Translate this page into:
Beneficiary level factors influencing Janani Suraksha Yojana utilization in urban slum population of trans-Yamuna area of Delhi
Reprint requests: Dr Arun Kumar Sharma, Professor, Department of Community Medicine, University College of Medical Sciences & Guru Teg Bahadur Hospital, Delhi 110 095, India e-mail: arsharma62@gmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Janani Suraksha Yojana (JSY), a conditional cash transfer scheme introduced to improve the institutional delivery rates and thereby reduce the maternal and infant mortality was implemented in all States and Union Territories of India from 2007. The present study was carried out to identify the beneficiary level factors of utilization of JSY scheme in urban slums and resettlement colonies of trans-Yamuna area of Delhi.
Methods:
A cross-sectional community based survey was done of mothers of infants in the selected areas of the two districts by stratified random sampling on a population proportionate basis. Socio-demographic factors, antenatal services availed and distance of nearest health facility were studied. Outcome variable, a beneficiary, was a woman who had ever interacted with the ASHA of her area during the antenatal period of previous pregnancy and had child birth in an institution. Descriptive tables were drawn; univariate analysis followed by multiple logistic regression was applied for identifying the predictors for availing the benefits.
Results:
Of the 469 mothers interviewed, 333 (71%) had institutional delivery, 128 (27.3%) had benefited from JSY scheme and 68 (14.5%) had received cash benefits of JSY. Belonging to Hindu religion and having had more than 6 antenatal check ups were the significant predictors of availing the benefits of JSY.
Conclusion:
There is a need to improve the awareness among urban slum population about the utilization of JSY scheme. Targeting difficult to access areas with special measures and encouraging more antenatal visits were essential, prerequisites to improve the impact of JSY.
Keywords
ASHA
cash incentives
determinants
Janani Suraksha Yojana
institutional delivery
maternal mortality

Maternal mortality ratio (MMR) estimate of 398/lakh live births in 1997-1998 has fallen to 212/lakh live births in 2007-0912. Though this shows a declining trend, the ratio falls very much short of the target of 100/lakh live births set to be achieved by 2012 under National Rural Health Mission (NRHM)3. One of the main strategies to reduce MMR is to improve the skilled attendance at childbirth by increasing the percentage of institutional delivery. Janani Suraksha Yojana (JSY), a conditional cash transfer scheme, was an important step in this direction. The programme envisages achieving a reduction in maternal mortality by providing adequate antenatal care, supervised transportation to institutions for delivery, skilled birth assistance and incentives for care of the newborn and the mother4. The main components of the programme are mobilizing the community with the help of intervention worker named Accredited Social Health Activist (ASHA) and providing cash assistance as an incentive for institutional delivery.
Delhi, classified as a high performing State under JSY due to its better health indicators has a population of 16.75 million5. However, a significant proportion of the population resides in urban resettlement colonies and slums. In one of the reports, the infant mortality rate in urban poor population of Delhi was estimated as 94.4/1000 live births against a State average of 45.9/10006. Hence, ASHAs were selectively posted in slums and resettlement colonies of Delhi. The JSY scheme was implemented in Delhi from 2007. Among the various activities of ASHAs in the community, the activities towards JSY were interacting with the women, motivating them towards institutional delivery and helping them in getting monetary incentives under JSY. The benefits are provided in all Government hospitals and maternity centres to the mothers satisfying the defined eligibility criteria. Women of Delhi with >19 yr age, with either 1st or 2nd child, with proof of belonging to Below Poverty Line (BPL), Scheduled Caste or Tribe (SC or ST) status were eligible for receiving cash benefits.
A separate scheme under the Delhi government, MAMTA scheme was also underway for women who access approved private health care facilities in Delhi. Such hospitals were named as MAMTA friendly hospitals and the eligibility criteria for women under the scheme were similar to eligibility for JSY cash benefits. No distinction was made on the two schemes as women who availed the MAMTA scheme benefits were also eligible for JSY cash benefits7.
