
Translate this page into:
Re-establishment of normal radioactive iodine uptake reference range in the era of universal salt iodization in the Indian population
Reprint requests: Dr Chandrasekhar Bal, Department of Nuclear Medicine, Thyroid Clinic, All India Institute of Medical Sciences, Room No. 59-A, Ansari Nagar, New Delhi 110 029, India e-mail: csbal@hotmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
The reference radioactive iodine uptake (RAIU) values established in the 1970s in the era of widespread iodine deficiency were relatively high. Now, after four decades of successful Universal Salt Iodization (USI) programme in India, there is a need to re-establish these reference ranges. The present study was aimed to quantify the two-hour and 24-h RAIU values in iodine sufficient euthyroid individuals and validate the results in Graves’ and Hashimoto's thyroiditis patients.
Methods:
In this prospective study conducted from April 2012 to September 2013, euthyroid volunteers who consented for the investigations were enrolled in the study. Treatment-naive Graves’ disease and Hashimoto's thyroiditis patients were recruited from the outpatient clinic. The investigations included neck ultrasonography, thyroid function tests, thyroglobulin (Tg), anti-Tg and anti-thyroid peroxidase antibody and urinary iodine concentration.
Results:
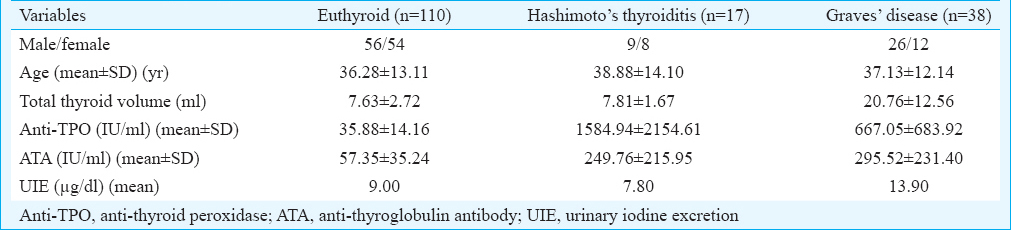
Three different groups comprising 110 euthyroid volunteers, 38 Graves’ and 17 Hashimoto's thyroiditis patients were enrolled in the study. The mean 2-h RAIU values for the euthyroid group, Hashimoto's thyroiditis and Graves’ patients were 3.83±2.77, 4.22±3.41 and 32.67±15.93 per cent, and mean 24-h RAIU values were 12.75±5.51, 11.66±9.55 and 61.85±12.9 per cent, respectively. The mean thyroid volumes were 7.63±2.72, 7.81±1.67 and 20.76±12.56 ml for the euthyroid, Hashimoto's thyroiditis and Graves’ disease groups and the mean spot urinary iodine concentrations were 9.0, 7.8 and 13.9 µg/dl in the three groups, respectively. The new reference range (95% confidence interval) for two-hour was 1-7 per cent and 24-h was 7-18 per cent.
Interpretation & conclusions:
Compared to the previous values, there was a considerable decrease in the RAIU values in euthyroid individuals. This was further corroborated with increase in the urinary iodine concentration and decrease in thyroid volume, attributed to successful USI programme. Further studies with a large sample from different parts of India need to be done to confirm these findings.
Keywords
Euthyroid
iodine
radioactive iodine uptake
re-establishment
reference range
thyroid
universal salt iodization

The classic radioactive iodine uptake (RAIU) test is advised, particularly, in the differential diagnosis of thyrotoxicosis. In a clinically suspected and biochemically confirmed thyrotoxic patient, it is an accepted fact that increased uptake in the thyroid gland suggests hyperthyroidism while decreased uptake predominantly indicates conditions, namely, sub-acute thyroiditis (de Quervain's thyroiditis or viral thyroiditis), Hashimoto's thyroiditis (chronic lymphocytic thyroiditis), drug interference, or extra-thyroidal cause of thyrotoxicosis, etc. In healthy individual, RAIU values vary with the iodine reserves in the thyroid gland that depend directly on the long-term dietary intake of iodine12. As there exists geographical variations in the dietary iodine content, the RAIU values are expected to vary accordingly3. Hence, it is important to establish the local RAIU reference values for correct diagnosis of various thyroid diseases and the accurate interpretation of laboratory reports.
