
Translate this page into:
Angiotensin receptor blockers & endothelial dysfunction: Possible correlation & therapeutic implications
Reprint requests: Dr Miroslav Radenković, Department of Pharmacology, Clinical Pharmacology and Toxicology, Medical Faculty, University of Belgrade, P. O. Box: 38; 11129 Belgrade, Serbia e-mail: mradenkovic@med.bg.ac.rs
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
The endothelium is one of the most important constituents of vascular homeostasis, which is achieved through continual and balanced production of different relaxing and contractile factors. When there is a pathological disturbance in release of these products, endothelial dysfunction (ED) will probably occur. ED is considered to be the initial step in the development of atherosclerosis. This pathological activation and inadequate functioning of endothelial cells was shown to be to some extent a reversible process, which all together resulted in increased interest in investigation of different beneficial treatment options. To this point, the pharmacological approach, including for example, the use of angiotensin-converting enzyme inhibitors or statins, was clearly shown to be effective in the improvement of ED. One of many critical issues underlying ED represents instability in the balance between nitric oxide and angiotensin II (Ang II) production. Considering that Ang II was confirmed to be important for the development of ED, the aim of this review article was to summarize the findings of up to date clinical studies associated with therapeutic application of angiotensin receptor blockers and improvement in ED. In addition, it was of interest to review the pleiotropic actions of angiotensin receptor blockers linked to the improvement of ED. The prospective, randomized, double-blind, placebo or active-controlled clinical trials were identified and selected for the final evaluation.
Keywords
Angiotensin II
angiotensin receptor blockers
endothelial dysfunction
endothelial progenitor cells
nitric oxide
renin-angiotensin system

Introduction
Vascular homeostasis and endothelial dysfunction
For a long time the endothelium was considered to be an inert, semi-permeable, monocellular layer, with only one function, and that is to mechanically separate vascular smooth muscle cells from the circulating blood. Today, there is a much better understanding of physiological and pathological features of endothelial cells. All this new information has helped to appreciate that endothelium represents both receptor and effector tissue, with the ability of independently producing substances with agonistic and antagonistic action that can be ultimately released in the blood circulation, and due to which endothelium possesses autocrine, paracrine and endocrine functions1. The substances that are produced by endothelium are among other processes involved in the maintenance of vascular tissue homeostasis through the regulation of blood flow and blood pressure, as well2. It has to be underlined that the modification of vascular tone is the most important function of endothelial cellular layer, although it is not the only one. Hence, endothelial cells also produce compounds that can act as procoagulants or anticoagulants, fibrinolytics or antifibrinolytics, pro-oxidants or antioxidants, as well as many other products involved in the regulation of vascular homeostasis1.
Vascular homeostasis is primarily maintained by the balanced production of endothelial relaxing factors, such as nitric oxide (NO), prostacyclin or group of autacoids with hyperpolarizing activity called endothelium-derived hyperpolarizing factor, as well as endothelial contractile factors namely, endothelin-1 (ET-1), tromboxane A2, angiotensin II (Ang II) or superoxide anion3. The response of different blood vessels to various relaxing and contractile vasoactive substances can be partly or entirely endothelium-dependent, as well as completely endothelium-independent4567. Although endothelium has the ability of producing different vasodilator substances, nearly all stimuli that ultimately produce endothelium-dependent vasodilatation include endothelial NO. In physiological conditions, endothelial NO production is continuous, thus keeping a balance between vasoconstriction and vasodilatation8. On the other hand, a chronic exposure to cardiovascular risk factors such as hyperglycaemia, hyperlipidaemia, hypertension, hyperhomocysteinemia, smoking, sedentary lifestyle, obesity, infections by Chlamydia pneumoniae, Helicobacter pylori, Cytomegalovirus, herpes zoster virus or Bacteroides gingivalis can actually overwhelm endothelial NO production and induce a disturbance in balance between endothelial relaxant and contractile factors. Such pathological condition is defined as an endothelial dysfunction (ED) and it represents the most important, although to some point reversible step in development of atherosclerosis149. In the fundamental nature of ED lies oxidative stress and all the above mentioned risk factors are capable to induce it. Oxidative stress initiates production of proatherogenic cytokines that consequently cause inhibition of NO synthesis1. The inhibition of NO synthesis leads to a shift in balance between endothelial relaxing and contractile factors in favour to autacoids with contractile action. Even though endothelium-dependent contraction is commonly present under physiological conditions, this process is much more pronounced in different pathological conditions associated with ED410.
