Translate this page into:
Magnitude of pedestrian head injuries & fatalities in Bangalore, south India: A retrospective study from an apex neurotrauma center
Reprint requests: Dr Nupur Pruthi, Assistant Professor, Department of Neurosurgery, National Institute of Mental Health & Neuro Sciences, Hosur Road, Bangalore 560 029, India e-mail: pruthi_nupur@yahoo.co.in
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Pedestrians contribute to 30-40 per cent of all road traffic injuries in India. However, there is a paucity of literature on pedestrian head injury as compared to two wheeler trauma. The purpose of the present study was to study the pattern of pedestrian injuries and their outcome with a special focus on head injuries.
Methods:
The study was conducted in two parts in the Trauma Center at National Institute of Mental Health & Neuro Sciences, Bangalore. A retrospective study was conducted at the casualty services of the hospital in which 529 consecutive pedestrians who sustained injury in a road traffic accident were studied from June to September 2009. In the second part, records from the hospital mortuary were retrospectively analyzed from 2007 to 2009. An analysis of 326 patients who died as a pedestrian in road accidents during this period was performed.
Results:
Patients in both paediatric and elderly age groups constituted 47.6 per cent (252/529) of all casualty admissions. Majority of the pedestrian injuries (41.7%, 221/529) occurred between 1600 - 2100 h; 87.1 per cent of all patients received some primary care before admission. The most common offending vehicle was a two wheeler (49.1%, 260/529). At the time of admission, 55.2 per cent (292/529) patients had sustained a moderate or severe head injury (GCS 3-13), and 40.5 per cent (214/529) had an abnormal CT scan. In addition, 90.4 per cent (478/529) patients had also sustained associated injuries. Major thoracoabdominal trauma was seen in 4 per cent and spine injury in 2.3 per cent of the patients. The mortality rate was 6.6 per cent. In the postmortem group, pedestrian deaths constituted 26.2 per cent of all the postmortems conducted. Two wheelers were the offending vehicle in the majority of the fatal crashes (39.9%).
Interpretation & conclusions:
Pedestrian injuries form a major part of the workload of a neurotrauma emergency. Majority of them sustained moderate to severe head injury. More attention, infrastructure and strict implementation of rules may help reduce this burden.
Keywords
Head injuries
mortality
pedestrian trauma
postmortem
traffic injuries

Road traffic injuries account for 45-60 per cent of traumatic brain injuries in different parts of India. Pedestrians contribute to 30-40 per cent of all these injuries. A large number of road users in India are pedestrians, two-wheeler riders and bicyclists who are known to be vulnerable road users (VRUs)12. These groups of road users form the major bulk on Indian roads and hence their exposure is higher. Unlike occupants in cars and other heavy vehicles, these road users are directly exposed in traffic environments and are thus unprotected. In the event of a crash, they come in direct contact with the impacting vehicle and energy transfer is high (even in low velocity crashes) resulting in serious injuries and deaths1.
As per data from National Crime Records Bureau3, 10,125 pedestrian deaths were reported in 2007 from India. Karnataka State was one among the top 10 States (6th place) with highest number of pedestrian deaths (692)3. Bangalore is known as the Silicon Valley of India because of its position as the nations leading IT (Information Technology) exporter4. A demographically diverse city, Bangalore is a major economic and cultural hub and one of the fastest-growing major metropolises in India. However, recent reports indicate that Pedestrians in Bangalore face a daunting task in using roads and footpaths and the pedestrian safety index is 0.63, a way below than other metros4.
The Trauma Center at National Institute of Mental Health and Neuro Sciences (NIMHANS), Bangalore, is one of the largest neurotrauma facilities in south India dealing with an average of 10,416 (mean of last 4 years- 2006 to 2009) patients per annum. There is a paucity of Indian literature on pedestrian neurotrauma. Hence, the purpose of the present study was to study the pattern of injuries sustained by pedestrians with special focus on head injuries, and to evaluate the postmortem data of pedestrian deaths.