The JSY scheme has shown an increasing trend in terms of expenditure under the programme and number of beneficiaries receiving cash benefits under the scheme8. However, there has been no detailed evaluation of the scheme since its introduction in an urban setting like Delhi which vastly varies in terms of socio-demographic profile from other States of India. Also, mere provision of a community health worker and cash incentives are not sufficient conditions for women to be motivated towards institutional delivery. There are several other interacting factors which may play a role in creating a positive environment towards utilizing the services of the community worker and the hospitals. These factors need to be studied for successful implementation of the programme. This study was undertaken to identify the beneficiary level factors of utilization of JSY scheme in urban slums and resettlement colonies in trans-Yamuna area of Delhi.
Material & Methods
The study was conducted from December 2009 to November 2010 in the urban slums and resettlement colonies of the East and North East districts of Delhi (trans-Yamuna area) where the ASHAs were posted under NRHM. This was a cross-sectional community- based evaluation survey where interviewee were the potential beneficiaries viz. mothers of infant (<12 months) who had resided in Delhi during antenatal period and at the time of child birth as they had the opportunity to have been benefited by this scheme.
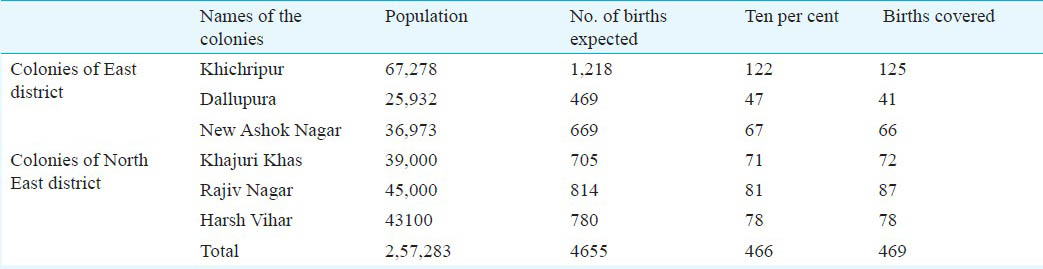
The East and North East districts have 46 and 11 colonies, respectively which had ASHAs posted there. Three colonies were randomly selected from each district. The recent available population details of these areas were obtained from the respective district health authorities and the crude birth rate of Delhi (18.1 per 1000) for the year 2001 was applied on the population to get an estimate of the number of births in one year in each area9. Ten per cent of these estimated births were decided upon as the agreed sample size to be covered by interview on a random basis (Table I). The desired sample size of 466 was covered on a population proportionate basis. The details of population and the births covered are provided in Table I. The mothers who had stayed in Delhi during antenatal period and at the time of delivery were chosen from these areas. Random sampling was adopted where one street in the area was chosen randomly from the last digit of a currency note. All the houses in the chosen street were covered, the subsequent streets were chosen by taking left turn at the end of each street. A new street was chosen randomly once a dead end street was met or there was a repetition of the same street.
A pre-tested interviewer administered structured interview schedule was used for interviewing the potential beneficiaries of JSY. The potential beneficiaries were explained the purpose of the study, assured regarding the confidentiality of the information obtained and an informed written consent was obtained before proceeding with the interview. The information was obtained on the socio-demographic details (name, age, religion, education, income, socio-economic status), obstetric history (place of antenatal check-ups, number of check-ups), place of delivery (home/institutional), awareness about ASHA and the services provided by ASHA during last pregnancy, and the cash benefits obtained via JSY. Ethical clearance for the study was obtained from the institutional ethical committee.
Statistical analysis of the data was done to identify factors of JSY utilization. The outcome variable, that is, a beneficiary of JSY was one who had ever interacted with the ASHA and had child birth in an institutional facility. Univariate analysis was performed using SPSS V 17.0 (SPSS Inc., USA) and statistical significance was assessed by chi square test. Multiple logistic regression was performed to examine the combined effect of all potential predictor variables. Full regression model was developed using all the variables studied followed by developing parsimonious model to obtain the predictors which were most significantly contributing to explaining the variance in outcome variable. This analysis was carried out using STATA (V8.0) (USA).