Angiotensin II and endothelial dysfunction
Though the major problem in ED is considered to be inadequate production of NO, but a significant issue is also the disturbance in the balance between NO and Ang II production1. Thus, depending on the equilibrium of these two endothelium-derived substances, a vasodilatation/anti-atherosclerotic or vasoconstriction/atherogenic effect will prevail. Ang II is one of the most important contractile factors of endothelial cells, which is synthesized to act as physiological antagonist of NO. It is a product of the renin-angiotensin system (RAS). The role of endothelium in this system is to convert Ang I into Ang II, due to angiotensin-converting enzyme (ACE) action located on the luminal surface of endothelial cells (Figure). Yet, even more important is the pathological generation of Ang II within endothelial cells3. This peptide produces its effects through the activation of two types of angiotensin receptors, known as angiotensin type 1 (AT1) and AT2 receptors. After binding to AT1 receptors, Ang II induces vasoconstriction and also prothrombogenic, pro-oxidizing and antifibrinolytic effects. Likewise, it is able to stimulate growth and proliferation factors, to provoke inflammation and to incite expression of proinflammatory and proatherogenic cytokines1. One of the pivotal actions of Ang II lies in its simulative effect on ET-converting enzyme11. ET-converting enzyme degrades the ‘big ET’ to produce ET-1, an important and exceedingly potent vasoconstrictor in blood vessels. Besides all these effects, Ang II is also capable to inhibit NO synthase, which is essential for NO production12.
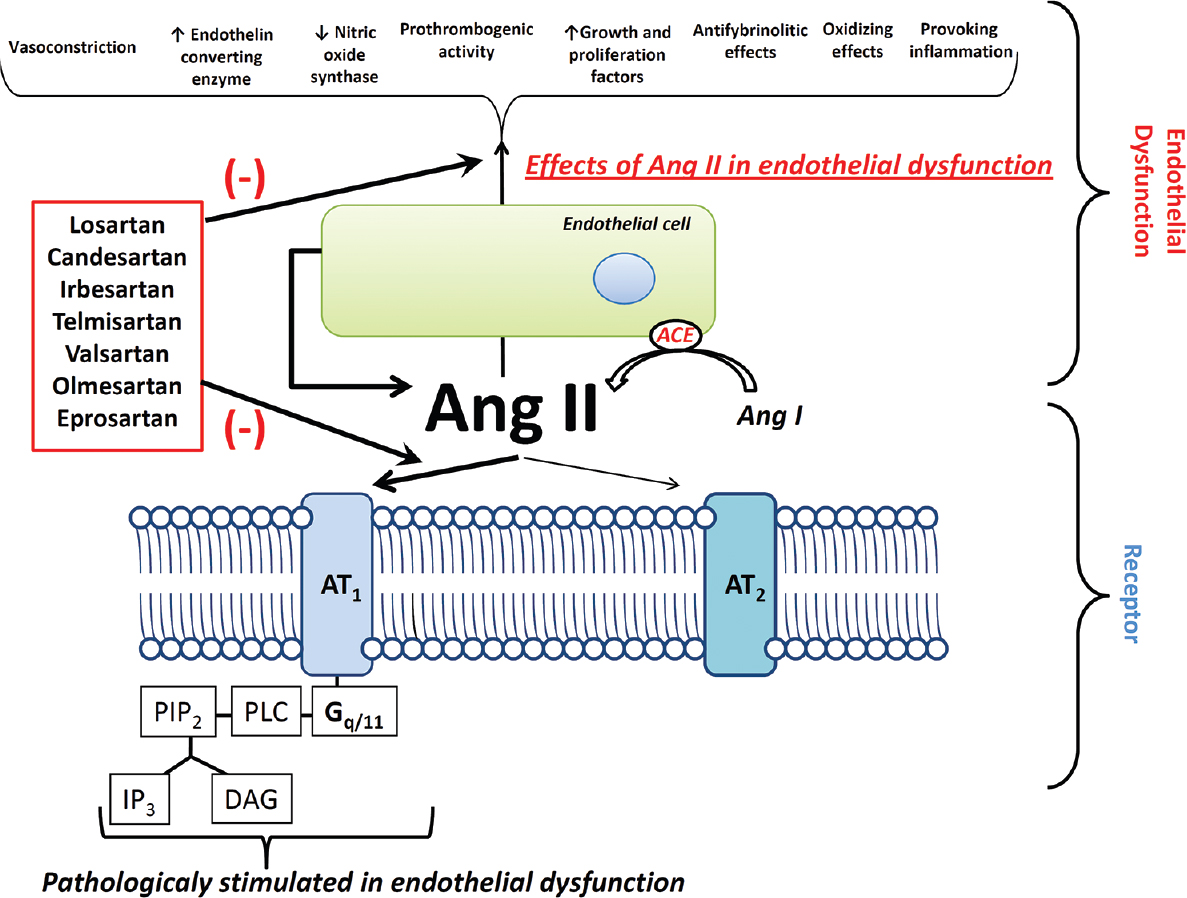
- The action of angiotensin receptor blockers on angiotensin II related endothelial dysfunction. Angiotensin receptor blockers reduce detrimental actions of angiotensin II, wherein the common risk factors are associated with increased angiotensin II production and pathological activation of endothelial cells. Thus, angiotensin receptor blockers partially or completely improve endothelial dysfunction. AT1, AT2, angiotensin type 1, 2 receptors; PIP2, phosphatidyl inositol 4,5 - bisphosphate; IP3, inositol triphosphate; PLC, phospholipase C; DAG, diacylglycerol; ACE, angiotensin converting enzyme.
