
Translate this page into:
Club cell protein 16 as a biomarker for early detection of silicosis
For correspondence: Dr Kamalesh Sarkar, Director, ICMR-National Institute of Occupational Health, Meghaninagar, Ahmedabad 380 016, Gujarat, India e-mail: kamalesh.sarkar@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Clinically silicosis is diagnosed by chest X-ray showing specific opacities along with history of silica dust exposure. Diagnosis is invariably made at an advanced or end stage when it is irreversible. Moreover, silicosis patients are susceptible to develop tuberculosis. Therefore, a suitable biomarker for early detection of silicosis is needed. This study evaluated the suitability of club cell protein (CC16) as a biomarker for early detection of silicosis.
Methods:
This pilot study included 121 individuals from X-ray-confirmed/advanced silicosis, moderate silica dust-exposed workers and healthy controls from western India. CC16 levels were quantified in serum samples through ELISA. Sensitivity and specificity of CC16 values at different cut-off points were calculated in both non-smokers and smokers.
Results:
Serum CC16 level was significantly (P<0.01) decreased in X-ray confirmed advanced silicosis patients (4.7±3.07 ng/ml) followed by moderately exposed workers (10.2±1.77 ng/ml) as compared to healthy non-exposed individuals (16.7±3.81 ng/ml). Tobacco smoking also caused a significant decrease of serum CC16 concentration in both healthy (10.2±1.12 ng/ml) and advanced silicosis workers (2.6±2.28 ng/ml) compared to non-smokers. Sensitivity and specificity of CC16 values were also found to be ≥83 per cent for screening all categories of individuals.
Interpretation & conclusions:
Because of high sensitivity and specificity, serum CC16 could be used as predictive biomarker for suspicion and early detection of silicosis, which would help in reducing/delaying premature deaths caused by silicosis. It would also control silicotuberculosis additionally.
Keywords
Club cell protein
dust exposure
early detection biomarker
serum
silicosis

Silicosis is an irreversible occupational disease of respiratory system caused by the reaction of lung tissue (parenchyma) to dust containing crystalline silica or silicon dioxide of respirable size (<10 μ in diameter). People with varying length of exposure of 2-15 yr or more in the industries like mines, stone quarry, agate, construction sites and non-metallic product manufacturing units such as, refractory, ceramic, glass, mica, structural clay are prone to silicosis1. Although silicosis occurs mostly in the occupational exposure set-up, a sizable number of cases have also been reported due to non-occupational exposure to silica dust234. Unfortunately, most silicosis cases remain undiagnosed at an early stage due to asymptomatic nature of the initial stage of the disease, lack of a suitable biomarker for early detection, poor health-seeking behaviour of the workers and poor occupational healthcare delivery services at the working areas, particularly in unorganized sectors.
Patients with silicosis are prone to develop pulmonary tuberculosis (i.e., silicotuberculosis), probably due to destruction of alveolar macrophages. Differential diagnosis is difficult unless the physician is aware of the occupational dust (silica) exposure history of the workers, which is very subjective in nature. Moreover, superimposition of silicotic nodules and tuberculous infiltration in X-ray film and difficulty in isolation of Mycobacterium tuberculosis from sputum of silicotuberculosis patients as silicotic fibrosis prevents its discharge into sputum, make the situation more complicated5. Therefore, a suitable bio-marker is needed for early detection of silicosis, which would not only prevent or control advanced silicosis cases but also silicotuberculosis, a neglected tropical disease in the developing countries.
A number of anti-inflammatory biomarkers for early detection of silicosis have been tested, but most of these were non-specific and hence found unsuitable for silicosis detection67. The club cell protein 16 (CC16) is one of the potentially immunosuppressive or anti-inflammatory proteins secreted from non-ciliated epithelial cells of bronchoalveolar epithelium89. CC16 is proposed to be a peripheral marker of respiratory epithelial injury that protects respiratory tract against oxidative stress-induced inflammation91011 and passively diffuses in bronchoalveolar-blood barrier to plasma12. CC16 deficiency has been reported to be associated with an increase susceptibility of lung to viral infections and oxidative stress in experimental rodent model131415. In human, a polymorphism of CC16 gene, localized to a region linked to airway diseases has been discovered in association with an increased risk of developing childhood asthma1617 and integrity of lung epithelium18. Though the exact physiological mechanism of CC16 remains unknown, but evidence suggesting significant reduction of CC16 in silica dust-exposed workers with no change in respiratory symptoms, normal chest X-ray and lung function tests1920 indicates that CC16 could be an early asymptomatic detection tool for silicosis and silica-exposed population at risk. Therefore, the present study was carried out to assess the feasibility to develop CC16 as a potential biomarker for early detection of silicosis.