Results & Discussion
A total of 633 mothers of infants were approached, of whom 469 had stayed in Delhi during their antenatal period and at the time of delivery (25.1% were not eligible). The median age of the mothers was 25 yr (IQR- 23-28). Hindus were the majority with 369 (78.6%) and about 82 per cent (384) were literate and nearly 79 per cent belonged to the lower middle and upper lower classes as per the Modified Kuppusamy Scale of Socio-economic classification with consumer price index for 200710.
A total of 432 (92%) of the women had received minimum three antenatal visits in the last pregnancy with 70 per cent of them having started their antenatal check ups within the 3rd month of pregnancy. The institutional delivery rate was 71 per cent (333) and 52.5 per cent (246) women had delivered in Government Institutions, 19 per cent (87) delivered in private hospitals and 29 per cent (136) delivered at home. The institutional delivery rate varied from 89 per cent in Khajuri Khas area in North East district to 38 per cent in Rajiv Nagar area.
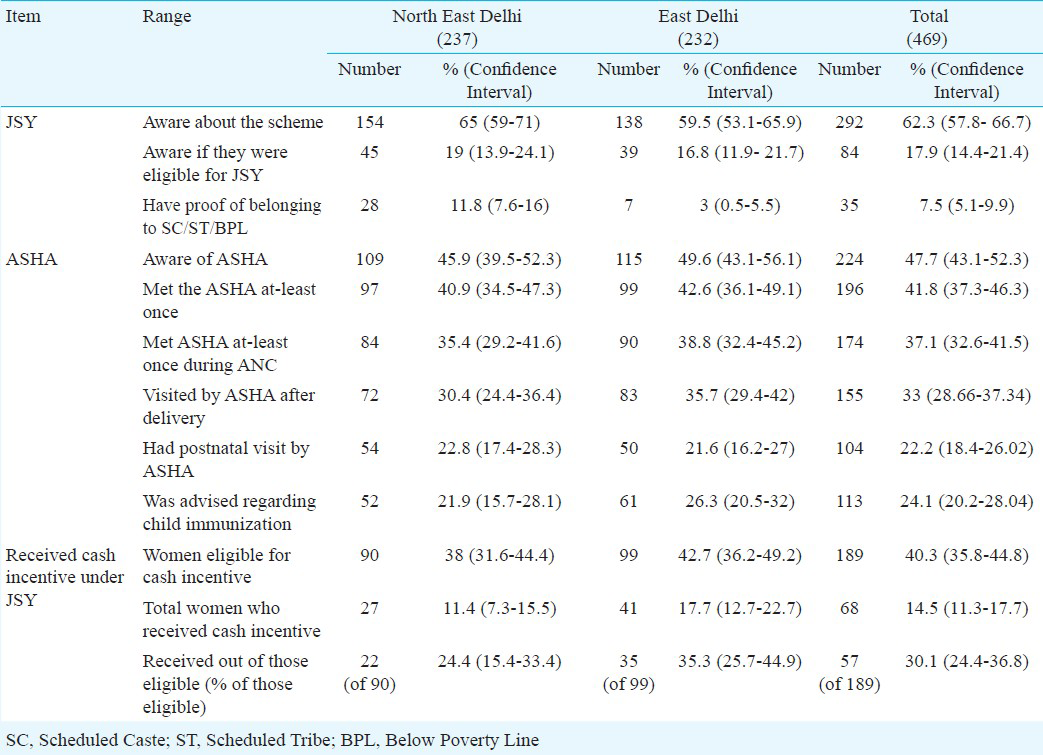
The awareness regarding JSY scheme was 62.3 per cent (292), of whom 72 per cent (211) were not aware if they were eligible for monetary benefits under the scheme. Only 7.5 per cent of the women residing in these slums and resettlement colonies had proof that they belonged to SC, ST or BPL category. Majority of women (68%) came to know about JSY during the antenatal period and place of ANC (51.7%) and place of delivery (40.1%) acted as the major sources of information about JSY with ASHA acting as the third major source (25.7%). Other sources were neighbours (20.5%), relatives/family members (6.5%), media (3.1%) and others (2.7%). Table II shows the awareness and utilization rates of JSY in the two districts of Delhi.
