Translate this page into:
emm type distribution pattern of group A streptococcus in north India: need for a new preventive approach
+For correspondence: superoxide@sify.com
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Group A streptococcus (GAS; Streptococcus pyogenes), pharyngitis in children assumes special significance due to the development of rheumatic fever (RF)/rheumatic heart disease (RHD). Streptococcal infections with an estimated death rate of over 500,000 individuals/year place GAS among major human pathogens, exceeded by HIV, Mycobacterium tuberculosis, Plasmodium falciparum and S. pneumoniae, and probably comparable to rotavirus, measles, Haemophilus influenzae type b, and hepatitis B12. Accurate characterization of GAS is required for better control of streptococcal diseases. GAS was classified on the basis of serotypic diversity of the M protein, a major virulence factor. The emm gene (encoding M protein) sequencing based on 5’ region3is becoming a universal method of choice. Though more than 180 emm sequence types and 800 emm subtypes have been described, new types/subtypes are still emerging from different regions4. GAS affects Indian population every year causing high cardiovascular mortality, morbidity leading to considerable socio-economic losses5.
Penicillin remains the only effective treatment against streptococcal diseases and no effective vaccine is available. Vaccine based on multiple amino terminal epitopes of GAS M protein that stimulates protective immunity against homologous strains6, do not provide broad coverage protection. Even the conserved regions of M type are being deciphered these days for the development of vaccines. Active epidemiological surveillance of GAS isolates in a north Indian region representing a particular ethnic population has been instituted to generate precise information on the transmission dynamics and emm type distribution for considering vaccine strategy in Indian scenario.
Carapetis et al1 estimated the occurrence of over 616 million incident cases of GAS pharyngitis worldwide per year. GAS pharyngitis and carriage in asymptomatic children varies in different countries. In India, prevalence of GAS pharyngitis and carriage ranges from 4.2 to 13.7 per cent and 1.3 to 20 per cent respectively57–9. GAS impetigo is quite common in south as compared to north India where pharyngitis is more common9. A few studies have reported the emm types from various geographical locations of India for a particular time span79–12. The emm types of these are heterogeneous in nature. Also the relationship of emm type with their isolation site needs to be discussed as has been done in the western world13. The types prevalent in India are different from those reported elsewhere1415, suggesting that the same serotypes are present within a population, but vary between distinct geographical settings. In the absence of exact GAS type distribution data, true propensity of any preventive strategy against streptococcal infection remains incomplete. Moreover, for the eventual introduction and success of multivalent vaccines or vaccines based on conserved regions, better understanding of GAS infections and their molecular epidemiology in India becomes imperative.
We compiled the epidemiological surveillance data of GAS emm types carried out in some north Indian communities, i.e., Panchkula district of Haryana; Roopnagar of Punjab and Chandigarh during 1995 to 2007. The volunteers (school going children age 5-15 yr) from urban, rural and peri-urban slums were included in the study. A total of 17,071 samples were collected from north India during the study period. Throat swabs (n=14008) from peri-tonsillar and posterior wall of pharynx of pharyngitis patients or asymptomatic carriers, RF/RHD patients (n=11) and skin swabs (n=3063) from skin infected patients were taken. Betahaemolytic streptococcal colonies were isolated using standard protocol16, confirmed as Lancefield GAS by latex agglutination kit (Streptex, Murex Biotech Ltd, UK) and preserved in 20 per cent glycerol stocks in -70°C. Of these 17071 samples, 446 were confirmed to be GAS (276 from throat of pharyngitis /asymptomatic cases, 11 from RF/RHD and 159 from skin infected patients) with the prevalence rate of 2.6 per cent.