Material & Methods
During June to September 2009, the emergency services at NIMHANS, Bangalore attended to 2555 head injury victims. Of these, 529 (20.7%) patients were pedestrians. Emergency case records and case files of these consecutive 529 patients were studied. A proforma (EPIINFO software, USA) was made to fill information about age, gender, time and place of injury, time taken to reach hospital, primary aid, associated injuries, Glasgow's coma score (GCS), CT scan requirement and findings, treatment given and the condition at discharge.
In the second part, records from hospital mortuary were retrospectively analyzed from January 1, 2007 to December 31, 2009. An analysis of 326 patients who died as pedestrians in accidents during this period was performed.
Statistical analysis: It was performed in SPSS 15 version (SPSS, Inc., Chicago, IL, USA; Network license, serial no. 5047404). Data expressed using descriptive statistics such as mean, standard deviation for continuous variables and frequency, percentage of categorical variables with risk (confidence interval 95%) and independent t test for continuous variable with significance level of P 0.05.
Results
During the period of the study, 2555 patients of head injury were treated, 529 (20.7%) of these patients were injured as pedestrians (Fig. 1). The majority of the injured pedestrians belonged to age group 18 to 50 yr (n=277, 52.4%). The elderly and paediatric group contributed 47.6 per cent (n=252) of total patient population. Majorities of patients were males (n=372, 70.3%). Majority of pedestrian injuries (221/529, 41.8%) occurred during peak traffic hours in the evening (1600-2100 h). The casualty attended to 4.17 injuries per day during weekdays and 4.8 per day on weekends. Bangalore city (urban and rural) accounted for 57.5 per cent (n=304) of all injuries.
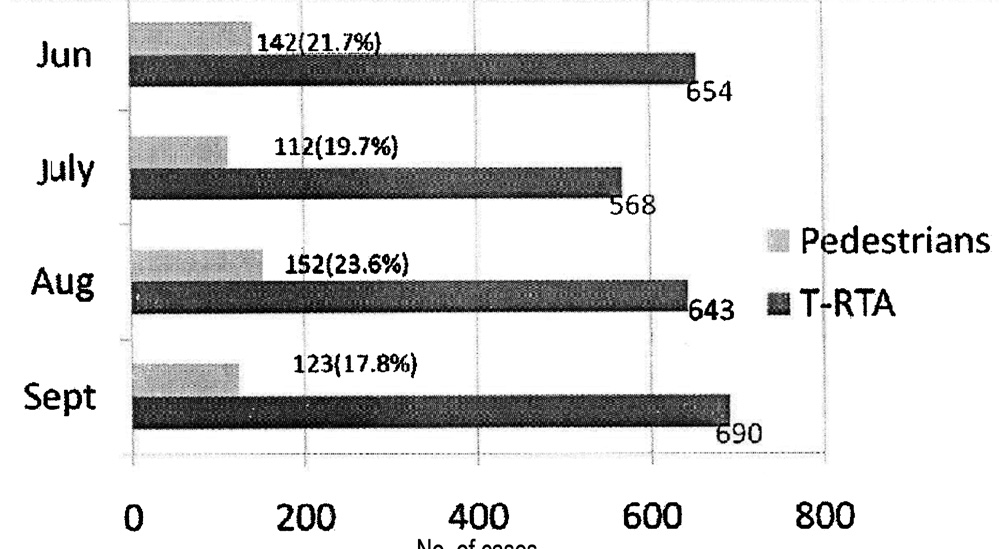
- Ratio of pedestrian to total head injuries.
