
Translate this page into:
F wave index: A diagnostic tool for peripheral neuropathy
Reprint requests: Dr G. R. Sathya, Flat No. 2E, 2nd Floor, Brindhavananam Apartments, Tenth Cross, Brindhavan, Puducherry 605 013, India e-mail: ksathyavenkat@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Each skeletal muscle is usually supplied by two or more nerve roots and if one nerve root is affected and the other is spared, the clinically used F wave minimum latency can still be normal. An F wave index was constructed taking into consideration the other parameters of the F wave such as persistence, chronodispersion, latency, arm-length to determine its usefulness in the diagnosis of peripheral neuropathy. This study was undertaken to construct the F wave index in the upper limb for the median nerve in normal healthy adult males and in patients with peripheral neuropathy and to compare the values obtained in both groups.
Methods:
This hospital-based study was carried out on 40 males who were diagnosed to have peripheral neuropathy and on 40 age matched healthy males who served as the control group. The F wave recording was done using a digitalized nerve conduction/electromyography/EP machine in a quiet and dimly lit room. All recordings were done between 0900 and 1100 h at an ambient temperature of 22°C. The F wave recording was obtained from a fully relaxed muscle by stimulating the median nerve.
Results:
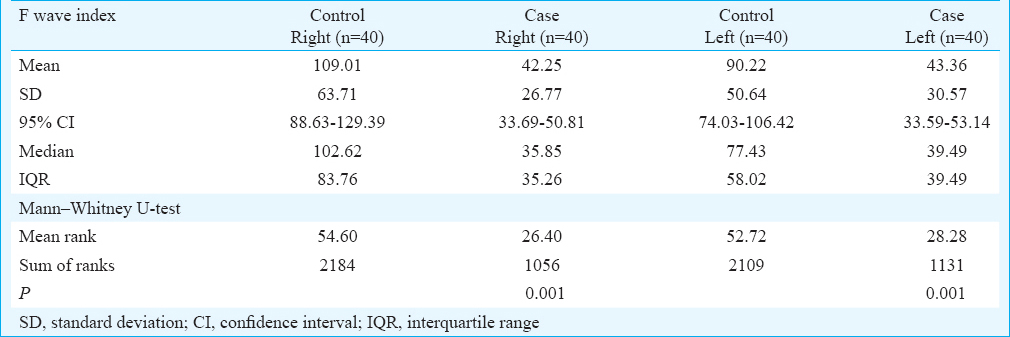
The median value for F wave index obtained from median nerve (abductor pollicis brevis) in patients with peripheral neuropathy [right arm - 35.85, interquartile range (IQR) - 35.26; left arm - 39.49, IQR - 39.49] was significantly lower (P=0.001) as compared to the control group (right arm - 102.62, IQR - 83.76; left arm - 77.43, IQR - 58.02).
Interpretation & conclusions:
Our results showed that F wave index in upper limb was significantly lower in patients with peripheral neuropathy than the healthy controls, and could be used for early detection of peripheral neuropathy.
Keywords
F wave index
latency
males
median nerve
peripheral neuropathy
upper limb

It is well known that diabetes mellitus is one of the most common diseases which affect the peripheral nerves and 47-91 per cent of diabetes patients could develop diabetic peripheral neuropathy (DPN) during their illness. If DPN is not detected and treated early, it can lead to pain, foot ulceration, infection, loss of ambulation and even amputation123. Nerve conduction studies (NCSs) are commonly used in the diagnosis of paraesthesias (numbness, tingling and burning) and weakness in the upper and lower limbs, and of these the F wave study is one of the most frequently used simple and non-invasive techniques for detecting peripheral neuropathy.
F wave is a late response that follows the motor response (M) and is elicited by supramaximal electrical stimulation of a mixed or a motor nerve4. F waves provide a means of examining transmission between stimulation sites in the arm and the leg and the related motor neurons in the cervical and lumbosacral cord. Dengler et al5 have suggested that motor units of all sizes would give rise to an F wave response, but the chance of development of F wave is greater when the twitch tension is stronger. The afferent and efferent pathway for the F wave is the alpha motor neuron.