Angiotensin receptor blockers and possible improvement of endothelial dysfunction
ED associated with different pathological conditions include chronic heart failure, acute coronary syndrome, cardiac syndrome X, hypertension, impaired glucose tolerance (IGT), type 2 diabetes, obesity, peripheral artery disease (PAD), Behçet's disease, polycystic ovary syndrome, ankylosing spondylitis, subclinical hypothyroidism, chronic haemodialysis and hypertension or diabetes in pregnancy491314. Since ED may be a reversible process, there is an increased interest in investigation of different non-pharmacological and pharmacological methods that could improve endothelial function. It has been shown that pharmacological approach is effective in reversal of ED, and this has been confirmed by different clinical studies that have investigated therapeutic efficacy and safety of ACE inhibitors, angiotensin receptor blockers, statins and other lipid lowering agents, calcium channel blockers, some β-receptor blockers, thiazolidinediones, spironolactone or L-thyroxin4.
Taking into account a specific input of Ang II in ED, especially considering negative correlation between Ang II and NO, it can be assumed that drugs with effect on RAS can improve endothelial function. Therefore, angiotensin receptor blockers represent a group of drugs commonly used in the treatment of hypertension as a result of selective binding to AT1 receptors on vascular smooth muscle cells. There is an increasing number of clinical studies indicating that angiotensin receptor blockers not only diminish some important clinical consequences related to cardiovascular disorders, but also prevent further development of different pathophysiological conditions and injuries of vital organs1516. The data indicate that there is a direct relationship between angiotensin receptor blockers and notable improvement or complete reversal of ED1718.