At All India Institute of Medical Sciences (AIIMS), New Delhi, India the reference RAIU values (24 h=15-50%) were established in the 1960s when there was widespread iodine deficiency4. With the initiative of the Government of India, Universal Salt Iodization (USI) programme was started in 1989 and as a result the prevalence of iodine deficiency disorders decreased considerably5. Given the achieved iodine sufficiency in India6, the normal RAIU values are expected to be much lower than those established earlier. Using the current RAIU reference values, it is possible that many patients with upper normal RAIU values are misdiagnosed as being normal. Therefore, there is a need to re-establish the RAIU reference range in the iodine sufficiency era.
Thus, this study was aimed at assessing the 2-h and 24-h RAIU values in the euthyroid individuals to establish new reference range. The secondary objective was to validate the reference values in newly diagnosed Graves’ disease and Hashimoto's thyroiditis patients where high and low-to-normal uptakes are expected, respectively.
Material & Methods
This was a prospective study conducted jointly by the departments of Nuclear Medicine, Endocrinology and Radiology, AIIMS, New Delhi, between April 2012 and September 2013. Healthy volunteers were invited to participate in the study. A healthy volunteer was defined as an individual not known to have prior clinical history of thyroid disorders or under treatment for the same. A total of 132 individuals gave consent for participation. All the individuals filled a questionnaire, before any test was administered, pertaining to recent iodine contamination, such as ingestion of drugs affecting the thyroid function or a recent (within 8 wk) contrast-enhanced radiological procedure performed. The study was approved by the Institutional Ethics Committee, and informed written consent was obtained from all the individuals above 18 years of age.
The individuals who were enrolled for the investigations underwent neck ultrasonography (USG), serum triiodothyronine (T3), tetraiodothyroxine (T4), thyroid-stimulating hormone (TSH), thyroglobulin (Tg), anti-Tg antibody (ATA), anti-thyroid peroxidase antibody (anti-TPO) and urinary iodine estimation (UIE). Clinically, individuals with normal biochemical investigations (T3, T4, TSH, Tg, ATA, anti-TPO) and normal echotexture and no abnormal nodularity in thyroid in USG were classified as euthyroid and included in the study. Subsequent to these investigations, 13 had elevated mean anti-TPO levels of 165 (0-65) IU/ml, of whom seven individuals were found to have raised mean serum TSH level of 14 (range: 0.17-4.0) mIU/l. These 13 volunteers were excluded for RAIU tests because of abnormalities in the thyroid function tests. On USG of thyroid gland, six individuals had heterogenous echotexture of the thyroid gland and three had sub-centimetre thyroid nodules. These nine individuals were also excluded from RAIU tests.
The minimum required sample size was determined using an appropriate formula by taking the level of significance (α) of 0.07, power of the study (1-ß) to be 80 per cent; approximately 84 individuals were required to be recruited in this healthy volunteer group. Finally, 110 healthy volunteers were enrolled for the RAIU who fulfilled all inclusion and exclusion criteria. The validation groups, clinically and biochemically confirmed newly diagnosed cases of Graves’ disease (n=38) and Hashimoto's thyroiditis (n=17) patients, those who consented to be included in the study, were selected from the outpatient clinic.
Thyroid ultrasonography (USG): Determination of thyroid volume was done by high-resolution LOGIQ E9 USG machine (GE Healthcare, Chicago, USA) with a linear transducer of 11 MHz frequency for patients in each group before radioiodine (131I) administration. All conventional parameters such as echogenicity, echotexture and size were analyzed in each of the three groups. The colour Doppler was also used in the three groups. The formula of Brunn et al7 was applied for sonographic estimation of total thyroid volume. In brief, the volume of each thyroid lobe=length × breadth × height × 0.5, and total thyroid gland volume was addition of both lobes.
Hormone assays: Hormone assays were performed in all individuals before RAIU and in disease groups at three-month follow up. The laboratory reference ranges: TSH, 0.17-4.0 mIU/l; total T4, 4.5-12.5 ug/dl; total T3, 70-200 ng/dl (Immunotec, California); Tg, undetecTable -52 ng/ml (Diametra, Italy); ATA, 0-125 IU/ml; and anti-TPO, 0-65 IU/ml (Hycor, United Kingdom). T3, T4 and TSH were assayed by classic radioimmunoassay techniques8. ATA, anti-TPO and Tg were assayed by enzyme-linked immunosorbent assay (ELISA) methods (Thermo Fisher Scientific, USA).
