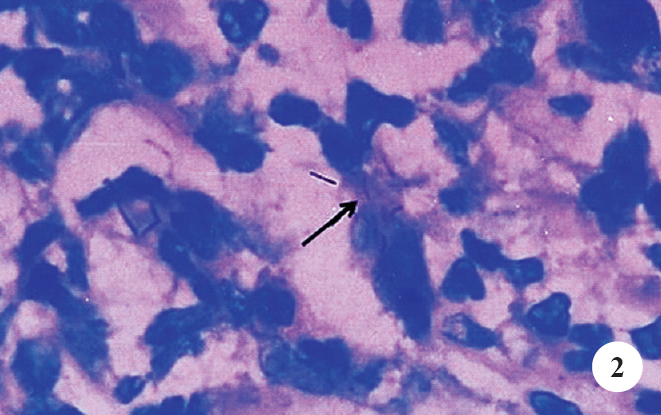
- Histopathology of oesophageal ulcer biopsy with Ziehl-Neelsen stain showing (arrow) acid fast bacilli (100 x).
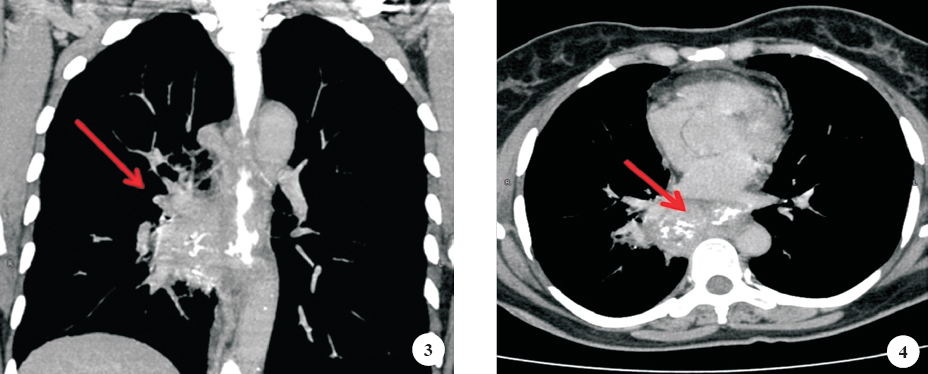
- CT scans showing (arrow) well-defined enhancing mid paraesophageal lesion with evidence of a fistulous tract between the oesophagus and right mid paraesophageal irregular cavity.




