
Translate this page into:
Genotype-phenotype relationship of CCL5 in pulmonary tuberculosis infection in Sahariya tribe: A pilot study
Reprint requests: Dr Pramod Kumar Tiwari, Department of Molecular & Human Genetics, Centre for Genomics, Jiwaji University, Gwalior 474 011, Madhya Pradesh, India e-mail: pktiwari.ju@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Sahariya, a primitive tribe of Central India, has shown significantly increased incidence of pulmonary tuberculosis (PTB). Our previous study on Sahariya showed a significant association of −403G>A single nucleotide polymorphism (SNP) of CCL5 with susceptibility to PTB. Hence, this study was aimed to analyze a genotype-phenotype relationship of this disease-associated SNP to develop a potential diagnostic marker for TB in this tribe.
Methods:
The present study was carried out on 70 plasma samples from Sahariya tribe, wherein the plasma CCL5 level was determined using a commercially available ELISA kit.
Results:
The level of CCL5 decreased significantly in patients who were on therapy/completed their therapy [inactive TB patient/inactive PTB (IPTB)], particularly with AA genotype of −403G>A (P=0.046). The level, with AA genotype, was also found to gradually decrease in sputum 3+ and 1+/2+ than in sputum-negative samples. Similarly, the CCL5 level was found to be higher in sputum-positive/active TB patients than in IPTB group and healthy controls.
Interpretation & conclusions:
Our results suggested that the CCL5 level was influenced collectively not only by the genotypes of −403G>A SNP and bacillary load but also by the treatment. Thus, CCL5 may be considered for the development of a diagnostic marker and also as an indicator of recovery.
Keywords
CCL5
resistance
Sahariya
susceptibility
tuberculosis

The Central Indian State, Madhya Pradesh, is home to a large number of tribes, Sahariya being one of them. According to the Census, 1981, Sahariya has been identified as ‘aboriginal’ and then categorized as ‘primitive tribe’1. They live in an environment, highly endemic to various infectious diseases such as tuberculosis (TB) which was evident from our surveys during 2005-2012, revealing a high incidence of TB in Sahariya, as compared to their non-tribal neighbours234. They have recently been categorized as particularly vulnerable tribal groups5.
TB which, in 2016, caused approximately 1.3 million deaths and affected an estimated 10.4 million people6, is a multi-factorial disease and its pathogenesis depends on the host genetics and gene-environment/pathogen interaction. This is strengthened by the fact that only 10 per cent of the Mycobacterium tuberculosis-infected individuals develop TB7. A successful host inflammatory response, to invading microbes, results in granuloma formation, which benefits the host8 and provides niche for M. tuberculosis persistence9. This granuloma formation depends on the recruitment of activated macrophages10 and T-cells11 to the site of infection which is mediated by chemokines. CCL5 or regulated on activation, normal T-cell expressed and secreted (RANTES) is a Th1 chemokine that promotes T-cell activation and proliferation and helps in chemotaxis of memory T-cells to the site of infection12. Several reports have shown the association of chemokines, particularly CCL5, secreted by the macrophages, with pathogenesis or susceptibility to TB, due to their important role in the regulation of T-cell activation and expression during M. tuberculosis infection13. It is likely that polymorphisms in this gene, which may cause altered regulation of CCL5, can influence the pathogenesis of the disease. Our earlier study carried out in Sahariya tribe showed a significant association of −403G>A (rs2107538) of CCL5 with TB susceptibility, alone or in combination with other polymorphisms14. Considering the possible role of CCL5 in TB pathogenesis, this study was conducted to establish a genotype-phenotype relationship for −403G>A polymorphism of CCL5 to develop a potential diagnostic marker or therapeutic target for Sahariya tribe of Central India.