Urinary iodine estimation (UIE): UIE was performed by ion selective electrode (Thermo Fisher Scientific, USA) in all individuals for the iodine status. Initially, before sample measurements, standardization of the electrode was done. From stock solution, 0.79 ml of iodide standard was taken in a flask and diluted with 100 ml distilled water and mixed well. By serial dilution of stock solution 10 ppm (1000 µg/dl), 1 ppm (100 µg/dl) and 0.1 ppm (10 µg/dl) concentrations of standard iodine solutions were prepared. In this study, the normal reference limit of 10 µg/dl, adopted from the WHO global database9, was followed for urinary iodine excretion.
Preparation of iodide combination electrode: The iodide combination electrode was prepared and flushed before use. The electrode (Thermo Fisher Scientific, USA) was passed by flushing, filling solution along its length. The electrode was filled with distilled water and drained from its chamber. Finally, the electrode was filled with fresh filling solution up to the fill hole. The electrode was ready for use to measure the standards followed by the samples.
Direct calibration technique: In the direct calibration procedure, a calibration curve was constructed in the metre memory. The electrode potentials of standard solutions were measured and plotted on the linear axis against their concentrations on the log axis. The resulting slope value was recorded. Fifty millilitres of each 10, 1 and 0.1 ppm concentrations were collected in separate falcons. Two per cent of adjuster was added into each falcon and mixed well. Each of these samples was measured in the calibration procedure and a slope was created. The ideal slope create was between a range of 50-60 mV. Subsequently, urine samples as the volume of the standards were used for analysis in the volunteers and in the patients.
Radioiodine uptake (RAIU): All those individuals who had normal parameters of USG, laboratory tests, UIE and also Graves’ and Hashimoto's thyroiditis patients who gave consent were included and underwent RAIU study. Liquid 131I was procured from the Board of Radiation and Isotope Technology, India. All patients were advised to remain empty stomach two hours prior and after the administration of 131I dose. Graves’ disease patients were advised to stop anti-thyroid drugs 2-4 days and Hashimoto's patients who were on levothyroxine were advised to stop it for 4-6 wk before the test10. All Graves’ disease patients who were referred for 131I therapy underwent RAIU both before 131I therapy as well as on three-month follow up. The liquid 131I [185 kBq (5 uCi)] was administered orally. Atomlab 950 (Biodex, USA) thyroid uptake probe was used for RAIU estimation at 2 and 24-h, with pulse height analyzer setting such that the window width was set at 309-420 KeV and the photopeak was set at 364 KeV. The uptake probe was placed at a distance of 25 cm in front of the neck such that the entire thyroid gland was included within the iso-centric field of the probe. Counts were taken from the background, standard sample placed in the International Atomic Energy Agency, Vienna, thyroid neck phantom, subject's neck and thigh for a time period of one minute each. The percentage RAIU values at the specific time intervals were calculated using the formula: RAIU=(neck counts per minute − thigh counts per minute)/(standard counts per minute − background counts per minute) × 100 per cent.
Statistical analysis: The clinical parameters were analyzed for mean, standard deviation and range. Univariate analysis using Student's t test was used to compare any two groups. P<0.07 was considered significant. Stata 11.2 (StataCorp, College Station, TX, USA) was used for analysis.
Results
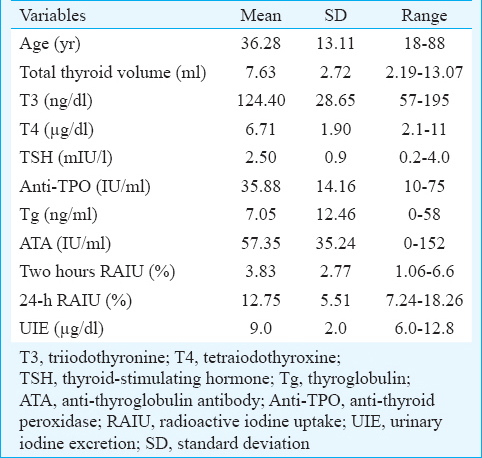
The demographic profile of the patient groups is summarized in Table I. The laboratory data of all euthyroid individuals are depicted in Table II. The reference range was calculated from 110 individuals with normal thyroid function tests and without any structural abnormalities of the thyroid gland. The mean RAIU values at 2- and 24-h for the euthyroid individuals were 3.8±2.8 and 12.8±5.5 per cent, respectively. The 2-h RAIU 95 per cent confidence interval (CI) was estimated to be 1.1-6.6. Similarly, the 24-h RAIU 95 per cent CI values for the euthyroid individuals ranged between 7.2 to 18.3 per cent. The mean Tg level of euthyroid individuals was within the normal limits and was found to be 7.05 ng/ml (0-58). The mean thyroid volume was 7.63±2.7 ml.