GAS isolates (240 from throat of pharyngitis/asymptomatic cases, 156 from skin infected patients and 11 from RF/RHD cases) were reconfirmed and emm typed by protocol as published earlier7; 373 isolates showed ≥95 per cent homology with the reference emm types, 16 isolates were identical to sequence types and 18 (4.4%) were M non typeable (MNT). The emm types were further designated as emm subtypes based on their variation from parent strain. A total of 70 types were obtained representing 53 known emm types with 33 subtypes, 12 sequence-types and five novel MNT strains (Fig.). emm 81 (15.7%) was the highly represented type common to both throat and skin infections. The seven most prevalent types- emm 81 (15.7%), 11 (7.9%), 112 (7.6%), 77 (7.4%), 44 (4.4%), 49 (3.7%) and 15 (3.4%) constituted 50 per cent of the isolates. Certain sequence types, like ST854, TP-c2135, AAB51153 and AAD 28609 recovered from Thailand and India, suggest a possible geographical bias in their isolation. MNT sequences - NS 292 and sp11014/VT-15, a rare type emm 1-2 and one new provisional sequence type (designated, StI129) were also identified. Most prevalent types found in GAS isolates from throat cultures were emm 81 (16.25%), 11 (10.8%), 77 (10%), 49 (4.6%), 75 (4.2%), 15 (3.3%), 71 (3.3%) and 68 (3.3%) as compared to emm types 81 (16%), 112 (15.4%), 44 (10.3%), 85 (5%), 15 and 1-2 (4.5%) from GAS skin cultures. These emm types constitute 56 per cent each of the throat and skin GAS cultures, respectively. Importantly, except for emm 81 and 15, other predominant types from throat infection were different from those in skin infections. Though several emm types were common to throat and skin sites, yet different types were seen in GAS cultures isolated from these sites, e.g., emm 1, 70, 80, 85, 104 and 5 sequence types were exclusively present in GAS skin cultures, emm 33 and 43 in GAS from RF/RHD patients and 33 different emm types were present only in throat GAS cultures. emm 1-2 was seen in both throat and skin GAS cultures. emm types 33, 43, 49, 74, 80, 93, 112 and NT were present in 11 RF/RHD cases. Hence, specific emm types can be associated with pharyngeal, skin and RF/RHD isolates.
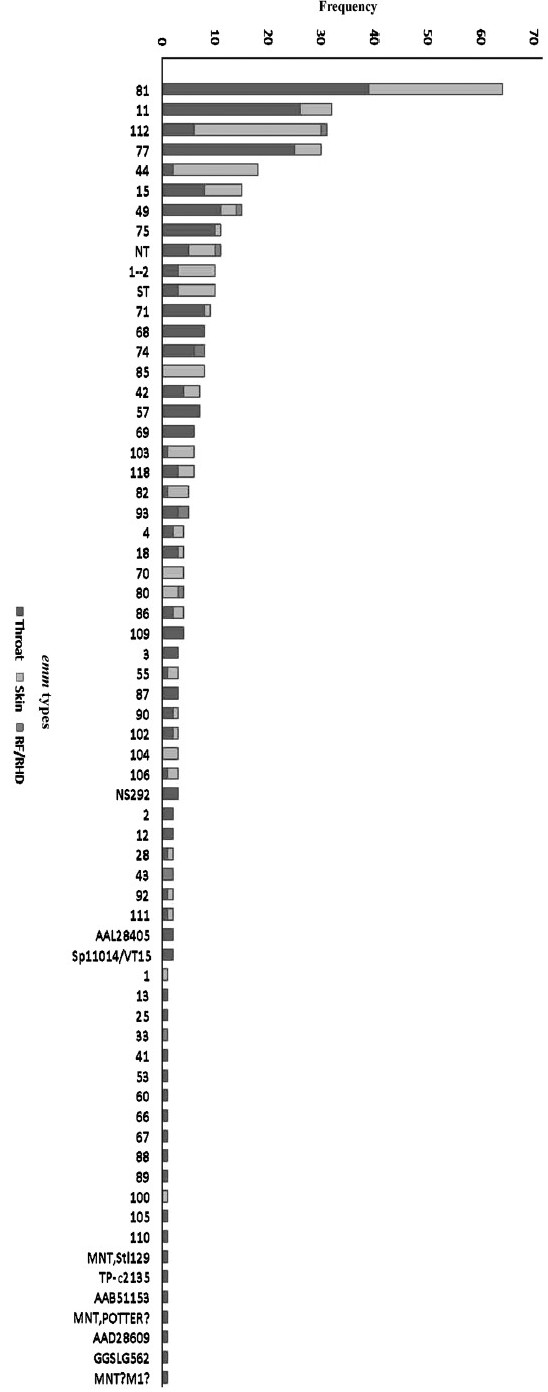
Distribution of emm types among north Indian group A streptococcus isolates.
