
Translate this page into:
Lumpy body & starry sky: A case of disseminated cysticercosis
*For correspondence: drsorabjee@sorabjee.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 29 yr old right-handed, vegetarian, immunocompetent male from Rajasthan was referred to the Emergency Department, Bombay Hospital Institute of Medical Sciences, Mumbai, India, in September 2014 with a six month history of headache and seizures. He denied any B symptoms. On examination, he had multiple painless subcutaneous lumps measuring 1 cm × 1 cm diameter better felt on the thighs and neck. He had impaired memory and judgement without any focal neurological deficit. There was no organomegaly or lymphadenopathy. Contrast enhanced computed tomography (CECT) brain scan revealed the classic 'starry-sky’ appearance (Fig. 1) suggestive of neurocysticercosis. Magnetic resonance imaging (MRI) brain with gadolinium contrast showed multiple cystic lesions with intracystic nodules suggestive of scolex (Figs. 2 and 3). His ELISA serology for cysticercal IgG antibody was strongly positive (>1:400). However, his stool examination for parasites was unremarkable. He was treated with antiepileptics (phenytoin 300 mg daily, levetiracetam 500 mg twice daily) and steroids (oral prednisolone 1 mg/kg). Albendazole was deferred in view of disseminated lesions with scolex suggesting ‘activity'. He responded dramatically to steroids with improvement in neurological symptoms within 48 h. After first eight weeks, steroids were gradually tapered at 5 mg every two weeks. His headache subsided completely after two weeks and he did not have recurrence of seizures. At one-year follow up, he was stable without any new lesions Fig. 4 on 5 mg prednisolone alternate day.
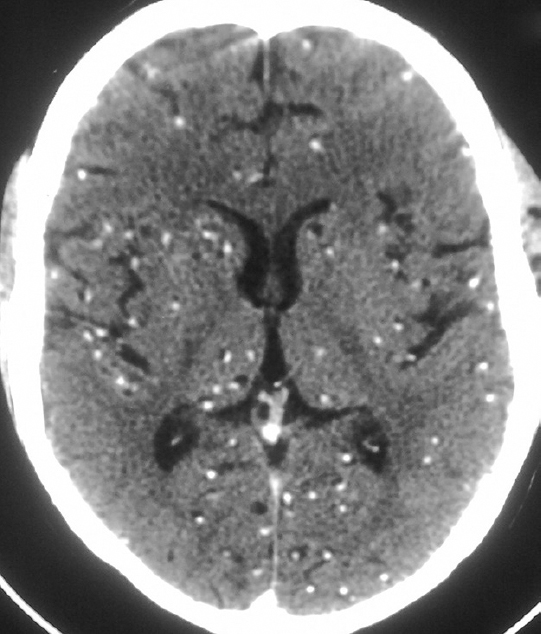
- Contrast-enhanced computed tomography (CECT) brain showing innumerable hyperdensities with eccentric calcific foci in both cerebral hemispheres - 'starry sky’ appearance.
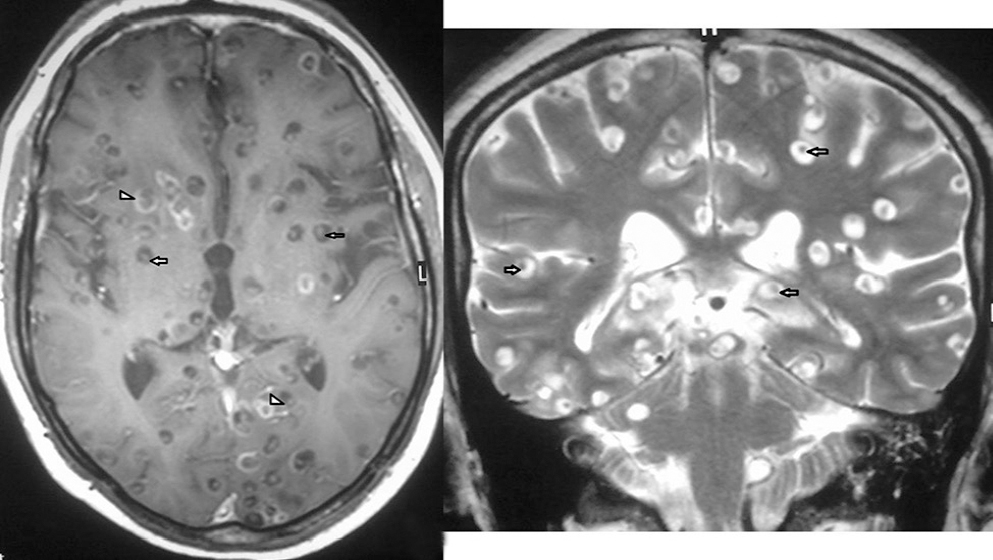
- (Left panel) Magnetic resonance imaging (MRI) brain T1-weighted sequence showing multiple hypointense cystic lesions, some with eccentric peripheral enhancement (arrowheads) and some with intracystic nodules suggestive of scolex (arrows). The head of the larva in the cyst gives the lesion a pathognomonic ‘hole-with-dot’ appearance. (Right panel) MRI brain T2-weighted sequence showing multiple hyperintense cystic lesions with intracystic hypointensity suggestive of scolex (arrows).