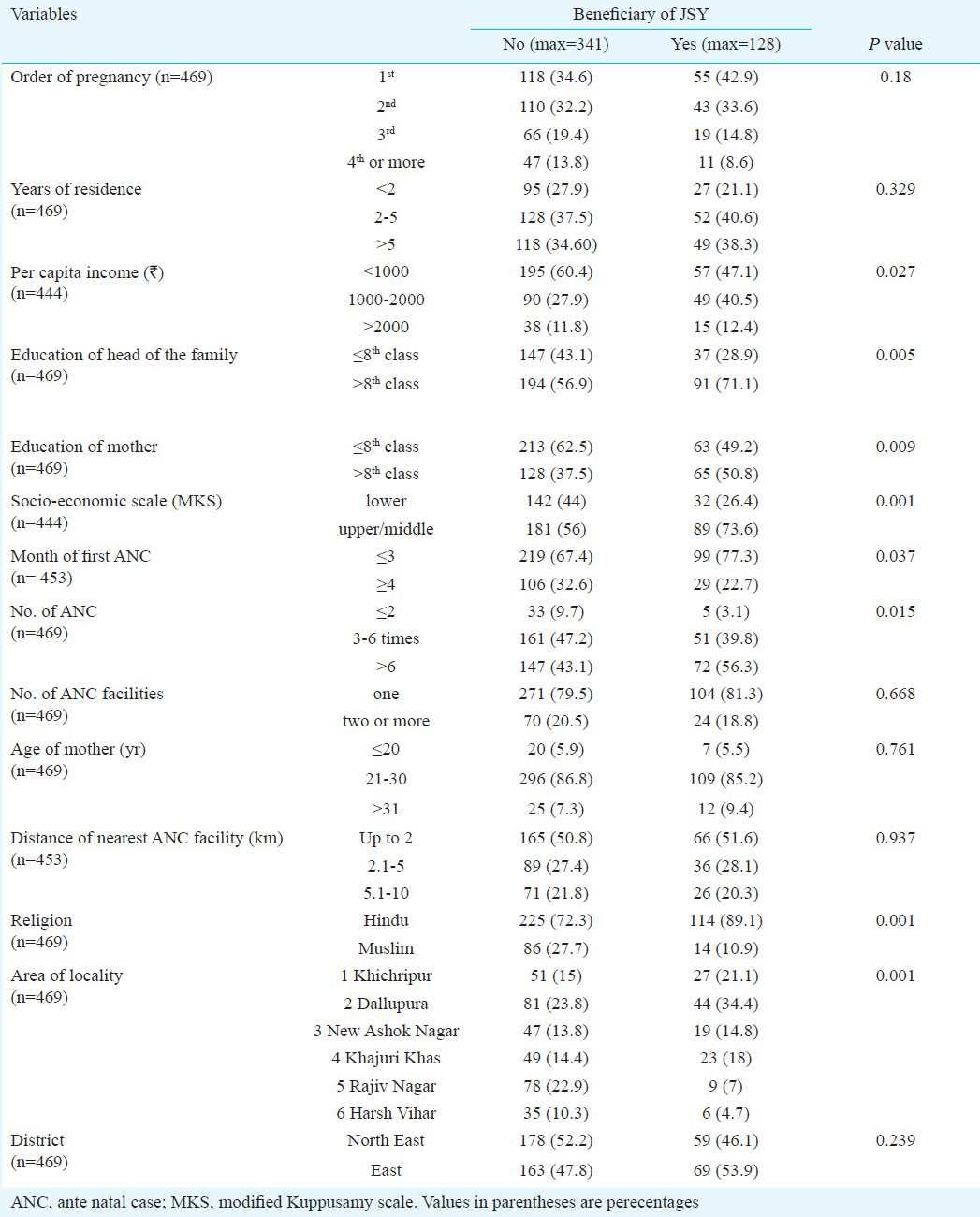
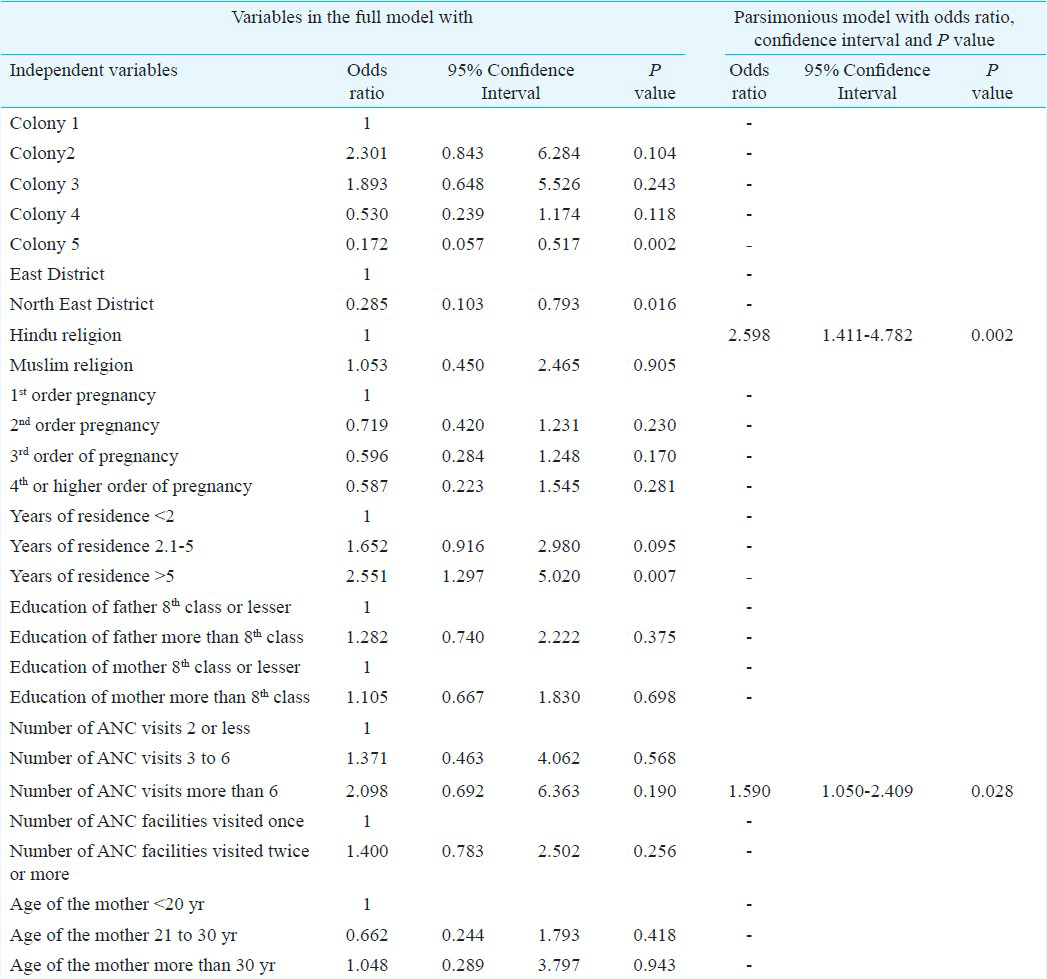
The results of the univariate analysis are presented in Table III. In the full logistic regression model shown in Table IV, place of residence was the only variable significantly associated with the dependent variable. The most parsimonious model (Table IV) showed only two variables, religion of mother and having more than six ANC visits as significant predictors. This was confirmed by the likelihood ratio test (LR chi-square value of 25.54 and the probability obtained was 0.0608 which was not significant).