Material & Methods
Sample collection: A total of 70 individuals, comprising age-matched 44 clinically diagnosed TB patients [mean age±standard deviation (SD): 37.39±6.99 yr] and 26 unrelated healthy controls (mean age±SD: 37.5 ± 6.19 yr), were selected according to different genotypes of −403G>A SNP from samples of our study, where 210 TB patients and 210 healthy controls of Sahariya tribe were genotyped14. These samples were previously recruited from Sheopur district, Madhya Pradesh, India, for the study through a field-based sampling programme. The TB patients were diagnosed and categorized into two groups; active pulmonary tuberculosis (APTB) patients and inactive pulmonary tuberculosis (IPTB) patients. The APTB group included patients who were sputum/culture positive and were not on therapy. Further, at the Revised National Tuberculosis Control Programme (RNTCP) Unit, Sheopur District Hospital, sputum samples were categorized as sputum 1+, 2+ or 3+ on the basis of an earlier described method15. However, the IPTB category of TB patients included the patients who were on therapy or who had completed their DOTs course. These IPTB patients were not relapse cases and were sputum negative at the time of sampling. The recruited 44 TB patients were equally represented in each category. The TB patients included in the study were also negative for the HIV tests. Peripheral blood (3 ml) was collected in ethylenediaminetetraacetic acid (EDTA) vials from every member of the Sahariya tribe (TB patients and healthy controls) who voluntarily participated in the study. The blood was stored at 4°C for ½ h, and then plasma was separated and stored at −20°C for further analysis. Both sputum and blood samples were collected from TB patients and controls of Sahariya tribe after obtaining their prior informed consent for participation in the study and after clearance from the Institutional Ethics Committee of Jiwaji University, Gwalior, India. The study was carried out during the period from November 2010 to March 2014 in the department of Molecular and Human Genetics, Centre for Genomics, Jiwaji University, Gwalior.
SNP typing of −403G>A SNP of CCL5: The genotypic data used in this study were generated by SNP typing of −403G>A of CCL5 using amplification-refractory mutation system (ARMS) PCR in our previous study14.
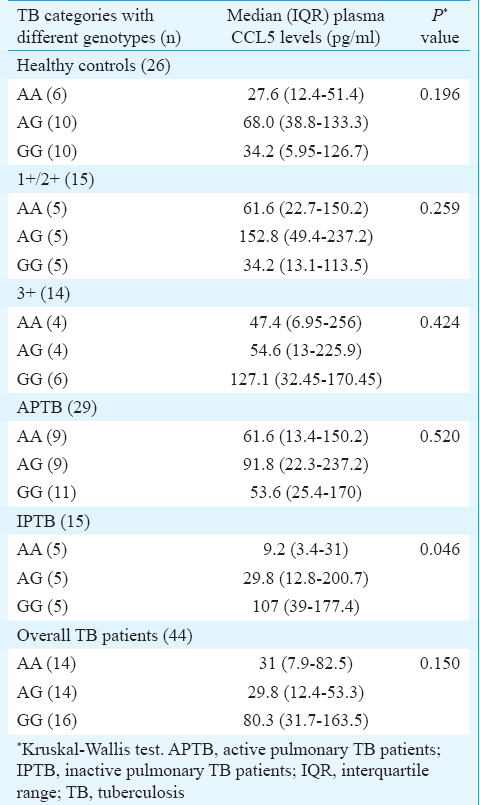
Measurement of plasma CCL5 level: The TB patients were analyzed on the basis of their (i) sputum positivity or disease status, and (ii) genotypic status for −403G>A polymorphism of CCL5. The details of the samples are given in Table I. The samples were analyzed for CCL5 using commercially available Single Analyte ELISA Kit (QIAGEN, Germany) using Sandwich ELISA method, following the manufacturer's protocol. The minimum detectable dose (MDD) of human RANTES ranged from 1.7 to 6.6 pg/ml and the mean MDD was 2.0 pg/ml. The concentration of CCL5 in different plasma samples was determined using an ELISA reader (Molecular Devices, California, USA) and the data were generated using SoftMax Pro 6.2 software (Molecular Devices, California, USA) and presented in picograms.
Statistical analysis: The data generated from ELISA were analyzed using SigmaPlot software version 11.0 (Systat Software Inc., CA, USA). The data were summarized with the median as a measure of central tendency and the quartiles as a measure of dispersion. The data were compared using Student's t test (when N was not <15) and Mann-Whitney U-test (when N was <15) to determine significant differences between the groups, while the related groups were compared using Kruskal–Wallis test.