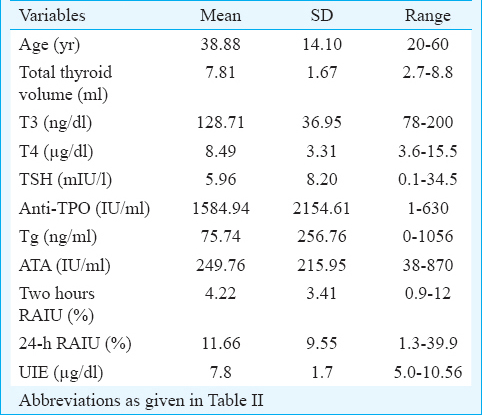
Hashimoto's thyroiditis patients: The demographic and laboratory data of Hashimoto's thyroiditis patients are depicted in Table III. All Hashimoto's thyroiditis patients had a mean T3, T4 and TSH of 128.71 ng/dl, 8.49 µg/dl and 5.96 mIU/l, respectively. Mean anti-TPO and ATA antibody levels were 1584.94 IU/ml and 249.76 IU/ml, respectively. Mean Tg was 75.74 ng/ml. Mean RAIU uptake value at 2-h was 4.22±3.41 per cent, ranging from 0.9 to 12 per cent. The mean 24-h RAIU uptake was 11.7±9.6 per cent (range, 1.3-39.9%). USG of the thyroid gland showed diffusely enlarged, coarsened, hypoechoic and mildly hypervascular pattern, with a mean thyroid volume of 7.81 ml.
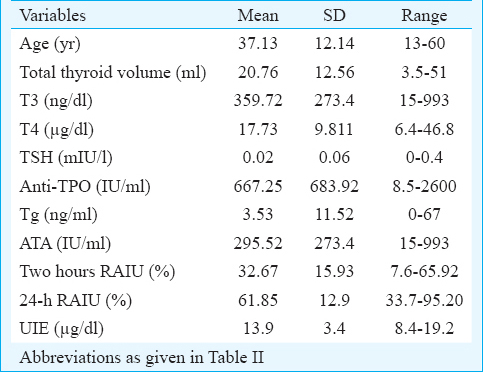
Graves’ disease patients: All patients with Graves’ disease had high mean serum T3 and T4 levels of 359.72 ng/dl and 17.73 µg/dl, respectively and suppressed mean serum TSH of 0.02 mIU/l. Table IV depicts the detailed profile and laboratory data of this group of patients. Most of the patients had high titres of anti-TPO and ATA. The mean anti-TPO was 667.25 IU/ml and mean ATA was 295.52 IU/ml. The mean 2-h and 24-h RAIU values were 32.7±15.9 per cent and 61.9±12.9 per cent, respectively. The mean RAIU values at 2-h and 24-h in Graves’ disease patients were significantly higher than in the euthyroid patients as well as in the Hashimoto's thyroiditis patients (P<0.001). USG showed bilaterally enlarged gland, heteroechoic and increased vascularity, with a mean thyroid volume of 20.76 ml.
Discussion
Entry of iodine into the follicular cell of thyroid is facilitated through the transmembrane protein called sodium iodide symporter (NaI-symporter). TSH is the most important tropic hormone for stimulation of thyroidal uptake of sTable iodine by upregulating the NaI-symporter11. Iodine deficiency status leads to increased TSH levels to maintain the circulating levels of T4 within normal limits which in turn stimulate the increased uptake of sTable/radioactive iodine whenever it is administered12. In the era of iodine deficiency, raised TSH stimulates the proliferation of the gland leading to large diffuse goitre and long-standing goitre leads to multi-nodularity. The uptake of radioiodine was high due to the fact that thyroid gland is depleted of intra-thyroidal iodine reserve leading to increased uptake.