The awareness about JSY- 62.3 per cent (SE ± 4.5) and the availing of JSY cash benefits of JSY 14.5 per cent (SE±3.2) (Table II) were very similar to results obtained in Coverage Evaluation Survey report 2009 by UNICEF in Delhi which were 62.4 and 14.7 per cent, respectively11. The study results showed a definite improvement in trend comparing the National Family Health Survey-3 (NFHS-3) report on Delhi in terms of percentage of women who had minimum three antenatal visits and institutional delivery rate which were 74.4 and 60.7 per cent, respectively12. Also, the criteria for distributing cash incentive for JSY was not strictly followed in all hospitals in the two districts as five women from North East and six from East district had received cash incentives despite having two or more children. Probable reason would have been misinforming the parity status as this cannot be verified by health workers except ASHA.
In the univariate analysis, per-capita income of less than  1000/- was associated with less utilization of benefits of JSY. Education more than 8th standard of the potential users and that of their husbands and better socio-economic status showed a significant association in the univariate analysis. This shows that the better privileged women utilize the services better. This finding was consistent with the findings of Lim et al13, which showed that the poorest and least educated women did not have the higher odds of receiving JSY benefits and stressed on the need to target these women. But these factors did not turn out to be significant in the regression analysis in our study. Early antenatal check up, higher number of antenatal check ups, religion and locality were the other significant factors in univariate analysis (Table III).
1000/- was associated with less utilization of benefits of JSY. Education more than 8th standard of the potential users and that of their husbands and better socio-economic status showed a significant association in the univariate analysis. This shows that the better privileged women utilize the services better. This finding was consistent with the findings of Lim et al13, which showed that the poorest and least educated women did not have the higher odds of receiving JSY benefits and stressed on the need to target these women. But these factors did not turn out to be significant in the regression analysis in our study. Early antenatal check up, higher number of antenatal check ups, religion and locality were the other significant factors in univariate analysis (Table III).
The logistic regression analysis gave a parsimonious model in which belonging to Hindu religion and having more than six ANC visits during pregnancy were significant predictors of women availing benefits of JSY. Women who utilized the antenatal health care services more than six times were evidently in a better position than others to make use of these facilities to avail the services of ASHA and health care institutions during delivery. Better interaction with the ASHA, increased awareness about the various benefits of a safe child birth in institutions, reduced fear of hospitals and knowledge of cash benefits of JSY could have helped in producing a positive inclination towards institutional delivery. In the full regression model, the place of residence was the only variable which had a significant relation with the availing of JSY benefits and place of residence is related to many other parameters like distance of the nearest hospitals, services rendered by the nearby hospital, accessibility to the nearest hospitals, the transport facilities, awareness about the scheme and overall socio-economic condition of the families in the area.
The limitations of the study include lack of implementation of uniform criteria for determining the beneficiaries of cash benefits of JSY. Some hospitals provided benefits to women with proof obtained from local councilors for BPL status while some restricted to SC or ST women while majority of the eligible women did not have any proof of belonging to SC, ST or BPL status. This did not allow us to have a proper sampling frame of eligible beneficiaries and to determine the utilization rate among eligible women and the determinants of availing cash benefits of JSY among the eligible women. Lack of a defined sampling frame in this survey restricted our options to work with estimates of birth from these areas and choosing the streets randomly instead of households. Crude birth rate of Delhi based on 2001 census was adopted as there was lack of representative and reliable crude birth rate estimates such as that from census for urban slums of Delhi from literature for 2008. But since a decline in crude birth rate is expected in the eight year period after which this study was conducted and the fact that most recent population estimates from these areas were used, the difference in estimated and real births is expected to be less. Also, some of the women in the bordering area of Uttar Pradesh (UP) preferred going to hospitals in UP where the monetary benefits were higher and the eligibility criteria were more relaxed than in Delhi.
