
Translate this page into:
Chikungunya outbreak in Atmakur village, Medak district, Telangana State, India
* For correspondences: mmurhekar@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Chikungunya is an acute febrile illness caused by chikungunya virus (CHIKV), transmitted by Aedes aegypti and Ae. albopictus mosquitoes which predominantly breed in fresh water12. After an incubation period of 3-7 days (range: 1-12 days), the infected person develops high grade fever (typically >39°C) and poly-arthralgia. Joint involvement is usually bilateral and symmetric, and can be severe and debilitating. Other symptoms may include headache, myalgia, arthritis, conjunctivitis, nausea/vomiting, or maculo-papular rash345. The articular symptoms usually resolve within days to a few weeks, but in some cases, these may last for months or even years6. Even though, the disease is rarely life-threatening, the widespread occurrence of disease causes substantial morbidity and economic loss7.
In 2006, chikungunya re-emerged in India with widespread outbreaks in Andhra Pradesh, Karnataka, Tamil Nadu and Maharashtra8910. According to the National Vector Borne Disease Control Programme, more than 2.7 lakh cases were reported from almost all the States of the country11. Although the disease incidence has shown a decline in India12, outbreaks continue to occur in areas that were not previously affected. On November 12, 2013, the District Medical and Health Officer of Medak district in Andhra Pradesh (this district is now in Telangana State) informed the State Disease Surveillance Unit about unusually high number of cases of febrile illness from Atmakur village (n=1045). On further enquiry, it was found that all the cases presented with joint pain. The State Disease Surveillance Unit, SHARE India and trainee of the field Epidemiology Training Programme of National Institute of Epidemiology, Chennai began investigations during November 15 to December 16, 2013 with the objectives of (i) confirming the aetiology, (ii) estimating the magnitude, (iii) identifying the risk factors, and (iv) proposing recommendations to control.
A suspected case of chikungunya was defined as an acute occurrence of fever with joint pain in a resident of Atmakur since November 1, 201313. Trained community health workers searched for suspected cases of chikungunya by house-to-house visits and collected information about age, sex, location, symptoms, date of onset, information about hospitalization, and duration of illness. A total of 20 serum samples were collected from suspected patients admitted in the district hospital, Medak; and were transported to Institute of Preventive Medicine, Hyderabad, for testing IgM antibodies against CHIKV using IgM-capture ELISA developed by the National Institute of Virology (NIV), Pune, India. The age and sex specific attack rates were calculated by dividing the number of cases by using projected, 2012 population estimates14. The epidemic curve was plotted to describe the distribution of cases by time. Spot map was prepared to understand the distribution of cases.
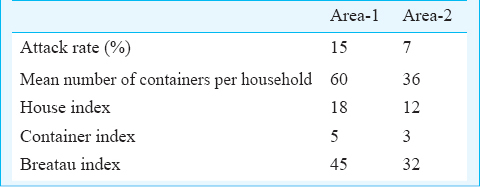
For the mosquito larval survey, Atmakur village was stratified into two areas (area-1 and area-2) by geographic location of houses and 85 households from each of the areas were systematically sampled and surveyed. The household surroundings were searched for the presence of mosquito breeding places like water storage containers, water containers for animals, flower pots, earthen pots, coconut shells, stagnant pits and tyres, etc. House index (HI) was calculated as the proportion of houses having containers with larvae and the Breteau index (BI) as the number of containers positive for mosquito larvae per 100 houses.
A total of 114 suspected chikungunya case-patients were identified from a population of 954 (attack rate: 11.9%; no deaths). All age groups were affected; with higher attack rates among individuals aged 15-45 yr (13.78%) and males (12.3%, Table I). The patients started coming from November 12, 2013, peaked during 15 to 20 November, and subsequently continued to occur for about four weeks. Besides fever (100%) and arthralgia (100%), common symptoms included headache (76%), myalgia (72%), back pain (23%), oedema (20%), nausea (20%), vomiting (18%), and rash (10%). The median number of joints affected was three. The most common joints involved were ankle, knee, wrist, and small joints of hands. Forty three (37.7%) of the 114 suspected patients were hospitalized in the district hospital (n=29) or primary health centre (n=14) for a median duration of eight days. Most of these patients on admission had high-grade fever, severe joint pain, dehydration and headache. At the district hospital, patients were investigated for malaria (peripheral smear), typhoid (Widal test, Span Diagnostics Ltd, Surat, India), and dengue infection (NS1 card test, J. Mitra & Co. Pvt. Ltd, New Delhi, India). All these tests were negative. Ten of the 20 serum samples from the admitted patients were positive for IgM antibodies against CHIKV. Although the sensitivity and specificity for the laboratory assay is high (95 and 97.2%, respectively), the sensitivity of the test in the first week of illness is low. This could be a possible reason for only 50 per cent positivity among the samples tested1315.