Material & Methods
The study was conducted by the ICMR-National Institute of Occupational Health (ICMR-NIOH), Ahmedabad, India, during the months of March to May, 2018. Prior approval of the study was obtained from the Institutional Ethics Committee. Written informed consent was obtained from each participant before initiation of the study.
A total of 121 persons were included in this pilot study by the convenient purposive samples (n=121) from three different categories, viz., no exposure (healthy controls), moderate dust exposure (ceramic factory workers) and X-ray confirmed silicosis patients (advanced stage). Clinical information was collected through health check-up and personal interview using a semi-structured field-tested questionnaire. Of them, 25 workers were from the sanitary ceramic production industry in Gujarat with varying period (1-8 yr) of silica dust exposure (considered as moderately exposed to silica dust) and 40 workers were X-ray confirmed silicosis patients (i.e., long duration exposure to silica dust) as per International Labour Organization (ILO) classification21 of chest X-ray, who worked in the agate industry in Gujarat and sand stone mines in Rajasthan. Furthermore, 65 age- and sex-matched healthy controls (volunteers coming from ICMR-NIOH) without any occupational history of silica dust exposure were included (9 refused to provide blood samples, hence excluded). Of these healthy controls, 24 were categorized in smoker subgroup (at least 5 cigarettes/day for the last 2 months) because smoking might reduce serum CC16 value like other lung biomarkers22. Those suffering from chronic lung or kidney disease, hypertension, diabetes, exsmokers and with regular intake of analgesics or anti-inflammatory drugs were excluded (n=6) from this study.
Sample collections and processing: Sample collection and processing were done as per the standardized method used in previous study23. For this purpose, venous blood (4 ml) was collected aseptically by trained medical laboratory technicians using Vacutainer needle and holder (Becton Dickinson, USA) and was transported to the laboratory immediately. Serum was separated on the same day and stored at −25°C till serum CC16 analysis was done.
Club cell protein measurement: The concentration of CC16 in serum was determined by ELISA kit specific to human as per manufacturer's protocol (BioVendor, USA). The absorbance was read at 450 nm in a standard microplate reader (BioTek, USA), which was proportional to the concentration of CC16 protein present in the sample and the value was calculated from the standard curve.
Statistical analysis: The normality of the data was checked by Kolmogorov-Smirnov test24. ANOVA (one-way classification) was applied to test the differences in CC16 levels among exposure groups, for smoking and non-smoking subgroups. Sensitivity and specificity analysis at a given cut-off value of serum CC16 was calculated considering the mean values with SDs for healthy non-smokers, moderate silica dust-exposed workers and X-ray confirmed silicosis workers (longer duration of silica exposed)2526. Similarly, cut-off value for healthy smoker and advanced silicosis workers with smoking habit were calculated. The CC16 value for moderate silica dust exposure individuals with smoking habit could not be measured as no individual of this kind was available for participation in this study.
Results
Participants in the smokers group were analysed separately to assess its additive effect over silica-induced lowering of CC16 values in the non-smokers. In this study, about 30.6 per cent (37 of 121) participants were smokers, and of them, 35.1 per cent (13 of 37) had silicosis. Of the 40 X-ray confirmed silicosis workers, 30 (75%) had varying degree of respiratory discomfort including shortness of breath/dyspnoea; 20 per cent of these silicosis patients (n=8) were suffering from silicotuberculosis. However, no such respiratory morbidity was found in the moderately exposed workers to silica dust.
