Translate this page into:
Long term non progressors (LTNP) with vertically infected HIV children - a report from western India
*For correspondence: 1/B Saguna, 271/B St Francis Road, Vile Parle (W) Mumbai 400 056, India irashah@pediatriconcall.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
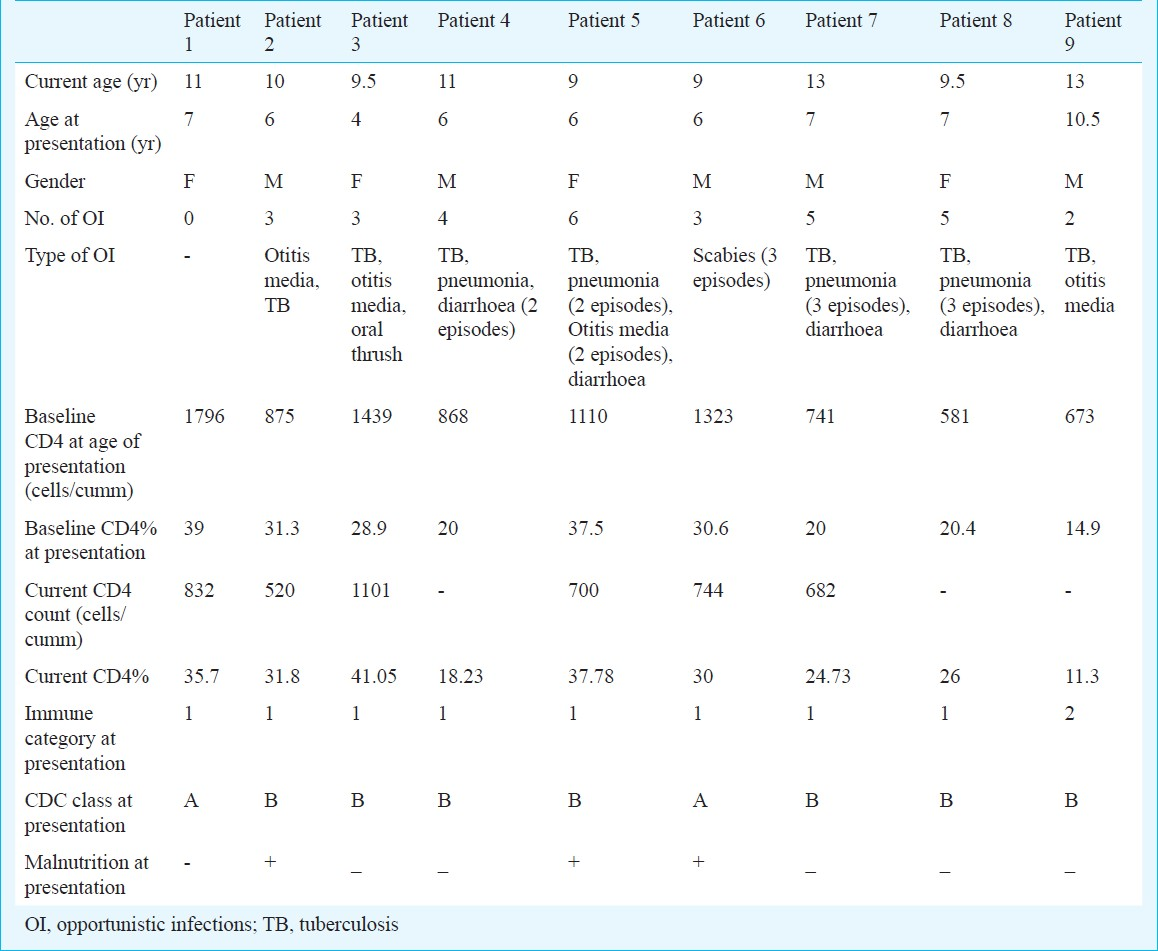
Long term non progressors (LTNPs) are individuals who are infected with HIV, but control the infection without antiretroviral therapy (ART). Vertically transmitted HIV infected children are now surviving into their adolescence due to ART. Very little is known about LTNP in vertically infected HIV positive children. We present here information on nine children with vertically transmitted HIV who have not been on ART and are controlled immunologically and clinically. They were considered to be long term non progressors if they were clinically controlled (had either no symptoms or only mild symptoms of HIV infection not requiring hospitalization), antiretroviral free, and with CD4 cell count >500 cells/mm3 and were more than 8 yr of age1. Details of each patient are given in the Table. The mean age was 10.6 ± 1.6 yr with age range of 9 to 13 yr. The average follow up duration was 3.7 yr, with a median of 4 and range of 2.5 to 4 yr. The male: female ratio was 1:1, with no difference in clinical characteristics or progression between the genders. The average number of opportunistic infections in these children was found to be 3, with a range of 0 to 6, throughout the follow up period. The types of opportunistic infections that occurred were tuberculosis in 7, pneumonia in 6, acute otitis media in 5, acute diarrhoea in 4, scabies in 3 and oral thrush in 1 individual. None of the infections required hospitalization. At presentation, two children belonged to Centers for Diseases Control (CDC) class A, and seven belonged to CDC class B. At follow up, eight children were asymptomatic whereas one child belonged to class A. At baseline, five children were underweight and four had normal weight centiles. Three of the five underweight children showed improvement in weight on follow up and one of the four normal weight children showed decrease in weight but was still within normal centile on follow up. The baseline CD4 count was 1045.1 ± 404.2 cells/μl. The baseline CD4% was 26.9 ± 8.5. The baseline CD4:CD8 ratio was 0.55 ± 0.25, with the latest CD4:CD8 ratio on follow up being 0.57 ± 0.16. At presentation, seven children belonged to immune category 1 and two to category 2 which did not differ with the CDC class. On follow up, the distribution remained the same, with none of the children worsening to category 3 on follow up.