Results
The results of genotype-phenotype relationship without stratification showed that the plasma CCL5 level did not differ significantly (P=0.196) in healthy controls with respect to all the three genotypes (Table I). However, low levels of CCL5 were found with ‘AA’ genotype, median 27.6 pg/ml [interquartile range (IQR), 12.4-51.4], while with AG genotype, it was higher, median 68.0 pg/ml (IQR, 38.8-133.3). Similar results were also found in TB patients (without stratification for disease status/bacilli load), median 31 pg/ml (IQR, 7.9-82.5), median 29.8 pg/ml (IQR, 12.4-53.3) and median 80.3 pg/ml (IQR, 31.7-163.5) for AA, AG and GG genotypes, respectively.
The results of genotype-phenotype relationship with disease status showed significantly lower levels of CCL5 in IPTB group with AA genotype, median 9.2 pg/ml (IQR, 3.4-27.6) as compared to AG, median 29.8 pg/ml (IQR, 12.8-200.7) and GG, median 107 pg/ml (IQR, 39-177.4) genotypes (P=0.046). The distribution of plasma CCL5 levels was also analyzed for each genotype within the APTB group. The results showed that plasma levels of CCL5 did not differ significantly for any of the genotypes; however, the levels were higher in sputum-positive TB patients (APTB) with AA genotype, median 61.6 pg/ml (IQR, 13.4-150.2) as compared to IPTB group, median 9.2 pg/ml (IQR, 3.4-27.6) and healthy controls, median 27.6 pg/ml (IQR, 12.4-51.4) (Table II). Further, the sub-categories of TB patients, stratified on the basis of disease status/bacilli load, were compared for plasma CCL5 levels on the basis of genotypic status to determine the genotype-phenotype relationship with bacilli load. In contrast to the results of genotype-phenotype relationship in healthy controls, high levels of plasma CCL5 were observed in samples with AA genotype in 1+/2+ sputum positive, median 61.6 pg/ml (IQR, 22.7-150.2) and 3+ sputum-positive categories of TB patients, median 47.4 pg/ml (IQR, 6.95-256), but the difference was not significant (Table I).
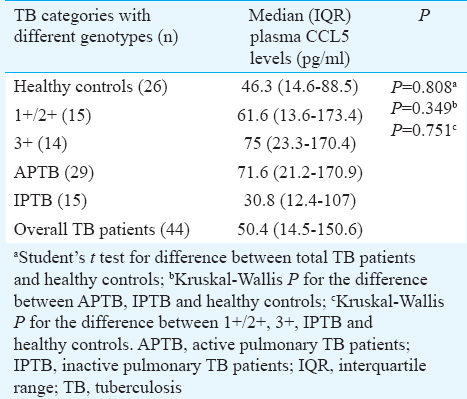
Further, the comparison of plasma CCL5 levels between TB patients and healthy controls, without stratification of genotypes, showed increased levels of CCL5 in TB patients, median 50.4 pg/ml (IQR, 14.5-150.6) as compared to healthy controls, median 46.3 pg/ml (IQR, 14.6-88.5) (Table II). No significant differences were found when plasma CCL5 levels were compared in stratified TB patients for disease status and healthy controls although the levels were higher in APTB group, median 71.6 pg/ml (IQR, 21.2-170.9), including both 1+/2+ and 3+ sputum-positive TB patients individually, median (IQR); 61.6 pg/ml (13.6-173.4) and 75 pg/ml (23.3-170.4), respectively, than in IPTB group, median 30.8 pg/ml (IQR, 12.4-107) and healthy controls, median 46.3 pg/ml (IQR, 14.6-88.5).
Discussion
CCL5 plays an important role during M. tuberculosis infection by regulating and activating the recruitment of macrophages and further activation of T-cells16. Several studies have shown the association of various polymorphisms of CCL5 with TB, maybe because these genetic variations, particularly, the promoter polymorphisms, are responsible for altered expression/levels of the protein1417181920. Among various polymorphisms of CCL5, −403G>A has been found to be significantly associated with TB susceptibility in Sahariya tribe14, alone or in combination with other polymorphism. We investigated the genotype-phenotype relationship of CCL5 in TB patients after stratification with disease status/bacilli load and in healthy controls of Sahariya tribe of India. There are few reports on Sahariya tribe showing an association of genetic polymorphisms of vitamin D receptor21, chemokines14 and HLA genes22 with pulmonary tuberculosis (PTB), but not on genotype-phenotype relationship of CCL5 in PTB.
