Translate this page into:
More blood, more life? Reflections on World Blood Donor Day – 2011
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications and was migrated to Scientific Scholar after the change of Publisher.
Previously commemorated by the International Federation of Blood Donor Organisations (IFBDO), the World Blood Donor Day has now been adopted by the World Health Organization (WHO) to recognise the contribution of blood donors to world health. Public recognition of blood donors is a strong motivator for donation1. In itself, it may be considered as an incentive and an example of ‘impure’ altruism2, sitting somewhat uneasily in the landscape of ‘voluntary, unpaid’ blood donation which appears to be, at the expense of any alternative, the sole donation route accepted by the WHO. It is fitting that blood donors are recognised, because blood-derived therapies continue to be a life-saving medical intervention in many instances. It is important, however, to reflect on the current state of the field of haemotherapy, if the role of donors is to be properly recognised. The past fifty years have seen blood transfusion shift in status in the established Western economies, from a modest medical technology to an alleged speciality ‘Transfusion Medicine’ (TM). TM may be viewed as a paradigm as described by Kuhn3, characterised by an unquestioned acceptance of its basic tenets yet containing tensions which may eventually lead to its replacement. Perhaps, the most significant component of the TM paradigm, in terms of these tensions, is the detachment, despite the term ‘Transfusion Medicine’, of transfusion from the direct medical interphase. TM has been replaced by a manufacturing construct, in which blood is viewed as a raw material for the extraction of various fresh components for immediate transfusion, principally red cells. The primary event which caused this replacement in the Western world was the discovery in 1964, that cryoprecipitate made in blood banks could provide an effective treatment for haemophilia4. This led to a rapid conversion of whole blood units to >95 per cent red cells, as more and more plasma was generated for cryoprecipitate. Thus the needs of a tiny, vulnerable but, suddenly, eminently treatable portion of the haemo-recipient community shaped the whole of blood transfusion. This event was doubtlessly influenced by the relative helplessness which transfusion experts felt in the early 1960s when facing the huge mortality of their other recipient groups such as leukemics and thallassaemics. The rapid conversion of blood banks to a pharmaceutical environment owes more to this development than to any other.
The extinction of ‘blood transfusion’ in the established economies is now proposed as the way forward for the developing world; the WHO strongly advocates centralised blood centres, component therapy and fractionation of recovered plasma as the only template5. Presumably these features are found in the blood services declared by the WHO to be the best in the world, although no indication of what leads to this accolade is otherwise found in the WHO's statements.
These features are also systematically sold to donors, through messages such as – ‘One donation saves many lives’6 etc. The implied link between component therapy and optimised inventory is not borne out by evidence. Yet tensions in this TM paradigm are emerging. Currently, the possible morbidities associated with the transfusion of stored red cells7 and the clinical benefits of whole blood transfusion8 are throwing doubts on the advisability of universal component therapy. The flimsy evidence base for components has been challenged9 and is not underpinned by regulatory scrutiny and approval of therapeutic claims. On the other hand, the protein therapies extracted from plasma serve established deficiencies such as haemophilia and immune deficiency through evidence based approval to market. In the established economies, component usage has flattened and dropped off in many countries, while the usage of protein therapies, particularly immunoglobulin (Ig), continues to increase.
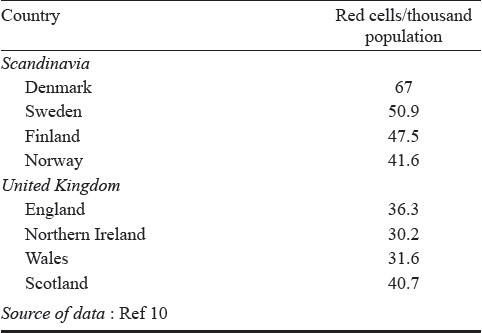
Hence, basing a policy for the optimal provision of all haemotherapies on collecting more and more blood (which appears to underpin most of the donor management programmes worldwide and resonates in the message of each World Blood Donor Day), may not be the best way forward for emerging countries. The risk of over-collection and wastage of red cells on one hand, and of inadequate provision of protein therapies on the other, should give pause for reflection. Given the flimsy evidence base for red cell transfusion, the hugely variable red cell usage rates between countries with similar health systems10 (Table I) are not to be wondered at. Uncertainty around the target red cell collection rate is best addressed through a critical assessment of clinical needs, not through continued calls to collect more blood. Given the capacity of modern medicine to deliver bloodless surgery and complex transplant procedures for Jehovah's Witnesses, can we justify the continuous calls to replicate the ‘blood empires’ of the West?