LTNP have been described rarely in children12 across the world. This is perhaps the first report of LTNP in vertically transmitted HIV infected children from India. LNTP constitute 5-15 per cent of HIV-infected individuals3. Studies have used different definitions, making comparisons difficult, but LTNP maintain good CD4 counts and tend to have low viral loads, although are not defined on the basis of viraemia because viral load testing was not available until the mid-1990s3. As viral load testing became available, most long term non progressors were shown to have low to moderate amounts of viraemia, and further follow up revealed that many had progressively increasing viral loads and declining CD4+ T cell counts4. Elite controllers (EC) constitute <1 per cent of HIV-infected individuals who maintain undetectable viral loads (<50 copies/ml) in the absence of ART5.
Various mechanisms for non progress of HIV disease in LTNP have been proposed. It has been found that antiretroviral that was unsuccessfully used to prevent maternal-to-child transmission (ZDV use in neonatal period) was associated with better prognosis and LTNP in these children2. None of our patients had been diagnosed to be HIV infected at birth and none of them had any perinatal exposure to antiretroviral drugs. It has been established that defective nef genes in the HIV virus and differences in the Nef-mediated down-modulation of CD4 and MHC-I cell surface expression can be associated with different rates of HIV-1 disease progression. Nef alleles derived from HIV-1-infected children with non-progressive infection are significantly more active in the upregulation of MHC-1 and downregulation of MHC-II than those derived from rapid progressors5. We could not do the nef gene anaylsis and thus do not know if that had any effect on the non-progression of the disease. HLA-B5701 and to a lesser extent HLA-B27 are strongly enriched among North American and European cohorts of HIV controllers compared to non controllers6. HLA class determination was not done in our patients.
Although there are multiple factors that may play a role in modulating the degree of HIV viraemia, current data indicate that durable in vivo control of HIV cannot be entirely explained by virus or host factors studied to date. Since HIV infected children are now surviving into adolescence, an understanding of their ability to control HIV infection may lead to the development of immune therapies or a therapeutic vaccine in future.
References
- A descriptive study of HIV-infected long-term surviving children in Barbados - a preliminary report. West Indian Med J. 2005;54:167-70.
- [Google Scholar]
- Neonatal factors associated with HIV long term non-progressors in a cohort of vertically infected children in Rio de Janeiro, Brazil (‘Peixe’ Project) Braz J Infect Dis. 2009;13:276-9.
- [Google Scholar]
- The immunology of paediatric HIV. Available from: http://www.eurocoord.net/PDF/october2009-Report.pdf
- [Google Scholar]
- Naturally HIV-1 seroconverters with lowest viral load have best prognosis, but in time lose control of viraemia. AIDS. 2002;16:791-3.
- [Google Scholar]
- Nef alleles from children with non-progressive HIV-1 infection modulate MHC-II expression more efficiently than those from rapid progressors. AIDS. 2007;21:1103-7.
- [Google Scholar]
- Maintenance of viral suppression in HIV-1-infected HLA-B *57+ elite suppressors despite CTL escape mutations. J Exp Med. 2006;203:1357-69.
- [Google Scholar]