The plasma CCL5 level was higher in APTB group, including both sputum 1+/2+ and 3+ TB patients with AA, AG and GG genotype as compared to healthy controls. However, the data were not statistically significant. A significant difference in plasma CCL5 level was found with the genotypes in IPTB patients who were on therapy or had completed their therapy. In such patients, the expression level was significantly lower with AA genotype. These results indicated that expression of CCL5 was also influenced by the pathogen as it remained high during the infection and supported our previous findings that AA genotype was a risk factor for disease development14. It also suggested that the plasma CCL5 level was affected significantly with AA genotype during treatment. However, no correction for multiple testing was applied. These results were further supported by the study of Almeida et al23, where the plasma level of CCL5 was reported to significantly decrease in treated patients for anti-mycobacterial therapy, as compared to active TB patients and healthy controls. However, the high levels of plasma CCL5 in active TB patients in the present study further implied that higher CCL5 level could result in high bacillary load as high levels of CCL5 can saturate the receptors and desensitize the cells to the migration signals24. Vesosky et al25 showed that the CCL5-knockout mice localized fewer antigen presenting cells (APCs) and chemokine receptor-positive T-cells to the lungs and showed altered cell trafficking to M. tuberculosis granulomas. These results seem to be in corroboration with a previous report, showing an association of two haplotypes of −403G>A with TB susceptibility, which acts opposite to each other by up- and down-regulating CCL5 transcription17. Similarly, other reports have shown that CCL5 can potently suppress the HIV infection at low concentrations, but with high concentration, it can actually enhance the HIV infection2627. In contrast, in coronary artery disease (CAD) patients, AA genotype was found to be related with low levels of CCL5 and GG genotype was found to be related with high levels of CCL5, while the level was balanced with AG genotypes. On the other hand, −28C/G SNP had no association with CAD risk and had no genotype-related phenotype differences18. However, −403A was reported to have no accelerating effect in HIV28. In contrast, an in vitro study reported increased transcriptional activity of CCL5, with −403A allele as compared to −403G allele19. Previous studies also suggested that −28C was associated with increased expression20 and −403A was associated with reduced expression of CCL518, which further implied that the production of CCL5 below and above this optimal range of concentrations might be associated with impaired function of this chemokine1729. This impaired function of CCL5 may affect the granuloma formation which is the pre-requisite for M. tuberculosis removal through impaired recruitment of immune cells. Thus, these studies suggest that gene polymorphisms have a definite involvement in TB pathogenesis through its effect on either up- or down-regulated expression of the gene.
The results of the present study showed that although CCL5 plasma levels neither differed significantly in healthy controls nor in TB patients with respect to all the three genotypes, the level was decreased with AA genotypes as compared to AG and GG genotypes in both the groups. It indicates that although the level of CCL5 may not be influenced by variants of −403G>A in controls and TB patients, the expression level with this variant genotype responds differently to the bacillary load and therapy. However, there is a lack of definite understanding as to how the level of CCL5 is regulated with different genotypes and bacillary load. This could be due to either limited sample size or lack of analysis on correlation with other polymorphisms. For e.g., −28C/G have been found to be associated with increased level of CCL528. These lacunae limit the generalization of our findings. Hence, further, studies with a large sample size and with more efficient technologies are needed to establish CCL5 as a diagnostic and therapeutic marker for TB, particularly, in this highly endemic Sahariya tribe.
Acknowledgment
This work was supported by the facilities available at Centre for Genomics through various funding agencies including Indian Council of Medical Research, Department of Biotechnology, Department of Science and Technology, Government of India, New Delhi. Authors thank the study participants of Sahariya tribe, the Chief Medical Officer and members of the RNTCP Unit at the District Hospital, Sheopur, for their active cooperation and support in this work. The first two authors (GM & SSP) acknowledge the Indian Council of Medical Research and Department of Atomic Energy, respectively, for providing Senior Research Fellowship.
Conflicts of Interest: None.
References
- Age at menarche and menopause among Saharia women - A primitive tribe of Madhya Pradesh. Anthropologist. 2004;6:247-52.
- [Google Scholar]
- Elevated level of serum LDH2 and LDH3 in sputum three positive TB patients of Sahariya tribe: A preliminary study. Clin Biochem. 2007;40:1414-9.
- [Google Scholar]
- Increased prevalence of pulmonary tuberculosis in male adults of Sahariya tribe of India: A revised survey. Indian J Community Med. 2010;35:267-71.