And this brings us back to the donors. Blood and plasma donation is undertaken for a wide and complex variety of motives, and is drawn from different demographic groups. The educated middle class is the predominant demographic for whole blood donation in the established economies11. In such countries, this social group is large enough to supply most of the fresh component needs of their societies through their overall modest gift – few countries achieve whole blood donation rates exceeding two units/donor/year. This demographic, occupying the upper levels of Maslow's Hierarchy of Needs12, derives utility through self-esteem, achievement, respect, etc. Their economic needs are met; they do not have to worry excessively about the needs reflected lower down in the Marlow pyramid (Fig. 1). In these groups, donation has been shown to increase with increased public recognition1, resulting in status which can be more important than material incentives13.
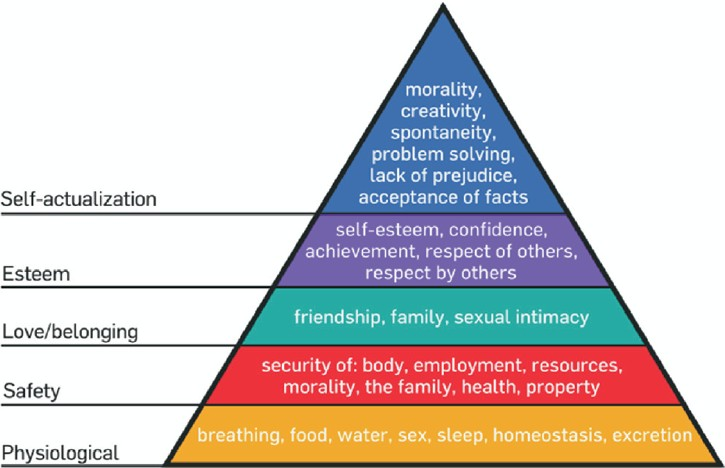
- Maslow's hierarchy of needs.
Clearly, this demographic is smaller in less affluent societies, whose social groups embedded in the middle parts of Marlow's pyramid predominate. For these groups, the needs of friendship, family, health, etc. are important. Here we may gain an understanding of the importance of replacement whole blood donors in these societies, exemplified by sub-Saharan Africa. The safety of such donors has been demonstrated14 but what is considered more important is the need to recognise that their role is a reflection of the socio-economic profile of these countries. Insisting that these societies convert their donor populations to the ‘western’ demographic of the educated middle class is unrealistic and ignores the basic fundamental features of such societies. Curtailing their contribution is clearly detrimental to patient welfare, and negates their valid position in the blood supply.
As outlined above, while red cell usage in the established countries decreases15, the demand for plasma protein therapies continues to rise (Fig. 2). An estimate of needs for evidence based indications demonstrates that these cannot be met through the generation of plasma from whole blood16. The volumes of plasma needed require recourse to frequent plasmapheresis of committed donors. The experience worldwide is that this cannot be achieved through the ‘voluntary’ system. Some countries have made significant progress in generating plasma by apheresing their mainstream donor population – Australia and The Netherlands are notable examples. However, the world supply of marketed plasma products still depends on the plasma generated from compensated donors, predominantly the one million compensated plasma donors of the United States. The need to return for a time consuming and arduous plasmapheresis repeatedly for many weeks breaches the ‘compassion threshold’ of the Western middle class whole blood demographic. It should not be a matter of shame or controversy that such plasma donors are more likely to be found in the lower sections of Marlow's hierarchy17. Clearly such individuals are unlikely to be able to afford the luxury of competing for esteem and recognition, but drawing them into the plasma supply environment through material compensation should be recognised as a beneficial engagement of an otherwise untapped demographic.