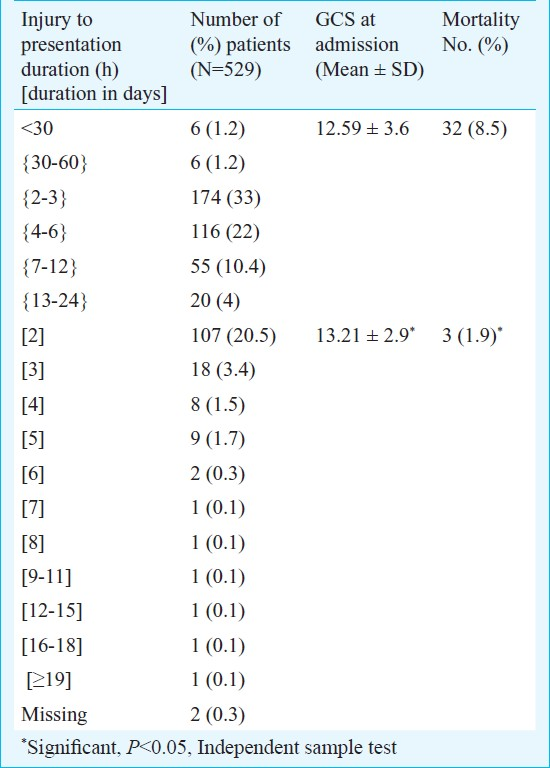
Majority of the patients (461/529, 87.1%) had received some form of primary care before attending the hospital casualty. Nearly two thirds of all patients reached the casualty services (71.6%) in less than 24 h after the injury. The mean GCS score in this group was significantly (P<0.05) less and mortality rate high as compared to patients who presented more than 24 h after injury (Table I). A two wheeler was found to be the involved vehicle in majority of pedestrian crashes (260/529, 49.1%). In 57 of 529 (10.8%) pedestrian injuries, the involved vehicle was a heavy vehicle (bus or truck); 28 (49%) of these 57, accidents occurred outside Bangalore city. Maximum members of three wheelers (auto) and pedestrian crashes occurred between 1600-2100 h (27/53, 50.9%). The offending vehicle was not known in 56 pedestrian injuries (10.5%). Interestingly 41% (23/56) of these occurred during late-night hours (2100-0700 h).
On admission, 292 patients (55.2%) sustained moderate or severe head injury (GCS - 3 to 13). Twenty five per cent (64/260, 24.6%) of all pedestrians injured with a two wheeler sustained severe head injury, whereas (34/100, 34%) of all patients injured by a four wheeler sustained severe head injury. Interestingly, 44.6 per cent (25/56) of all pedestrians injured by an unknown vehicle had suffered severe head injuries. On examination, 56 patients (10.6%) had abnormal pupils on light reaction. Associated injuries were found in 90.4 per cent (478/529) patients. The total number of associated injuries were 727; 162 (22.2%) of these injuries were major. Major thoraco-abdominal trauma was seen in 4 per cent and spine injury in 2.3 per cent of the patients.
Patients with a post-resuscitation GCS less than 15 were subjected to CT scan. Other patients were observed clinically for a period of 24 h and discharged if GCS was equal to 15 after the observation period. Of the 529 patients, 334 (63.2%) underwent CT scan and 214 had an abnormal CT scan (presence of skull fracture with or without intracerebral or extracerebral hematoma). The most common injury was cerebral contusion which was seen in 47.2 per cent of scans. Skull fractures, contusions and extra-dural hematoma were more commonly seen on the right hemisphere.
Majority of the patients could be managed conservatively. Surgery for hematoma evacuation was required in 30 of 529 (5.7%) patients. The majority of patients were discharged with GCS 14 to 15 (429, 81%). The mortality rate of pedestrian head injury was 6.6 per cent (35/529).
The mortuary attached to the hospital conducts postmortems on all patients who succumb to death after sustaining neurotrauma. During 2007 to 2009 pedestrian deaths contributed 326 out of 1243 (26.2%) postmortems conducted during this period (Fig. 2). Majority of the patients were young (18 to 50 yr - 181/326, 55.5%) and males (240/326, 73.6%). Of these 326 patients, 206 (63.2%) were injured as pedestrians within Bangalore city. Most of the fatal crashes occurred between 1600-2100 h (111/326, 34%) followed by 2300-0400 h (64/326, 19.6%). Most of the fatal pedestrian crashes occurred during week days (245/326, 75.1%, 0.31/day). The remaining 81 accidents (24.8%, 0.26/day) occurred on weekends. Two wheelers were the involved vehicle in majority of the fatal injuries (130/326, 39.9%) followed by four wheelers (91/326, 27.9%).