In conclusion, our findings show a gap in the awareness and utilization of JSY scheme in the urban slum population. This needs to be addressed via proper information, education and communication drives to improve demand for the scheme. Also, communities belonging to minority religion need special attention for improving utilization. Encouraging more than six antenatal visits showed impact on improving utilization of the Scheme.
Acknowledgment
Authors acknowledge the Indian Council of Medical Research, New Delhi for financial assistance for MD thesis to first author (VK).
References
- Special Bulletin on Maternal Mortality in India 2004-2006 (April 2009). Sample Registration System. Office of Registrar General, India. Available from: http://censusindia.gov.in/Vital_Statistics/SRS_Bulletins/MMR-Bulletin-April-2009.pdf
- [Google Scholar]
- Maternal and child mortality and Total Fertility Rates. Sample Registration System. Office of Registrar General, India. Available from: http://www.censusindia.gov.in/vital_statistics/SRS_Bulletins/MMR_release_070711.pdf
- [Google Scholar]
- Government of India, Ministry of Health and Family Welfare. National Rural Health Mission (2005-2012): Mission Document. Available from: http://www.mohfw.nic.in/NRHM/Documents/NRHM%20Mission%20Document.pdf
- [Google Scholar]
- Government of India, Ministry of Health and Family Welfare, Maternal Health Division, New Delhi. Janani Suraksha Yojana: features & frequently asked questions and answers. Available from: http://mohfw.nic.in/dofw%20website/JSY_features_FAQ_Nov_2006.htm
- [Google Scholar]
- Government of India. Ministry of Home affairs. Office of the Registrar general and Census Commissioner of India. Provisional Population Totals. NCT of Delhi. Available from: http://censusindia.gov.in/2011-prov-results/data_files/delhi/0_PDFC-Paper-1-2011%20NCT%20of%20Delhi_9.pdf
- [Google Scholar]
- Government of India, Government of National Capital Territory of Delhi. Health post. Final report on health status of Urban Delhi. Available from: www.uhrc.in/name-CmodsDownload-index-req-getit-lid-63.html
- [Google Scholar]
- Department of Planning and Evaluation. National Institute of Health and Family Welfare. Evaluation of MAMTA scheme in National Capital Territory of Delhi. Report. 2010. Available from: http://www.nihfw.org/pdf/Mamta%20Report%20full.pdf
- [Google Scholar]
- Government of India. Ministry of Health and Family Welfare. National Rural Health Mission. 3rd Common Review Mission. Available from: http://mohfw.nic.in/NRHM/CRM/CRM_files/Attachment/3rd%20CRM%20Report/3rd%20CRM%20Report.pdf
- [Google Scholar]
- Ministry of Health and Family Welfare. National Rural Health Mission. Health profile of Delhi. Available from: http://www.mohfw.nic.in/NRHM/Health_Profile.htm#del
- [Google Scholar]
- Kuppusamy's socio economic status scale – updating for the year 2007. India J Paediatr. 2007;74:1031-2.
- [Google Scholar]
- UNICEF. Coverage Evaluation Survey Report 2009. State Fact Sheet Reports. Available from: http://www.unicef.org/india/Delhi_Fact_Sheet.pdf
- [Google Scholar]
- International Institute for Population Sciences. National Family Health Survey. Fact sheets for key indicators on final data. Available from: http://www.nfhsindia.org/pdf/Delhi.pdf
- [Google Scholar]
- India's Janani Suraksha Yojana, a conditional cash transfer programme to increase births in health facilities: an impact evaluation. Lancet. 2010;375:2009-20.
- [Google Scholar]