Age and occupational silica dust exposure history of various categories of both the non-smoker and smoker groups are shown in the Table. In the non-smoker group, the mean duration of moderate silica dust exposure was 4.2±3.9 yr in the ceramic industry workers; and the same was 23.1±9.88 yr in the X-ray confirmed advanced silicosis workers from the agate and sand stone mines. Similarly, in the smoker group, 24.3±12.7 yr was the mean duration of silica dust exposure for the advanced silicosis workers.
| Parameters (mean±SD) | Non-smokers (n=84) | Smokers (n=37) | |||
|---|---|---|---|---|---|
| Healthy controls (n=32) | Moderate silica dust-exposed workers (n=25) | X-ray-confirmed/advanced silicosis (n=27) | Healthy controls (n=24) | X-ray-confirmed/advanced silicosis (n=13) | |
| Age (yr) | 37.5±11.41 | 31.7±7.38 | 52.0±8.67**,†† | 38.9±12.55 | 52.8±11.24δδ |
| Duration of exposure (yr) | Nil | 4.2±3.90 | 23.1±9.88†† | Nil | 24.3±12.71†† |
**P<0.01 vs. respective healthy controls, ††P<0.01 vs. moderate silica dust-exposed workers, δδP<0.01 vs. respective healthy controls
CC16 levels in healthy controls, moderate silica dust-exposed workers and X-ray-confirmed advanced silicosis patients: In this present study, mean serum CC16 concentrations were 16.7±3.81, 10.2±1.77 and 4.7±3.07 ng/ml, respectively, in the healthy controls, moderately silica dust-exposed workers and X-ray confirmed advanced silicosis patients without any smoking habit (Fig. 1). In the three X-ray-confirmed silicosis workers, serum CC16 levels were found to be below the detection limit of the ELISA kit (i.e., 46 pg/ml). The results revealed significantly (P<0.01) lower serum CC16 levels in the moderately silica dust-exposed workers and X-ray confirmed silicosis workers compared to the healthy controls in the non-smoker group. In smoker group also confirmed silicosis patients had significantly (P<0.01) lower serum CC16 values compared to healthy controls (Fig. 1). Smoking had an additional lowering effect on serum CC16 levels over the non-smokers in all categories of the individuals (Fig. 1). However, no significant difference of serum CC16 levels was found in X-ray-confirmed silicosis workers of the two different occupational set ups such as, agate industry and sand stone mines.