The study of the F waves is particularly useful for the diagnosis of proximal nerve lesions that would be otherwise inaccessible to other routine NCSs6. Various F wave parameters are used for diagnostic evaluation of peripheral nerve disorder7. It serves as a sensitive measure for axonal polyneuropathy and radiculopathy and is used in the diagnosis of DPN, Guillain–Barre syndrome (GBS) and amyotropic lateral sclerosis. F waves also help in early detection of abnormality in motor fibres8. The minimal F wave latency of the median nerve in the upper limb is 34.4 msec in males and 31 msec in females. Right to left asymmetry exceeding 2 msec is considered abnormal9. Chronodispersion is the difference between the maximal and minimal latencies. It is highly sensitive for diagnosing demyelinating neuropathy9. Persistence (calculated by dividing the number of F responses by the number of stimuli) shows variation depending on the muscle i.e., highest for flexors of arm and extensors of legs9.
The F wave minimal latency is the parameter that is normally used to arrive at a clinical diagnosis. Each skeletal muscle is usually supplied by two or more nerve roots. If one root is affected and the other is spared, the F wave minimum latency might still be normal. Hence, F wave minimum latency alone may not be a sensitive parameter for the early detection of peripheral neuropathy. Discrepancies in results among various studies suggest that a diagnosis of peripheral neuropathy cannot be made by just considering a single parameter. Several studies suggested that the other parameters of F wave were prolonged in cases of peripheral neuropathy101112131415. Hence, this study was undertaken with the hypothesis that the construction of an F wave index by taking into consideration all the F wave parameters would be more accurate in diagnosing cases with peripheral neuropathy and thereby minimizing the chances of missing the diagnosis.
Thus, this study was carried out to compare the diagnosing ability of F wave minimum latency versus F wave index [Persistence × Arm length) / (Latency × Chronodispersion] in peripheral neuropathy patients.
Material & Methods
The study was carried out over a period of one year from January 2012 to January 2013 in the Department of Physiology at Pondicherry Institute of Medical Sciences (PIMS), Puducherry, India. This was a hospital-based study carried out in males aged 30 and 50 yr. The sample size was calculated based on an earlier study15 (α - 5%, β - 10%, power - 90%, standard deviation - 2.79 and precision - 2 msec). The sample size was calculated to be 34 in each group. Therefore, 40 patients with peripheral neuropathy (cases) and 40 healthy age-matched controls were included. The patients were chosen from the departments of Neurology and General Medicine (both in and outpatients) at PIMS on every alternate day. A detailed clinical history was taken using a structured questionnaire by the neurologist. The confirmed cases of peripheral neuropathy were selected based on the Toronto Clinical Score16 which included the presence of clinical features such as unpleasant, unusual or abnormal sensation such as burning pain, electric shock-like sensations, tingling, pins and needles formication, prickly feeling and cramp like sensation in the upper limb. Age-matched (±2 yr) healthy controls were chosen from among the relatives of the patients attending the outpatient department. Male patients between 30 and 50 yr of age and were confirmed to have peripheral neuropathy were included as cases. Those who had any history of carpal tunnel syndrome, GBS, myopathy, hypothyroidism, neuromuscular injury/disorders, fracture of upper limb bones and individuals with pacemakers were excluded from the study. To improve the accuracy of measurement, the variables that could have altered the F wave study such as age, gender, temperature and arm length were taken care of by matching the age, enrolling only males in the study, maintaining a standard temperature and by correcting latency for arm length in the F wave index. The temperature in the electrophysiology laboratory was maintained at 22°C. The study was carried out at a fixed time of the day (between 0900 and 1100 h). A standardized routine clinical procedure was used for recording the F response1718. The F wave was recorded from the abductor pollicis brevis (APB) by stimulating the median nerve. The F wave parameters were recorded directly using a digitalized nerve conduction/electromyography (EMG)/EP machine (Aleron, Recorders Medicare Systems, Chandigarh, India).
This study was conducted after obtaining ethical clearance from the Institute's Ethical Committee and after getting a written informed consent from all the participants.
Statistical analysis: The data were analyzed using Statistical Package of Social Sciences, version 16.0, (SPSS Inc, Chicago, USA). Mean, standard deviation, median, confidence interval and interquartile range (IQR) of F wave latency and F wave index were tabulated. Unpaired t test and Mann–Whitney U test were used to compare the mean score of F wave minimum latency and mean score of F wave index, respectively among healthy individuals and patients with peripheral neuropathy.