With the gradual alleviation of the iodine deficiency, there is a need to re-establish the RAIU reference values periodically313. The periodic reassessment is essential not only in the iodine-deficient regions that are gradually moving towards iodine sufficiency but also in the iodine sufficient areas as changes in the dietary iodine consumption are known to fluctuate with time in the regions with high iodine intake as well14.
Ahuja et al15 in 1974 reported in normal healthy individuals, 24-h RAIU to be 51.1 per cent. Nearly a decade after the USI implementation, Moorthy et al13 in 2001 estimated the mean 24-h RAIU in healthy euthyroid individuals to be 19.1±8 per cent. It was significantly lower than the one reported earlier in 197415. The 24-h mean RAIU value was 12.8 per cent observed in the present study, lower as compared to 2001 study13, indicating the residual iodine deficiency has been mitigated.
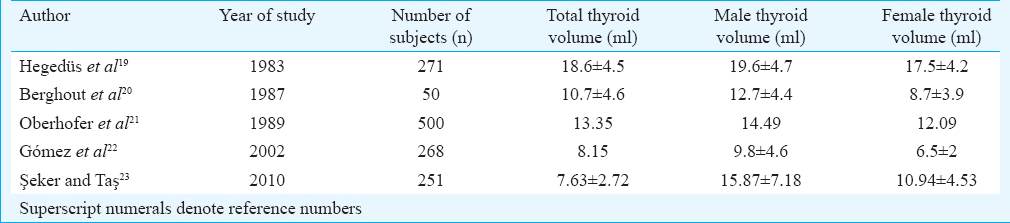
The RAIU values in the present study were comparable with studies reported from iodine sufficient countries of the world161718. For example, a previous study from Alabama, the United States of America, reported a drop in the mean 24-h RAIU values from 28.6 per cent in 1959 to 15.4 per cent in 1967-1968 and explained that the decline was caused by the sufficient dietary intake of iodine in the latter period17. The thyroid volume is a surrogate marker for iodine status in the population. Table V shows a comparison of thyroid volume as reported in various studies from different countries. The mean thyroid volume has been considerably decreased in size, reflecting the dietary iodine sufficiency status, in general population1920212223.
The urinary iodine concentration is the direct measure of dietary iodine intake. In the present study, the concentration was found to be higher than the previous studies from India1315. It was inferred that with increase in dietary consumption of iodine, there was a decrease in the RAIU values, decrease in mean thyroidal volume and a parallel increase in the urinary iodine concentration.
Despite the variation in the RAIU values and the urinary iodine concentrations, the values of serum T3, T4 and TSH in the euthyroid individuals were comparable with those reported in the previous studies from India1324. This can be explained by the pituitary-thyroid axis, being in the autoregulation mode, adjusts to the environmental changes and hormonal needs of the individual.
Milakovic et al2 from Sweden reported the effect of long-term iodine supplementation on thyroid 131 I uptake. There was a significant decrease in the uptake in euthyroid individuals but not in hyperthyroid individuals as compared to observations 50 years ago. In our study also there was a significant decrease in the 24-h RAIU values in the healthy euthyroid individuals but not in Graves’ disease patients.
During 2012-2013 the database of hyperthyroid patients of thyroid clinic, in the Department of Nuclear Medicine, AIIMS, was analyzed to validate our results. Among a total of 532 biochemically hyperthyroid patients, 22 (4%) patients had 24-h RAIU range of 19-35 per cent in spite of being biochemically hyperthyroid (mean serum TSH 0.22 mIU/l, range: 0-0.004 mIU/l). In these set of patients, radioiodine therapy would not be recommended if the previously established 24-h reference values were followed, though having biochemically toxic profile. However, with the present re-established 24-h RAIU values, radioiodine therapy was recommended in the above patients. Following therapy, all the patients responded and had normal biochemical profiles.
In conclusion, the 24-h RAIU reference interval for the healthy euthyroid individuals in the present study was 7.2-18.3 per cent with 12.8 per cent as the mean uptake. These values were considerably lower than the previously published reference values from India and were comparable with the RAIU values in most of the iodine-sufficient regions of the world. Thus, the current normal RAIU reference range may be used for clinical purposes. However, the sample size of the current study was small; hence, larger sample size would be required from different parts of India to re-establish the RAIU normogram.