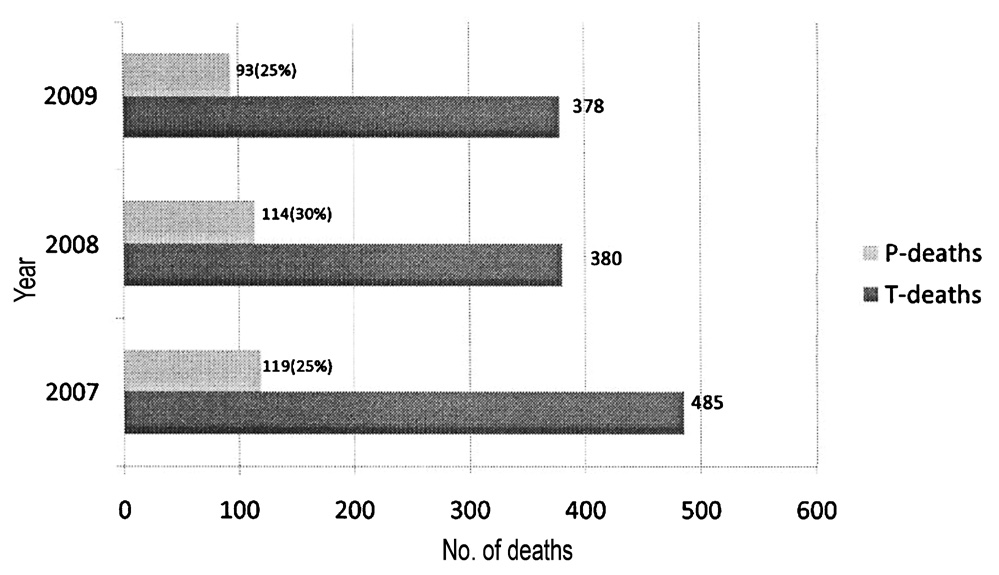
- Pedestrian (P) deaths vs total (T) deaths.
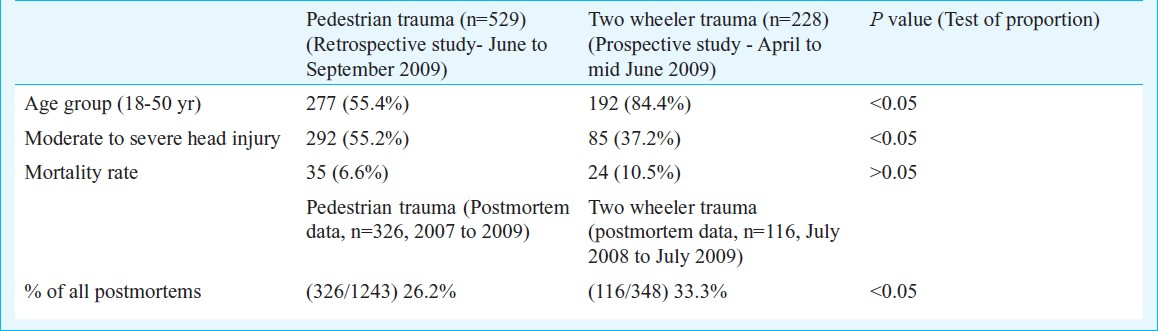
The demographic profile, injury severity, mortality rate and post-mortem details of two wheelers from same institute are compared with the pedestrian data (Table II).
The most common autopsy finding was diffuse brain oedema (96.6%). Interestingly right sided hematomas were more common as compared to the left sided ones (contusions, extra dural hematoma, brain lacerations). Associated injuries were detected in 310 patients (95%). The most common cause of death was head injury alone (277/326, 84.9%). Significant associated injury in addition to head injury was the cause of death in the remaining 49 patients (15.1%).
Discussion
To summarize the results, every fifth head injury patient attending the casualty services at NIMHANS was a pedestrian. Almost one-third of these injured pedestrians reached the hospital more than 24 h after the accident. Half of these patients belonged to the paediatric or elderly age groups. A two-wheeler was involved in almost every second pedestrian head injury. More than half of all these patients sustained moderate or severe head injury. Every second or third patient had an abnormal CT scan. Almost all of these patients sustained associated injuries. Nearly every fifteenth patient succumbed to the head injury. Pedestrian deaths constituted nearly one third of all the postmortems conducted at our center during the study period.