On comparison with the epidemiological data from south, heterogeneity in GAS emm types was seen from both the regions. Of the 34 GAS isolates from south, 22 different types (64.7% diversity) were observed, the most common being emm 49; and out of 227 GAS isolates 59 emm types were seen with the most prevalent types being emm 112 (12.3%), 82, 11, 105, 108 and 110111217. The first study on streptococcal pharyngitis patients from peri-urban slums near Chandigarh showed presence of emm types- 1-2, 11, 25, 49, 68, 69, 74, 75 and 90 with the most common being emm 49 and 75 (unpublished data). 59 GAS collected from pharyngitis patients visiting Chandigarh hospital and from villages of district Panchkula, Haryana during March 2000-2001 showed 33 different types with emm 74 to be most prevalent7. Later in 2000-2002, a total of 71 GAS cultures were collected from Raipur Rani, Panchkula, Haryana, that were deciphered into 17 different types, being emm 71 to be most prevalent followed by emm 8111. In year 2003, a total of 40 GAS when emm typed showed 23 different types with emm type 49 to be most prevalent in children from the slums, rural and urban areas of Chandigarh10. In 2002-2004, of the 139 GAS collected from rural community of Haryana, 27 different types were observed with emm 81 and 112 to be most common (unpublished data). Recent findings of GAS collected from rural areas of Punjab from 2002- 2007 depict emm 57 to be most prevalent (unpublished data). The pattern of emm type distribution varied from one region to another in north India with the passage of time. Earlier studies from north India showed high diversity of emm types encountered in a single year, but no specific emm type could be associated with the isolation site and those studies stressed upon the selection of emm types for vaccine development and/or need to tailor multivalent vaccine for regional use710. But the present observations indicate that the emm specific vaccine is not going to work in this region.
Surprisingly, only emm 11 was common amongst the six serotypes often seen in USA (emm 1, 3, 4, 11, 12, 28). We further looked for the types considered in the 26 valent multiple-epitope formulation vaccine and found though 50 per cent of those emm types (emm 1, 1-2, 2, 3, 11, 12, 13, 18, 28, 29, 33, 43, 75, 77, 89, 92) were seen in north Indian collection of emm types during the last 12 years; yet their frequency was quite less (around 15.4%) as compared to 80-85 per cent coverage of these types seen in western world18. The emm 81 is not a new emm type19 but predominated as an invasive strain in Sweden also20.
Reports examining the emm type diversity from developing nations support the presence of predominant types. In the Indian literature, only about 30 per cent of clinical GAS isolates were serologically M typed, therefore emm sequencing was initiated21. Our findings support the finding of heterogeneity among Indian strains. No marked preponderance of any single emm type was seen in South9111217. However, in north India substantial year-year, intra-site and inter-site variability in emm type distribution exists79–11, sometimes exceptionally striking, as compared to consistency found in other countries18. The individual GAS serotype enters and leaves a community quickly, however, emm 81 is seen prevalent throughout these years and also from both the north and south regions. Kaplan et al22 also reported displacement of M1 GAS with M6 in USA, further complicating the design of regional vaccines. The factors influencing the distribution of particular emm type are yet to be determined. Hence, it becomes important to monitor continuously the emerging emm types.
The strain variations have been noted within particular M types, and virulence has been linked with a particular isolate rather than being broadly related to a given serotype23. Hence emm types are not always adequate strain markers, because these can be shared by unrelated clonal types also. These observations would be of great significance and imply the efficacy of currently available vaccines may not be successful in India.
Pilot studies to check the protective efficacy of multivalent vaccine as well as considering a peptide sequence containing a conserved epitope from C-repeat region of M protein, were not encouraging724. The knowledge of circulating M types and molecular variants of other candidate antigens in the study population needs to be deciphered.
In conclusion, our findings like heterogeneous emm types encountered from north India, their association with isolation site and their divergence from western world are noteworthy. Regional and temporal variations in the prevalent emm types, emergence of new types and presence of M non-typeable strains in our country highlight better understanding of the present scenario and reveal an urgent need not only to reconsider the vaccine development but an alternative preventive approach to combat streptococcal diseases and their sequelae worldwide.
Authors acknowledge the financial support provided by Indian Council of Medical Research (ICMR) and Department of Biotechnology (DBT), New Delhi.