Acknowledgment
This study was funded by an intramural research grant from AIIMS, New Delhi (No: A-119) to the third author (CSB).
Conflicts of Interest: None.
References
- Thyroid radioiodine uptakes and scans in euthyroid patients. Mayo Clin Proc. 1975;50:79-84.
- [Google Scholar]
- Effect of lifelong iodine supplementation on thyroid 131-I uptake: A decrease in uptake in euthyroid but not hyperthyroid individuals compared to observations 50 years ago. Eur J Clin Nutr. 2006;60:210-3.
- [Google Scholar]
- Iodine deficiency disorders (IDD) control in India. Indian J Med Res. 2013;138:418-33.
- [Google Scholar]
- A correlative study of histopathological features with some immunological tests in thyroid disease [MD Dissertation]. New Delhi: All India Institute of Medical Sciences; 1965.
- Prevention of endemic goitre with iodized salt. Bull World Health Organ. 1973;49:307-12.
- [Google Scholar]
- Relevance and importance of universal salt iodization in India. Natl Med J India. 1997;10:290-3.
- [Google Scholar]
- Volumetric analysis of thyroid lobes by real-time ultrasound (author's transl) Dtsch Med Wochenschr. 1981;106:1338-40.
- [Google Scholar]
- Laboratory evaluation of thyroid function. J Assoc Physicians India. 2011;59(Suppl):14-20.
- [Google Scholar]
- Assessment of iodine deficiency disorders, and monitoring their elimination. In: A guide for program managers. Geneva: WHO; 2001. p. :1-122.
- [Google Scholar]
- Society of Nuclear Medicine Procedure Guideline for Thyroid Uptake Measurement. 2006. Ver. 3. Thyroid Uptake, SNM;. :1-4. Available from http://snmmi.files.cms-plus.com/docs/Thyroid%20Uptake%20Measure%20v3%200.pdf
- [Google Scholar]
- Thyroid Hormone Synthesis: Thyroid iodide transport. In: Braverman LE, Cooper DS, eds. Werener & Ingbar's the thyroid a fundamental and clinical text. Philadelphia: Lippincott Williams & Wilkins; 2013. p. :32-47.
- [Google Scholar]
- Iodine deficiency and endemic cretinism. In: Braverman LE, Cooper DS, eds. Werener & Ingbar's the thyroid a fundamental and clinical text. Philadelphia: Lippincott Williams & Wilkins; 2013. p. :217-241.
- [Google Scholar]
- Radioiodine kinetics and thyroid function following the universal salt iodization policy. Natl Med J India. 2001;14:71-4.
- [Google Scholar]
- Iodine nutrition in the United States. Trends and public health implications: Iodine excretion data from National Health and Nutrition Examination Surveys I and III (1971-1974 and 1988-1994) J Clin Endocrinol Metab. 1998;83:3401-8.
- [Google Scholar]
- Thyroid hormonogenesis in sporadic euthyroid goitre. Indian J Med Res. 1974;62:1387-91.
- [Google Scholar]
- Changing normal values for thyroidal radioiodine uptake. N Engl J Med. 1969;280:1431-4.
- [Google Scholar]
- Patterns of thyroid radioiodine uptake. Jordanian experience. J Nucl Med Technol. 2010;38:32-6.
- [Google Scholar]
- The determination of thyroid volume by ultrasound and its relationship to body weight, age, and sex in normal subjects. J Clin Endocrinol Metab. 1983;56:260-3.
- [Google Scholar]
- Determinants of thyroid volume as measured by ultrasonography in healthy adults in a non-iodine deficient area. Clin Endocrinol (Oxf). 1987;26:273-80.
- [Google Scholar]
- Thyroid gland volumes of healthy adults in an area with endemic goiter. Acta Med Austriaca. 1989;16:38-41.
- [Google Scholar]
- Pituitary-thyroid axis, thyroid volume and leptin in healthy adults. Horm Metab Res. 2002;34:67-71.
- [Google Scholar]
- Determination of thyroid volume and its relation with isthmus thickness. Eur J Gen Med. 2010;7:125-9.
- [Google Scholar]
- Quantitative aspects of iodine metabolism in simple goitre seen in Delhi and neighbouring areas. J All India Inst Med Sci. 1977;3:159-64.
- [Google Scholar]