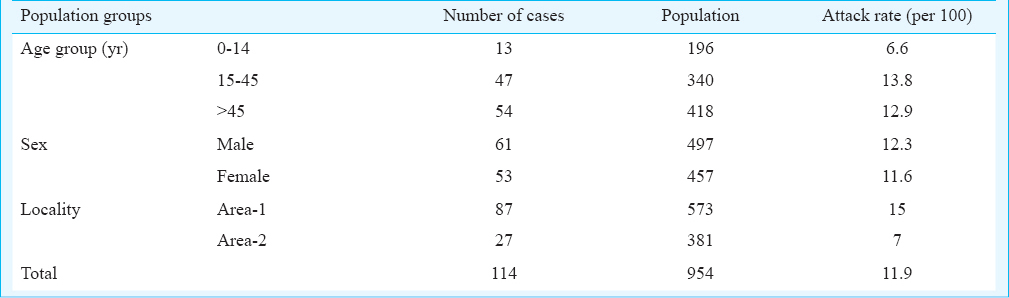
The cases were clustered in area-1 compared to area-2 of the village. Area-2, where houses were made of clay or dried bamboos with no water storage facility had lower attack rate (attack rate: 7%, 27/381). In contrast, the attack rate in area-1 where majority of the houses were pucca houses made with brick and mortar and had plenty of water storage containers was 15 per cent (87/573) (Table I). The mean numbers of containers per household in area-1 and area-2 were six and 11, respectively. The entomological indices were higher in area-1 as compared to area-2 (Table II).
Although only 50 per cent of the samples tested were positive for IgM antibodies against CHIKV, but negative test results for other likely aetiologies (dengue, typhoid, malaria), clinical presentation of cases and entomological findings supported chikungunya as the aetiology of outbreak in Atmakur village.
In conclusion, an outbreak of chikungunya occurred in Atmakur village, Medak district in November-December 2013 affecting about 12 per cent of the village population. High entomological indices and the water storage practices in the village were favourable for the transmission of the infection. As per the guidelines of the National Vector borne Disease Control Programme, the health authorities applied temephos in domestic water storage containers and sprayed indoors with pyrethrum extract spray16. The number of cases declined following these control measures. However, the transmission continued for about one month, as the anti-larval and anti-adult measures were conducted only for one week on alternate days. This finding underscores the need for continuation of vector control activities till the outbreak subsides.
The State of Andhra Pradesh (now Andhra Pradesh and Telangana) experienced large-scale outbreaks during 2005-20068912. The occurrence of this outbreak also indicates that chikungunya remains a risk in previously unaffected areas. Health authorities, therefore, need to institute surveillance for chikungunya outbreaks for detecting and responding early so as to interrupt the transmission to other unaffected areas.
Acknowledgment
Authors acknowledge the services of health personnel of Atmakur PHC staff along with district health authority and State Integrated Disease Surveillance Unit of Medak district, Telangana State, India, for their support. Authors also acknowledge the services of the health personnel of Institute of Preventive Medicine, Hyderabad, for the laboratory work.
References
- Chikungunya fever: an epidemiological review of a re-emerging infectious disease. Clin Infect Dis. 2009;49:942-8.
- [Google Scholar]
- Clinical features and molecular diagnosis of chikungunya fever from South India. Clin Infect Dis. 2008;46:1436-4.
- [Google Scholar]
- Chikungunya fever: clinical manifestations & management. Indian J Med Res. 2006;124:471-4.
- [Google Scholar]
- Epidemiology, clinical manifestations, and diagnosis of Chikungunya fever: lessons learned from the re-emerging epidemic. Indian J Dermatol. 2010;55:54-63.
- [Google Scholar]
- Persistent arthralgia among Chikungunya patients and associated risk factors in Chennai, South India. J Postgrad Med. 2014;60:3-6.
- [Google Scholar]
- Household economic impact of an emerging disease in terms of catastrophic out-of-pocket health care expenditure and loss of productivity: investigation of an outbreak of chikungunya in Orissa, India. J Vector Borne Dis. 2009;46:57-64.
- [Google Scholar]
- Epidemiological investigation of an outbreak of chikungunya in Hyderabad and Nalgonda districts of Andhra Pradesh, India. Int J Health Sci (Qassin). 2007;1:303-8.
- [Google Scholar]
- Chikungunya fever: a re-emerging viral infection. Indian J Med Microbiol. 2008;26:5-12.
- [Google Scholar]
- Chikungunya: Clinically suspected chikungunya fever cases since 2009. National Vector Borne Disease Control Programme. Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India. Chikungunya-Clinically suspected cases since 2008. Available from: http://nvbdcp.gov.in/chik-cd.html
- [Google Scholar]
- Fading chikungunya fever from India: beginning of the end of another episode? Indian J Med Res. 2014;139:468-70.
- [Google Scholar]
- Seroprevalence of chikungunya in southern Odisha. J Family Med Prim Care. 2013;2:33-6.
- [Google Scholar]
- Census of India. Government of India, Ministry of Home Affairs. Available from: http://www.censusindia.gov.in/vital_statistics/SRS_Reports_2012.html
- [Google Scholar]
- Laboratory diagnosis of chikungunya virus: do we really need it? Indian J Med Sci. 2011;65:83-91.
- [Google Scholar]
- Guidelines for containment of cikungunya and dengue epidemic outbreaks. National Vector Borne Disease Control Programme; Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India. Available from: http://nvbdcp.gov.in/Chikun-Guidelines.html
- [Google Scholar]




