
Translate this page into:
Coexistence of emphysematous liver abscess & bilateral emphysematous urinary infection
* For correspondence: 814288678@qq.com
-
Received: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 60 yr old maleꬷ with a long history of diabetes presented to the Emergency department of Fujian Provincial Hospital, Fuzhou, China, in May 2020, with abdominal pain and fever for two days. Physical examinations were remarkable for notable percussion pain over liver and bilateral kidney regions, and he displayed septic shock and a multiple organ dysfunction syndrome when admitted. Blood tests showed that white blood cell (WBC) count, procalcitonin, HbA1c and glucose levels increased to 32.2×109/l [neutrophil percentage (NEU%): 90.0%], 30.0 ng/ml, 13.6 per cent and 24.83 mmol/l, respectively, while liver and kidney function tests were not abnormal. Urine routine test showed bacterial and WBC count increased to 2008/µl and 1875.7/µl, respectively, with qualitative detection of nitrites positive. Computed tomography (CT) revealed a disseminated gas-forming infection in the liver (Figure A) and bilateral urinary tracts (Figure B-D) including kidneys, pelvis, ureters and bladder. He was given percutaneous drainage of the liver abscess, empirical antibiotics [imipenem and cilastatin sodium (IMP/CS)], anti-shock, glycaemic control and organ support treatments, while no any specific intervention was done for the urinary tract, except for indwelling urinary catheterization. Klebsiella pneumoniae sensitive to IMP/CS and ceftriaxone sodium (CROS) was isolated from the drainage fluid, urine and blood. The condition alleviated gradually. Two days after admission, blood tests showed that WBC and procalcitonin decreased to 10.8×109/l (NEU%: 89.6%) and 8.6 ng/ml, respectively. He was transferred to a local hospital three days later on his request where he continued to receive IMP/CS for three weeks, following by CROS for one week. Two weeks after discharge, he finished oral antibiotic course and a follow up showed that he recovered well. Prompt investigations including abdominal CT should be done for appropriate diagnosis and subsequent management of such patients at the earliest.
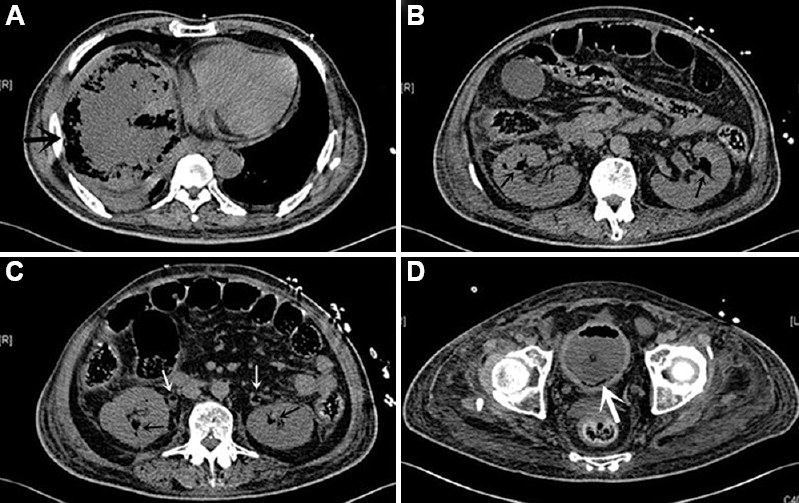
- Concurrent emphysematous liver abscess and bilateral emphysematous urinary infection. Plain CT scans showed (A) a large abscess with gas formation (large black arrow) in the liver; (B and C) bilateral emphysematous pyelonephritis (small black arrows); (C)ureteritis (small white arrows); and (D) cystitis (large white arrow). CT, computed tomography.
Financial support and sponsorship
This work was sponsored by the Startup Fund for scientific research, Fujian Medical University (Grant number: 2018QH1123).
Conflicts of interest
None.
Acknowledgment
CT images were provided by the department of Radiology, Fujian Provincial Hospital (Fuzhou, China)