Results
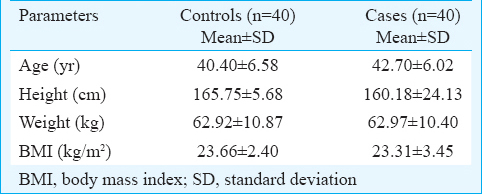
The demographic parameters of the controls and peripheral neuropathy patients are presented in Table I. There was no significant difference between the two groups. The F wave minimum latency was significantly shorter in controls (right arm - 27 msec; left arm - 26.48 msec) as compared to those with peripheral neuropathy (right arm - 28.28 msec; left arm - 29.08 msec) (Table II). Since the data of F wave index were skewed, the median score of F wave index was analyzed using Mann–Whitney U test. The F wave index was significantly less in peripheral neuropathy patients (right arm - 35.85; left arm - 39.49) as compared to controls (right arm - 102.62; left arm - 77.43) (Table III). The Figure shows that F wave index detected more number of cases with peripheral neuropathy (right arm - 85%; left arm - 80%) than F wave minimum latency (right arm - 7.5%; left arm - 32.5%).

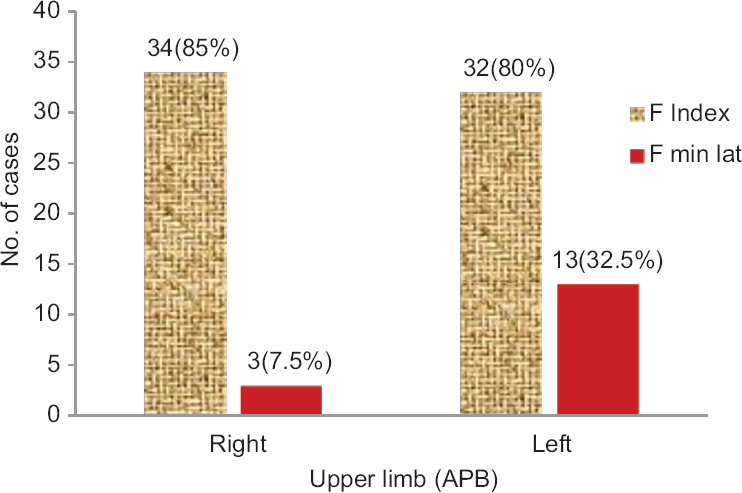
- Bar diagram showing case detection by F wave index and F minimum latency in the upper limb (abductor pollicis brevis, APB) of patients with peripheral neuropathy.
Discussion
Besides history taking and clinical examination, NCS plays an important role in the diagnosis of neuropathy because electrophysiological signs of neuropathy are well detected despite clinical symptoms1920. Efforts have been made towards establishing the mechanism that underlies the complication as well as the methods that could prevent, diagnose and treat it2122. Among all the NCS, F waves are the most sensitive and reliable NCS for evaluating polyneuropathies and can provide a meaningful physiological window into disorders of the central nervous system23. Our study was aimed at determining the effectiveness of F wave minimum latency versus F wave index in detecting peripheral neuropathy.
Our study showed that comparison of F wave minimum latency between controls and peripheral neuropathy patients in both the arms was significant as also shown in other studies242526. Individuals who had their F wave minimum latency more than 30.84 msec in the right arm and 32.24 msec in the left arm were considered as confirmed cases of peripheral neuropathy. This cut-off was derived by considering the upper limit of F wave minimum latency among healthy volunteers. Those individuals who had their F wave index less than 35.85 in the right arm and 39.49 in the left arm were considered as confirmed cases of peripheral neuropathy. This cut-off was arrived at by considering the lower limit of F wave index among patients with neuropathy.
There were some studies which showed that the other parameters like F wave maximum latency, chronodispersion or tachydispersion would be more sensitive than F wave minimum latency in detecting neuropathy101112131415. The present study included all the parameters of F wave in constructing the F wave index to determine its usefulness in the diagnosis of peripheral neuropathy. Since the F wave index showed a skewed data, median and IQR were considered. The results of the present study showed that F wave index was significantly lower in patients with peripheral neuropathy than that of controls.
Our study showed that the F wave index was able to detect more number of patients with peripheral neuropathy as compared to F wave minimum latency and could be used as a better tool in detecting peripheral neuropathy in the upper limb (median nerve - APB) rather than the F wave minimum latency alone. It has been suggested that the accuracy of persistence in the F wave testing would be better if the number of stimuli given to the nerve is ≥20427. However, in the present study, the digitalized nerve conduction/EMG/EP machine used was able to stimulate the nerve only 15 times, and this might have been responsible for obtaining a decreased persistence. This could have been the reason why the F wave index was able to detect only 85 per cent of the patients with neuropathy in the right arm and 80 per cent patients with neuropathy in the left arm.