Drawn from these different demographic groups, the donors of haemotherapies have two things in common – they all save lives, and they all deserve recognition and protection. The continued exclusion of compensated plasma donors from the scope of World Blood Donor Day is unjustified, given the superior evidence base and the unquestioned efficacy of plasma protein therapies, which save the lives of thousands of vulnerable patients. Replacement donors make an essential contribution to the blood supply in emerging countries and their dismissal by the WHO is not constructive. All these groups are united in saving lives, and authorities should unite in recognising all of them. They all need to be protected from the possible adverse effects of donation, whether it be protein depletion18 or the studiously under-exposed issue of iron deficiency19.
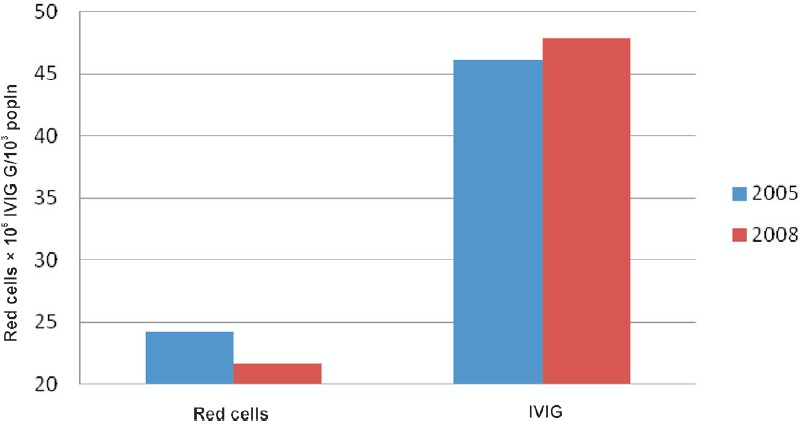
- Red cell and intravenous immunoglobulin (IVIG) use in the UK.
If TM is to live up to its status, more needs to be done to manage and recognise the very basis of its being – blood and plasma donors worldwide.
References
- Social Image Concerns and Pro-Social Behavior. Institute for the Study of Labor. 2008. Available from: http://ftp.iza.org/dp3771.pdf
- [Google Scholar]
- Impure altruism and donations to public goods: a theory of warm-glow giving. Econ J. 1990;100:464-77.
- [Google Scholar]
- The structure of scientific revolutions. Chicago (IL): University of Chicago Press; 1962.
- [Google Scholar]
- high-potency antihaemophilic factor concentrate prepared from cryoglobulin precipitate. Nature. 1964;203:312.
- [Google Scholar]
- World Health Assembly 2010. Availability, safety and quality of blood products. Available from: http://apps.who.int/gb/ebwha/pdf_files/EB126/B126_R14-en.pdf
- [Google Scholar]
- American Red Cross. Blood facts and statistics. Available from: http://www.redcrossblood.org/learn-about-blood/blood-facts-and-statistics
- [Google Scholar]
- Current issues relating to the transfusion of stored red blood cells. Vox Sang. 2009;96:93-103.
- [Google Scholar]
- Warm fresh whole blood is independently associated with improved survival for patients with combat-related traumatic injuries. J Trauma. 2009;66(Suppl 4):S69-76.
- [Google Scholar]
- European directorate of quality of medicines and Healthcare Council of Europe. The collection, testing and use of blood and blood components in Europe - 2006 Report. Available from: http://www.edqm.eu/medias/fichiers/The_Collection_Testing_and_Use_of_Blood_and_Blood_1.pdf
- [Google Scholar]
- Relative safety of first-time volunteer and replacement donors in West Africa. Transfusion. 2010;50:340-3.
- [Google Scholar]
- Serious Hazards of Tranfusion (SHOT) Annual Report 2009 Summary. Yearly summary of issues by the 4 UK Blood Services 1999–2009. Available from: http://www.shotuk.org/wp-content/uploads/2010/06/SHOT-2009-Summary.pdf
- [Google Scholar]
- Bad blood: the moral stigmatization of paid plasma donors. J Contemp Ethnogr. 1992;20:416-41.
- [Google Scholar]
- Specific protein content of pools of plasma for fractionation from different sources: impact of frequency of donations. Vox Sang. 2010;99:220-31.
- [Google Scholar]
- Iron and blood donation-an under-recognised safety issue. Dev Biol (Basel). 2007;127:137-46.
- [Google Scholar]