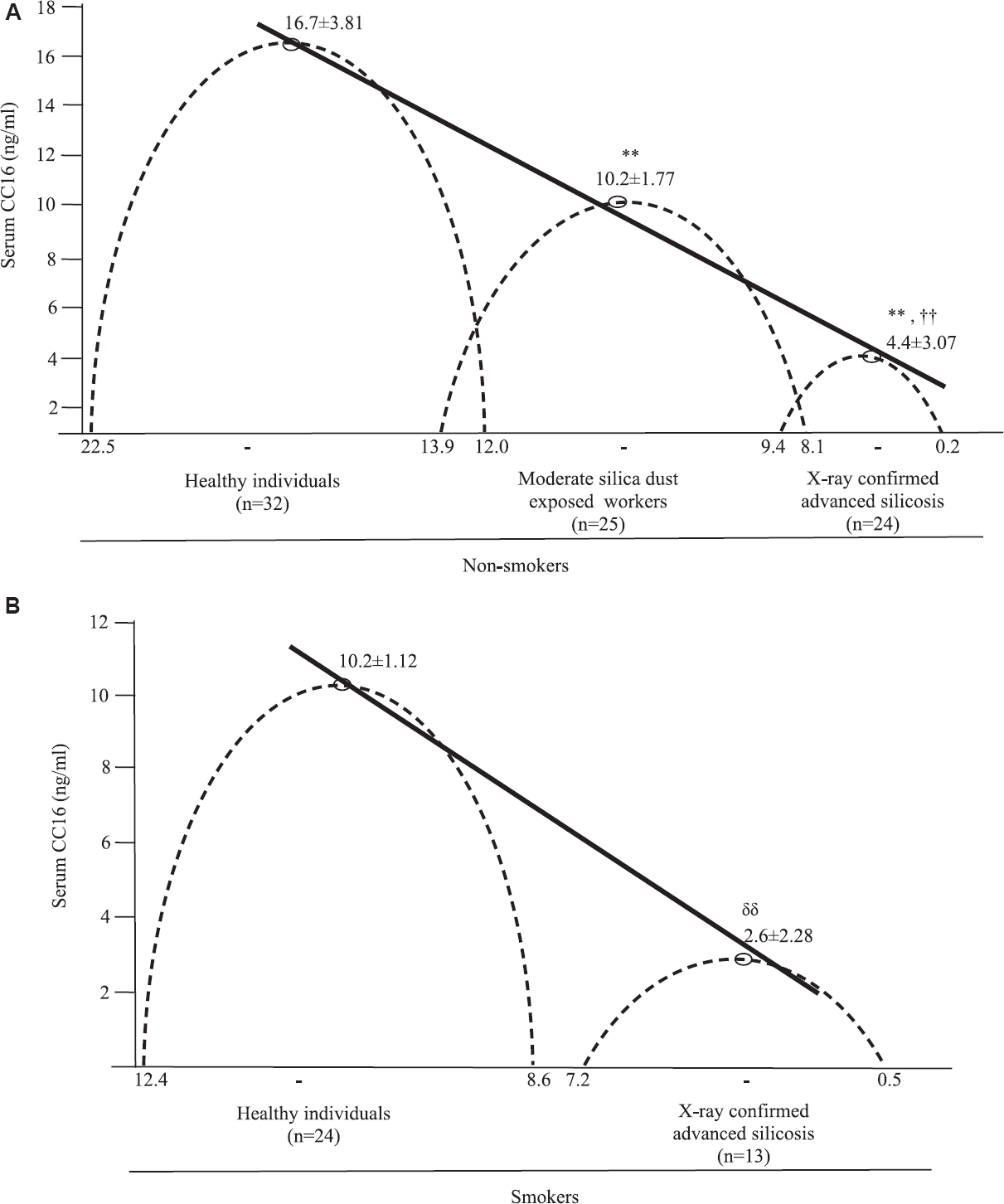
- Mean±SD of serum club cell protein (CC16) levels with range in various categories of non-smoker (A) and smoker (B) groups.**P<0.01 vs. healthy controls, ††P<0.01 vs. silica dust-exposed workers, δδP<0.01 vs. healthy controls.
Sensitivity and specificity of serum CC16 test: There was a continuous fall in serum CC16 levels from 22.5 to 0.2 ng/ml in different categories of the study participants in both the non-smoker and smoker groups. Hence, it was decided to have a cut-off value for each category considering the mean values with SDs, to have the maximum possible sensitivity and specificity at a given cut-off value. In this study, best possible cut-off values were obtained for non-smokers: 13.0 ng/ml to separate out the healthy controls from moderately exposed silica dust and 7.0 ng/ml for separating out X-ray-confirmed/advanced silicosis from moderately exposed asymptomatic individuals (Fig. 2A). With the above cut-off value, sensitivity and specificity were calculated for healthy controls as well as advanced silicosis cases. The sensitivity for the healthy controls was 88 per cent (28/32) and for the advanced silicosis individuals was 92 per cent (22/24). The specificity for healthy controls was 96 per cent (24/25) and for advanced silicosis individuals, was 92 per cent (22/24) (Fig. 2A). In the smoker group, healthy and advanced silicosis individuals had the cut-off values of 9.0 and 5.0 ng/ml, respectively (Fig. 2B). Hence, for healthy smokers, the sensitivity was 83 per cent (20/24), and for advanced silicosis smokers, it was 85 per cent (11/13) (Fig. 2B). However, specificity could not be calculated as true negative could not be found out due to non-availability of the smokers in moderate silica dust-exposed workers.

- Sensitivity and specificity of serum club cell protein (CC16) test at given cut-off values in various categories of non-smoker (A) and smoker (B) groups. Results represent the range and mean of serum CC16 levels with higher and lower side cut-offs.