- [Google Scholar]
- Prevalence of smear-positive pulmonary tuberculosis in different ethnic groups in India: Evaluation of public health. Public Health. 2012;126:295-9.
- [Google Scholar]
- Pulmonary tuberculosis – A health problem amongst Saharia tribe in Madhya Pradesh. Indian J Med Res. 2015;141:630-5.
- [Google Scholar]
- Global tuberculosis report 2017. Geneva: WHO; 2017.
- Restraining mycobacteria: Role of granulomas in mycobacterial infections. Immunol Cell Biol. 2000;78:334-41.
- [Google Scholar]
- Lazy, dynamic or minimally recrudescent? On the elusive nature and location of the mycobacterium responsible for latent tuberculosis. Infection. 2009;37:87-95.
- [Google Scholar]
- Beta-chemokines that inhibit HIV-1 infection of human macrophages stimulate uptake and promote destruction of Trypanosoma cruzi by human macrophages. Cell Mol Biol (Noisy-le-grand). 1997;43:1067-76.
- [Google Scholar]
- T helper 1 and T helper 2 cells respond differentially to chemokines. J Immunol. 1998;160:550-4.
- [Google Scholar]
- Differential expression of chemokine receptors and chemotactic responsiveness of type 1 T helper cells (Th1s) and Th2s. J Exp Med. 1998;187:129-34.
- [Google Scholar]
- Genetic polymorphisms of CCL2, CCL5, CCR2 and CCR5 genes in Sahariya tribe of North Central India: An association study with pulmonary tuberculosis. Infect Genet Evol. 2012;12:1120-7.
- [Google Scholar]
- Sputum grading as predictor of treatment outcome in pulmonary tuberculosis. Indian J Tuberc. 2002;49:139.
- [Google Scholar]
- Polymorphisms in the RANTES gene increase susceptibility to active tuberculosis in Tunisia. DNA Cell Biol. 2011;30:789-800.
- [Google Scholar]
- Association between RANTES functional polymorphisms and tuberculosis in Hong Kong Chinese. Genes Immun. 2007;8:475-9.
- [Google Scholar]
- The RANTES -403G>A promoter polymorphism in Korean men: Association with serum RANTES concentration and coronary artery disease. Clin Sci (Lond). 2007;113:349-56.
- [Google Scholar]
- Effect of variation in RANTES promoter on serum RANTES levels and risk of recurrent wheezing after RSV bronchiolitis in children from Han, Southern China. Eur J Pediatr. 2009;168:963-7.
- [Google Scholar]
- Polymorphism in RANTES chemokine promoter affects HIV-1 disease progression. Proc Natl Acad Sci U S A. 1999;96:4581-5.
- [Google Scholar]
- Coding and non-coding polymorphisms in VDR gene and susceptibility to pulmonary tuberculosis in tribes, castes and Muslims of Central India. Infect Genet Evol. 2011;11:1456-61.
- [Google Scholar]
- Distribution of HLA-A, B and DRB1 alleles in Sahariya tribe of North Central India: An association with pulmonary tuberculosis. Infect Genet Evol. 2014;22:175-82.
- [Google Scholar]
- Anti-mycobacterial treatment reduces high plasma levels of CXC-chemokines detected in active tuberculosis by cytometric bead array. Mem Inst Oswaldo Cruz. 2009;104:1039-41.
- [Google Scholar]
- CCL5 participates in early protection against Mycobacterium tuberculosis. J Leukoc Biol. 2010;87:1153-65.
- [Google Scholar]
- Enhancement of human immunodeficiency virus type 1 infection by the CC-chemokine RANTES is independent of the mechanism of virus-cell fusion. J Virol. 1999;73:684-94.
- [Google Scholar]
- The CC-chemokine RANTES increases the attachment of human immunodeficiency virus type 1 to target cells via glycosaminoglycans and also activates a signal transduction pathway that enhances viral infectivity. J Virol. 1999;73:6370-9.
- [Google Scholar]
- Modulating influence on HIV/AIDS by interacting RANTES gene variants. Proc Natl Acad Sci U S A. 2002;99:10002-7.
- [Google Scholar]
- CCL5 (RANTES) gene polymorphisms in pulmonary tuberculosis patients of South India. Int J Immunogenet. 2011;38:397-402.
- [Google Scholar]