There were certain limitations in the present study. The normal values for F minimum latency and F Index were derived from the normal individuals and patients with peripheral neuropathy. The skewed data in our study could be due to small sample size. Further, in our study, F wave index was calculated only for the median nerve - APB muscle in the upper limb. Hence, studies should be carried out to calculate F wave index using a larger sample size, in both genders and in all the nerves of the upper limb. Since the cases and controls were chosen from the hospital, the results cannot be extrapolated to the entire population. Other neurological tests such as quantitative sensory testing (QST) and sympathetic skin response (SSR) were not carried out to detect peripheral neuropathy.
In conclusion, early detection of peripheral neuropathy by electrophysiological study like F wave index would help to diagnose and provide better treatment options for patients with peripheral neuropathy.
Acknowledgment
The authors thank all the faculties, study individuals, technical and non-teaching staff for their support.
Conflicts of Interest: None.
References
- The peripheral neuropathy evaluation in an office-based neurology setting. Semin Neurol. 2011;31:102-14.
- [Google Scholar]
- Current medical management of diabetic foot infections. Expert Rev Anti Infect Ther. 2010;8:1293-305.
- [Google Scholar]
- F wave. In: Aminoff HJ, Brown WF, Bolton CF, eds. Neuromuscular function and disease Vol 1. (1st ed). Philadelphia: Saunders; 2002. p. :473-81.
- [Google Scholar]
- Nerve conduction studies: Essentials and pitfalls in practice. J Neurol Neurosurg Psychiatry. 2005;76(Suppl 2):ii23-31.
- [Google Scholar]
- The diagnostic sensitivity of different F wave parameters. J Neurol Neurosurg Psychiatry. 1998;65:535-40.
- [Google Scholar]
- The relative diagnostic sensitivity of different F-wave parameters in various polyneuropathies. Muscle Nerve. 1992;15:912-8.
- [Google Scholar]
- F response latencies and durations in upper motor neuron syndromes. Electromyogr Clin Neurophysiol. 1986;26:327-32.
- [Google Scholar]
- A comparison of F waves in peripheral nerve disorders. Electromyogr Clin Neurophysiol. 2005;45:417-23.
- [Google Scholar]
- Assessments of chronodispersion and tacheodispersion of F waves in patients with spinal cord injury. Am J Phys Med Rehabil. 2003;82:498-503.
- [Google Scholar]
- F-waves in clinical neurophysiology: A review, methodological issues and overall value in peripheral neuropathies. Electroencephalogr Clin Neurophysiol. 1996;101:365-74.
- [Google Scholar]
- F-persistence studies in L5-S1 lumbosacral radiculopathies. Electromyogr Clin Neurophysiol. 1996;36:387-93.
- [Google Scholar]
- The value of nerve conduction study and F-wave latency in subclinical neuropathic type II diabetic patients. Med J Babylon. 2012;9:918-24.
- [Google Scholar]
- Complications, Reliability and validity of the modified Toronto Clinical Neuropathy Score in diabetic sensorimotor polyneuropathy. Diabetic Medicine. 2009;26:240-6.
- [Google Scholar]
- AAEE minimonograph #26: The electrodiagnosis of carpal tunnel syndrome. Muscle Nerve. 1987;10:99-113.
- [Google Scholar]
- Evaluative procedures to detect, characterize, and assess the severity of diabetic neuropathy. Diabet Med. 1991;8:S48-51.
- [Google Scholar]
- Electrodiagnostic studies in the management and prognosis of neuromuscular disorders. Muscle Nerve. 2004;29:165-90.
- [Google Scholar]
- Elevated glycosylated hemoglobin is associated with subclinical neuropathy in neurologically asymptomatic diabetic patients: A prospective study. J Clin Neurophysiol. 2009;26:50-3.
- [Google Scholar]
- ABC of diabetes Vol 1. (5th ed). London: BMJ Publishing Group; 2003. p. :42.
- Nerve blood flow and oxygen delivery in normal, diabetic, and ischemic neuropathy. Int Rev Neurobiol. 1989;31:355-438.
- [Google Scholar]
- F-wave conduction velocity in Guillain-Barrésyndrome. Assessment of nerve segment between axilla and spinal cord. Arch Neurol. 1975;32:524-9.
- [Google Scholar]
- Late responses as aids to diagnosis in peripheral neuropathy. J Neurol Neurosurg Psychiatry. 1980;43:156-62.
- [Google Scholar]
- F-wave latency, the most sensitive nerve conduction parameter in patients with diabetes mellitus. Muscle Nerve. 1997;20:1296-302.
- [Google Scholar]
- F wave parameters of normal ulnar and median nerves. Indian J Med Res. 2010;21:47-50.
- [Google Scholar]