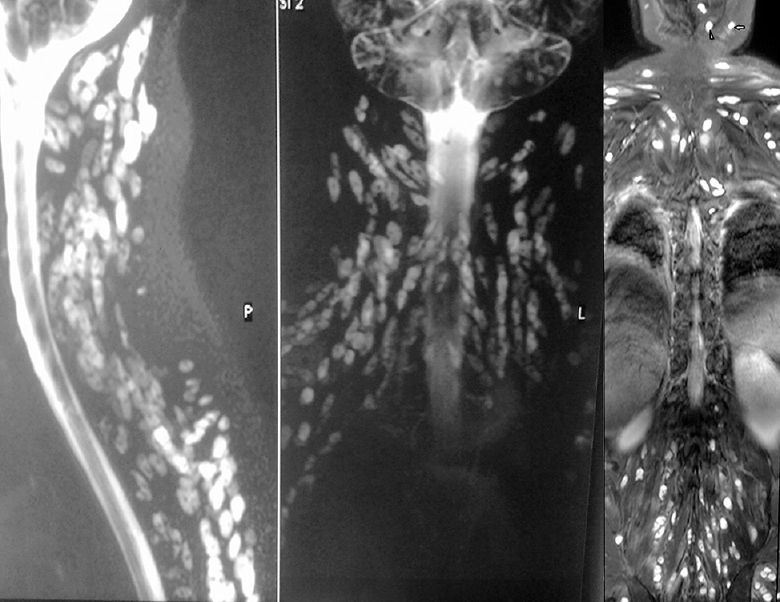
- (Left and middle panels) Magnetic resonance imaging (MRI) spine shows diffuse large ovoid cystic lesions in paraspinal region. (Right panel) MRI spine shows generalized uptake in all muscles including masticator (arrow) and tongue muscles (arrowhead).
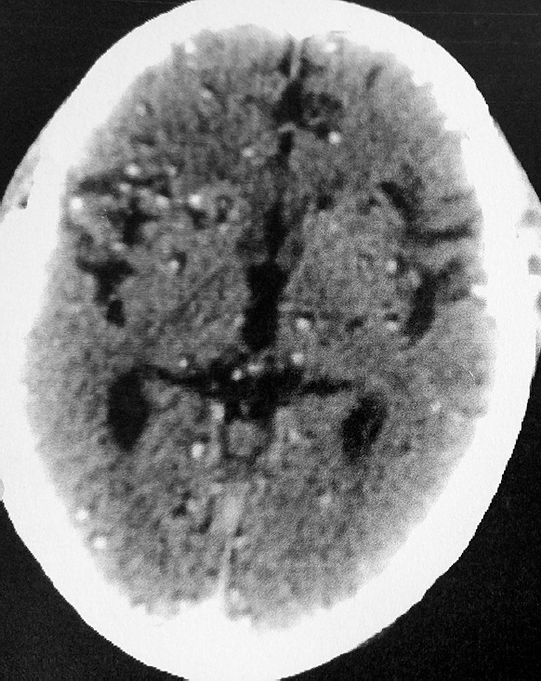
- Follow up CECT brain after one year showing a mild reduction in number of lesions.




