
Translate this page into:
Autoimmunity strikes neuromuscular junction: Myasthenia gravis & achalasia cardia
*For correspondence: sulenasingh@yahoo.co.in
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 11 yr old male child† presented to division of Neurology, Guru Gobind Singh Medical College & Hospital, Faridkot, India, in September 2019, with persistent vomiting, difficulty swallowing and regurgitation since one year. Examination showed partial ptosis of the left eye with fatigability (Fig. 1).

- (A) Ptosis of left eye at the time of presentation. (B) Improvement in ptosis of left eye after treatment with Pyridostigmine.
Acetylcholine receptor antibody was positive [0.69 nmol/l (Serum reference value <0.25 nmol/l)] and repetitive nerve stimulation test of median and spinal accessory nerve was suggestive of postsynaptic neuromuscular junction disorder - myasthenia gravis (Fig. 2).

- Repetitive nerve stimulation of median nerve at 3 Hz showing significant decrementing responses in Compound Muscle Action Potential (>10%) suggestive of post-synaptic neuromuscular transmission disorder-Myasthenia Gravis.
Upper gastrointestinal endoscopy (Fig. 3) and computed tomography of the chest showed dilated oesophagus (Fig. 4). Barium swallow X-ray and oesophageal manometry showed the failure of the lower esophageal sphincter LES to relax, elevated basal LES pressure and aperistalsis of the oeasophageal body suggestive of achalasia cardia (Figs 5 and 6). The patient was started on steroids, acetylcholinesterase inhibitor (pyridostigmine) and nifedipine. He responded well to the treatment (Fig. 1B) upon follow up after one month.
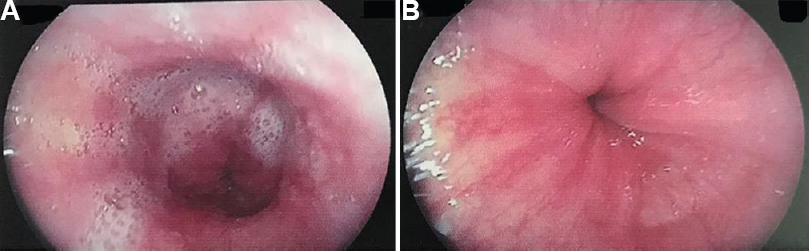
- (A) Upper gastrointestinal endoscopy showing dilated oesophagus and (B) pooled secretions with tight lower oesophageal sphincter.
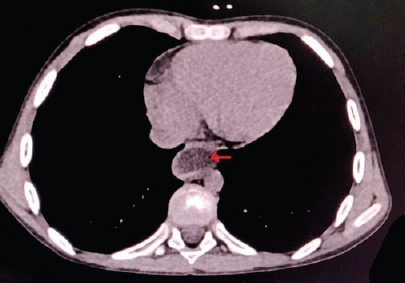
- Arrow in the axial view of computed tomography of the chest showing dilated oesophagus.

- Arrow in the Barium swallow X-ray showing a prominent bird beak sign, oesophageal dilatation and incomplete relaxation of the lower oesophageal sphincter.
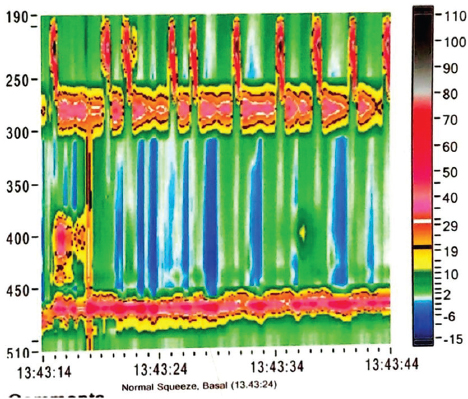
- Oesophageal manometry showing the failure of the lower oesophageal sphincter (LES) to relax, elevated basal lower oesophageal sphincter pressure (51.6 mm of Hg) and aperistalsis of the oesophageal body suggestive of achalasia cardia-type 1.
Coexistence of myasthenia gravis and achalasia cardia in children has not been reported before. Clinicians should keep an open mind to these rarities as these are amenable to treatment with good prognosis.
Conflicts of Interest: None.