Conflict of Interest: We declare that we have no conflict of interest.
References
- The global 1.burden of group A streptococcal diseases. Lancet Infect Dis. 2005;5:685-94.
- [Google Scholar]
- World Health Organization. In: The World Health Report. Geneva: WHO; 2004. Available from: http://www.who.int/whr/previous/en/index.html
- [Google Scholar]
- Sequencing 3.emm specific PCR products for routine and accurate typing of group A streptococci. J Clin Microbiol. 1996;34:953-8.
- [Google Scholar]
- Group A streptococcal 4. infections in children. J Paediatr Child Health. 2007;43:203-13.
- [Google Scholar]
- Addressing the burden of group A 5.streptococcal disease in India. Indian J Pediatr. 2004;71:41-8.
- [Google Scholar]
- Immunogenicity of a 26-valent group A streptococcal vaccine. Infect Immun. 2002;70:2171-7.
- [Google Scholar]
- High diversity of group A streptococcal emm types in an Indian community: the need to tailor multivalent vaccines. Clin Infect Dis. 2005;40:46-51.
- [Google Scholar]
- Pharyngeal carriage of group A streptococci in school children in Chennai. Indian J Med Res. 2006;124:195-8.
- [Google Scholar]
- Epidemiology of group A streptococcal pharyngitis impetigo: a cross-sectional follow up study in a rural community of northern India. Indian J Med Res. 2009;130:765-71.
- [Google Scholar]
- Molecular heterogeneity among north Indian isolates of Group A streptococcus. Lett Appl Microbiol. 2004;39:84-8.
- [Google Scholar]
- Heterogeneity of community based pediatric GAS isolates from India: Challenges to the multivalent vaccine approach. In: Sriprakash KS, ed. Streptococci - New insights into an old enemy. Netherlands: Elsevier International Congress Series 1289; 2006. p. :49-53.
- [Google Scholar]
- 12.emm type diversity of beta - a hemolytic streptococci recovered in Chennai, India. J Med Microbiol. 2008;57:540-2.
- [Google Scholar]
- Epidemiologic analysis of group A streptococcal serotypes associated with severe systemic infections, rheumatic fever, or uncomplicated pharyngitis. J Infect Dis. 1992;166:374-82.
- [Google Scholar]
- Prevalence 14.of emm types and antibiotic resistance of group A streptococci in Austria. Diagn Microbiol Infect Dis. 2006;55:347-50.
- [Google Scholar]
- Multicentre surveillance of the prevalence and molecular epidemiology of macrolide resistance among pharyngeal isolates of group A streptococci in the USA. J Antimicrob Chemother. 2006;57:1240-3.
- [Google Scholar]
- Culture, recognition and storage. In: Johnson DR, Kaplan EL, eds. Laboratory diagnosis of group A streptococcal infections (1st ed). Geneva: World Health Organization; 1996. p. :11-20.
- [Google Scholar]
- emm types of Streptococcus pyogenes in Chennai. Indian J Med Microbiol. 2001;19:161-2.
- [Google Scholar]
- Group A streptococcal pharyngitis serotype surveillance in North America, 2000-2002. Clin Infect Dis. 2004;39:325-32.
- [Google Scholar]
- Streptococcal emm types in Hawaii: a region with high incidence of acute rheumatic fever. Pediatr Infect Dis J. 2009;28:13-6.
- [Google Scholar]
- Molecular and clinical characteristics of invasive group A streptococcal infection in Sweden. Clin Infect Dis. 2007;45:450-8.
- [Google Scholar]
- Type-specific antibodies to purified streptococcal M-proteins from potentially rheumatogenic M types in patients with rheumatic fever and rheumatic heart disease. J Med Microbiol. 1996;45:483-9.
- [Google Scholar]
- Dynamic epidemiology 22.of group A streptococcal serotypes associated with pharyngitis. Lancet. 2001;358:1334-7.
- [Google Scholar]
- Variable susceptibility to opsonophagocytosis of group A streptococcus M-1 strains by human immune sera. J Infect Dis. 1999;180:1921-8.
- [Google Scholar]
- M protein conserved region antibodies opsonise multiple strains of Streptococcus pyogenes with sequence variations in C-repeats. Res Microbiol. 2005;156:575-82.
- [Google Scholar]




