
Translate this page into:
‘Silent’ putty kidney
* For correspondence: stephensailo@gmail.com
-
Received: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 35 yr old male† presented to the department of Urology, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, India, in April 2019, with a three month history of pain on the right side of the chest after blunt trauma. He suffered from pulmonary tuberculosis 15 years ago and had completed a full course of anti-tubercular drugs. There were no symptoms suggestive of renal tuberculosis. He was normotensive and physical examination was unremarkable. Chest X-ray and urinalysis were also normal. The plain radiograph, however, showed dense reniform opacity in the region of the right kidney (Fig. 1).

- Plain radiograph showing dense reniform opacity (arrow) in the right renal area.
Ultrasonography detected a contracted and echogenic right kidney (6.6 × 3.0 cm), with a strong acoustic shadow (Fig. 2). Intravenous urogram (Fig. 3) and renal scintigram (Fig. 4) demonstrated a non-functioning right kidney (‘putty kidney’). The patient was reassured and advised to undergo nephrectomy if he becomes symptomatic.
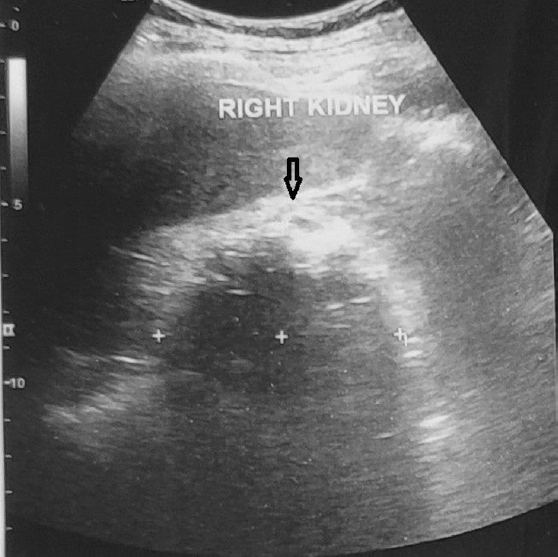
- Contracted and echogenic right kidney (arrow) detected on ultrasound.

- Intravenous urogram (20-min film) revealing completely calcified and non-functioning right kidney (arrow) and normal left kidney.
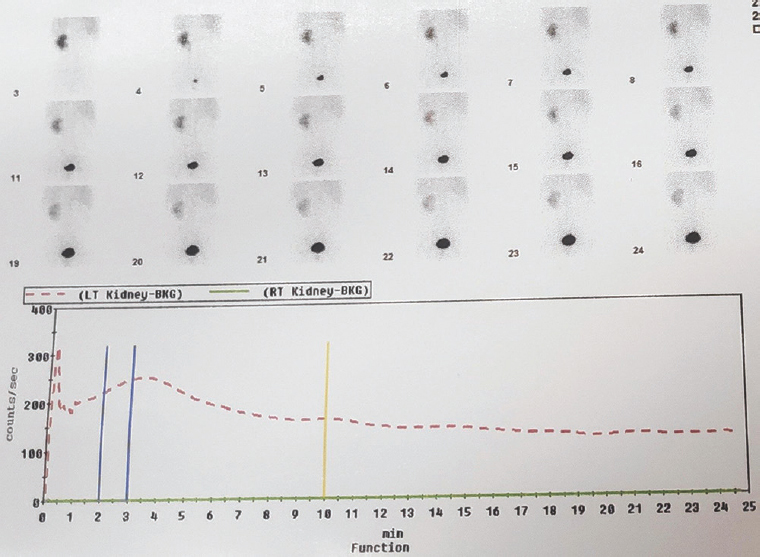
- Renal scintigram (99m Tc-DTPA) showing non-functioning right kidney.
Renal tuberculosis is secondary to pulmonary tuberculosis. Rarely, the affected kidney is completely calcified and damaged (‘autonephrectomy’). Patients with renal tuberculosis may have minimal symptoms and sometimes may be asymptomatic (silent) as in the present case. Patients with a history of pulmonary tuberculosis should, hence, be screened for renal tuberculosis for the early diagnosis and prevention of renal damage.