Pedestrian-related crashes cause an estimated 1.2 million deaths and 50 million injuries worldwide9. The African continent accounts for 55 per cent of all pedestrian fatalities across the world5. The distribution also varies across low, middle, and high-income countries; 45 per cent of road traffic fatalities in low-income countries are among pedestrians, whereas an estimated 29 per cent in middle-income and 18 per cent in high-income countries are among pedestrians6. In developing and underdeveloped countries, walking is one of the common mode of transport and pedestrian accidents have been increasing in number in these countries. Dandona et al7 conducted a study regarding non fatal road traffic injuries among children in urban India. They concluded that children of highest household incomes were significantly less likely to sustain pedestrian injury as compared to children with low household incomes. In developed countries the incidence of pedestrian injuries however, seems to be decreasing due to improvements in trauma care and a nationwide decline in walking8.
Two wheeler and pedestrian trauma are extremely common in developing countries1. Pedestrian trauma prevention however, fails to get as much attention as two wheeler trauma. Recently a study was conducted on two wheeler trauma at NIMHANS9. As evident from Table II, pedestrian trauma involves almost all age groups, whereas, two wheeler injuries mainly affect the young economically productive age group (18-50 yr). There is a significantly higher incidence of moderate to severe head injury amongst pedestrian trauma victims. Tokdemir et al5 also found that the GCS values of pedestrian victims were significantly lower than those of the motor vehicle occupants on admission.
In the present study, the most commonly involved vehicle was found to be two wheeler. Umaru et al10 in a similar study from Nigeria stated that motorcycles were responsible for most of the pedestrian injuries. Baldwin et al11 (2008) in their study from London, UK found that 74 per cent of all pedestrian injuries involved either a bus or a car.
The prognosis of an injured patient also depends on how early he/she receives specialty care. In our study, it was observed that only 2.4 per cent cases reached our Institute within one hour and 29 per cent reached after 24 h. Martin et al12 in a study from Philadelphia, Pennsylvania, found that mortality rates varied across various age groups. The mortality rate among patients above the age of 65 yr was 15.2 per cent and 3.3 per cent in patients below the age of 65 yr. The mortality rate in the present study (mainly focusing on neurotrauma) was 6.6 per cent.
Pedestrian injuries form a major part of the workload of a neurotrauma emergency. Majority of them sustained moderate to severe head injury. Even in an urban setting, almost one-third of the injured pedestrians reach the hospital more than 24 h after the injury. More attention, infrastructure and strict implementation of rules are required to reduce pedestrian injuries.
References
- Road traffic injury prevention in India. Bangalore: National Institute of Mental Health and Neuro Sciences; 2006.
- World report on road traffic injury prevention. Geneva: WHO; 2004.
- National Crime Records Bureau. In: Accidental deaths and suicides in India. New Delhi: Ministry of Home Affairs, Government of India; 2007.
- [Google Scholar]
- Study of Traffic and Transportation Policies and strategies in Urban areas in India, Final report. New Delhi: Ministry of Urban Development; 2008.
- [Google Scholar]
- Comparison of the severity of traumatic brain injuries in pedestrians and occupants of motor vehicles admitted to Firat health center: a five-year series in an Eastern Turkish city. Med Sci Monit. 2009;15:PI1-4.
- [Google Scholar]
- Distribution of road traffic deaths by road user group: a global comparison. Inj Prev. 2009;15:55-9.
- [Google Scholar]
- Road use pattern and risk factors for non-fatal road traffic injuries among children in urban India. Injury. 2011;42:97-103.
- [Google Scholar]
- Patterns of head injury among drivers and pillion riders of motorised two-wheeled vehicles in Bangalore. Indian J Neurotrauma. 2010;7:123-8.
- [Google Scholar]
- Pedestrian injuries resulting from road traffic accidents: the Azare experience. Niger J Med. 2007;16:169-72.
- [Google Scholar]
- Look right! A retrospective study of pedestrian accidents involving overseas visitors to London. Emerg Med J. 2008;25:843-6.
- [Google Scholar]
- Are roadside pedestrian injury patterns predictable in a densely populated, urban setting? J Surg Res. 2010;163:323-6.
- [Google Scholar]




