
Translate this page into:
Initial presentation of tonsillar carcinoma with candidiasis
*For correspondence: zhengping_shi@yahoo.com.tw
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 57 yr old man† presented to the department of Otorhinolaryngology-Head and Neck Surgery, Tri-Service General Hospital, Taipei, Taiwan, in April 2014 with fever, otalgia, sore throat, odynophagia and mild swelling in the right side of infra-auricular region for three weeks. He had no systemic disease and had no history of ingestion of immunosuppressant drugs. Intraoral examination revealed a whitish pseudomembrane over right tonsil without enlargement and prominent ulceration (Fig. 1). There was no bleeding on touch. The tonsil culture was performed and Candida albicans was reported. The result from the fine-needle aspiration of neck mass demonstrated metastatic squamous cell carcinoma. Subsequently, the punch biopsy of right tonsil was performed. The histopathological result revealed tumour cells with high nuclear-cytoplasmic ratio infiltrating in the stroma and intermixed with proliferative fungus (Fig. 2). Poorly differentiated squamous cell carcinoma of the tonsil with candidiasis was confirmed. A contrast-enhanced computed tomography scan of the neck revealed no apparent enhancing lesion in the tonsillar region and an enlarged necrotic level II lymph node measured at 2.5 cm×1.6 cm in the right side of neck. No distant metastasis was found. The patient received concurrent chemoradiotherapy and no recurrence was found at three year follow up after treatment.

- Endoscopic view of oropharynx showing pseudomembrane coating over right tonsil.
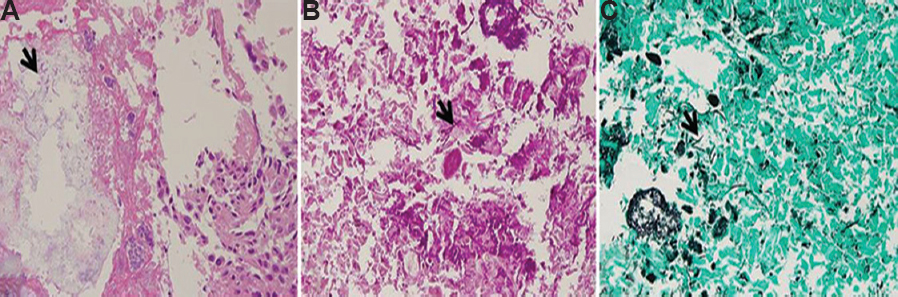
- (A) Photomicrograph of haematoxylin and eosin-stained section of punch biopsy of right tonsil showing carcinoma cells with focal necrosis and Candida pseudo-hyphae (arrow) (×200). (B) Periodic acid-Schiff-stained section highlighting fungal spores and hyphae (arrow) (×400). (C) Gomori methenamine silver-stained section showing fungal spores and hyphae (arrow) (×400).
Patients with head and neck malignancies are predisposed to suffer from oropharyngeal candidiasis because of the impairment of host defence mechanism resulting from radiation therapy and chemotherapy; however, the first manifestation as Candida infection in a tumour site is uncommon. In this case, oropharyngeal candidiasis was related to the suppression of local immunity by tonsillar carcinoma. In addition, tonsillar candidiasis without a predominant ulceration or mass in the affected tonsil may be a negative factor to early recognition of tonsillar malignancy.
Conflicts of Interest: None.