Discussion
The present study showed a significant reduction in serum CC16 levels in individuals in three different occupational set ups in Western India (Gujarat and Rajasthan), while comparing with the non-exposed healthy controls. Previous studies have shown a decline of serum CC16 levels with silica dust exposure, but no study has conclusively evidenced on healthy, early silica-exposed cases without having X-ray changes and confirmed silicosis cases, and their relationship with serum CC16 values1527. CC16 concentrations in BAL fluid correlate with serum levels, suggesting that serum could be used to infer local CC16 lung biology28. Furthermore, alteration of serum CC16 reflects early toxic effects of silica on the respiratory epithelium of the miners; thus, it ensures the efficiency of CC16 molecule as an early detection marker by using it as a screening tool for suspicion/prediction of silicosis during exposure to silica dust particles in the workplaces8.
Lowering of serum CC16 values by smoking in this study, indicated that tobacco smoking along with silica exposure aggravated the disease progression more among the smokers. Celli and Owen28 corroborated the possibility of CC16 as a modulator of cigarette smoke-induced respiratory morbidity. Park et al22 revealed a reduced serum CC16 level linked with accelerated decline in lung function test after adjustments for age, sex, race, smoking status, airway reactivity and body mass index, etc.
High sensitivity and specificity are essential components for any public health screening program26. As per Florkowski29, sensitivity and specificity are critically dependent on clinical context and vary with the cut-off values chosen for a particular diagnostic test. Serum CC16 protein is not directly related to silicosis, rather it is indicative of the amount of healthy lung tissue available; and in this study, observed values ranged from 22.5 to 0.2 ng/ml from the healthy non-smokers to moderate silica dust-exposed with moderate lung damage to X-ray-confirmed/advanced silicosis with significant lung damage. In the present study, cut-off values of 13.0 and 7.0 ng/ml were considered for the healthy non-smokers to separate out from the early initiation of silicosis (asymptomatic stage) and from early initiated silicosis to the terminal or advanced silicosis, respectively. For smokers, the values of 9.0 and 5.0 ng/ml confirmed additive effect of tobacco smoking. Sensitivity and specificity were reasonably high (83% or above) for screening purpose. Since this was a pilot study with a small number of samples, an in-depth study involving larger population from wider geographic areas of the country is needed to understand the details of serum CC16 cut-off values in the Indian context.
Based on the two cut-off values of non-smokers, serum CC16 levels (13.0-10.0 ng/ml) reflected the early initiation of the process of lung damage caused by silica dust exposure, whereas serum values between 10.0 and 7.0 ng/ml indicated that the process of lung damage though progressed to further extent but still in asymptomatic stage. Tobacco smoking with X-ray confirmed silicosis reduced the cut-off value, suggesting additional destruction of lung epithelium in silico sis with smoking habit. Shinkins et al25 opined that sensitivity and specificity along with cut-off values were useful for reporting the transparent and accurate clinical diagnosis. If periodic screening of silicosis with CC16 is initiated, it would alert the dust-exposed workers regarding their lung health status and would help to delay the advancement of the disease if preventive measures are undertaken.
Since silicosis is an irreversible progressive disease, early detection is beneficial. In absence of a suitable biomarker for early detection of silicosis, the present findings suggest that the low serum CC16 value below or equal to 7.0 ng/ml along with occupational exposure history of silica dust may be an effective biomarker for early detection of silicosis. Early detection of silicosis will also help in reducing silico-tuberculosis in the country.
Acknowledgment
Authors thank Servshri R. Kumar and P. Upadhayay for CC16 ELISA analysis, and Servshri K. Pandit, J. Patel, H. Makwana, K. Pathak, S. Dodia, J.R. Parikh and Dr S Yadav for assistance in field sample collection. Also, voluntary participation of the individuals are acknowledged.
Financial support & sponsorship: This study was funded by an intramural research grant received from the ICMR-National Institute of Occupational Health, Ahmedabad
Conflicts of Interest: None.
References
- Silicosis - An uncommonly diagnosed common occupational disease. ICMR Bull. 1999;29:1-7.
- [Google Scholar]
- Silicosis in a Himalayan village population: Role of environmental dust. Thorax. 1991;46:341-3.
- [Google Scholar]
- Non-occupational exposure to silica dust. Indian J Occup Environ Med. 2012;16:i95-100.
- [Google Scholar]
- Health effects for the population living near a cement plant: An epidemiological assessment. Environ Int. 2012;41:1-7.
- [Google Scholar]
- Biomarkers of silicosis: Potential candidates. Ind J Occup Environ Med. 2005;9:103-6.
- [Google Scholar]
- Biomarkers: A potential prognostic tool for silicosis. Indian J Occup Environ Med. 2012;16:101-7.
- [Google Scholar]
- Early decrease of serum clara cell protein in silica-exposed workers. Eur Respir J. 1994;7:1932-7.
- [Google Scholar]
- Mechanistically identified suitable biomarkers of exposure, effect, and susceptibility for silicosis and coal-worker's pneumoconiosis: A comprehensive review. J Toxicol Environ Health B Crit Rev. 2006;9:357-95.
- [Google Scholar]
- Clara cell 16 protein in COPD sputum: A marker of small airways damage? Respir Med. 2007;101:2119-24.
- [Google Scholar]
- Association of serum clara cell protein CC16 with respiratory infections and immune response to respiratory pathogens in elite athletes. Respir Res. 2014;15:45.
- [Google Scholar]
- Serum clara cell protein (CC16), a marker of the integrity of the air-blood barrier in sarcoidosis. Eur Respir J. 2001;18:507-14.
- [Google Scholar]
- Clara cell secretory protein (CC16): Features as a peripheral lung biomarker. Ann N Y Acad Sci. 2000;923:68-77.
- [Google Scholar]
- Effect of oxidative stress on development of silicosis. World J Respirol. 2012;2:1-5.
- [Google Scholar]
- Club cell protein 16 (CC16) augmentation: A potential disease-modifying approach for chronic obstructive pulmonary disease (COPD) Expert Opin Ther Targets. 2016;20:869-83.
- [Google Scholar]
- A polymorphism of the CC16 gene is associated with an increased risk of asthma. J Med Genet. 1998;35:463-7.
- [Google Scholar]
- Clara cell protein 16 (CC16) gene polymorphism influences the degree of airway responsiveness in asthmatic children. J Allergy Clin Immunol. 2003;111:515-9.
- [Google Scholar]
- Diagnostic values for club cell secretory protein (CC16) in serum of patients of combined pulmonary fibrosis and emphysema. COPD. 2015;12:347-54.
- [Google Scholar]
- Biomonitoring of early effects on the kidney or the lung. Sci Total Environ. 1997;199:205-11.
- [Google Scholar]
- Clearance of clara cell secretory protein 16 (CC16) and surfactant proteins A and B from blood in acute respiratory failure. Am J Respir Crit Care Med. 1998;158:1528-35.
- [Google Scholar]
- ILO International Classification of Radiographs of Pneumoconioses (digital format). Available from: https://wwwiloorg/global/p ublications/books/WCMS_168337/lang--en/indexhtm
- Club cell protein 16 and disease progression in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;188:1413-9.
- [Google Scholar]
- Inorganic lead exposure in battery and paint factory: Effect on human sperm structure and functional activity. J UOEH. 2006;28:157-71.
- [Google Scholar]
- Normality tests for statistical analysis: A guide for non-statisticians. Int J Endocrinol Metab. 2012;10:486-9.
- [Google Scholar]
- Diagnostic accuracy studies: How to report and analyse inconclusive test results. BMJ. 2013;346:f2778.
- [Google Scholar]
- Requirements for minimum sample size for sensitivity and specificity analysis. J Clin Diagn Res. 2016;10:YE01-6.
- [Google Scholar]
- A critical review of the use of clara cell secretory protein (CC16) as a biomarker of acute or chronic pulmonary effects. Biomarkers. 2007;12:445-67.
- [Google Scholar]
- The club cell and its protein, CC16: Time to shine. Lancet Respir Med. 2013;1:757-9.
- [Google Scholar]
- Sensitivity, specificity, receiver-operating characteristic (ROC) curves and likelihood ratios: Communicating the performance of diagnostic tests. Clin Biochem Rev. 2008;29(Suppl 1):S83-7.
- [Google Scholar]