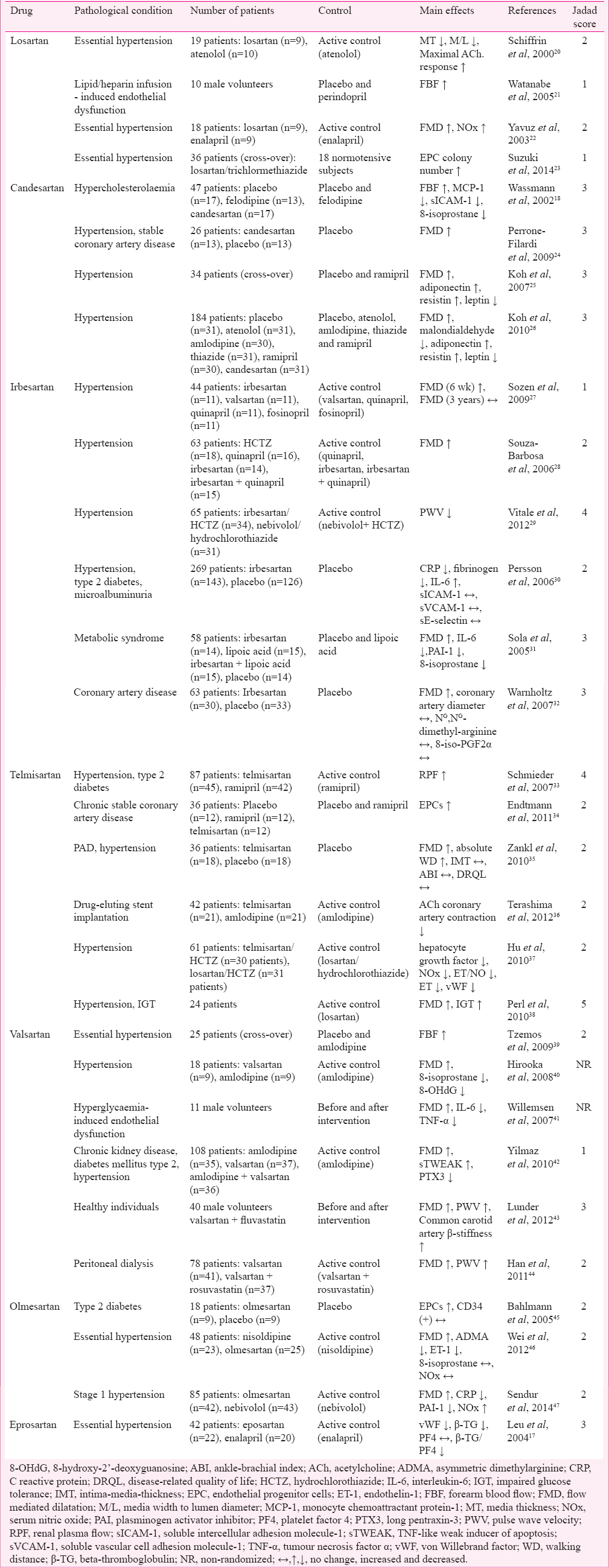
Considering the available data and taking into account that angiotensin receptor blockers have good pharmacological efficacy and adequate safety profile, the aim of this article was to summarize the up to date clinical studies associated with therapeutic application of angiotensin receptor blockers and improvement of ED. In addition, it was of secondary interest to review off-target signalling mechanisms of angiotensin receptor blockers linked to the improvement of ED. Thus, the relevant clinical trials were identified through the search of the MEDLINE and the SCOPUS databases until April 2014. Search terms included: ‘losartan’ or ‘candesartan’ or ‘irbesartan’ or ‘telmisartan’ or ‘valsartan’ or ‘olmesartan’ or ‘eprosartan’ that were combined with ‘ED’. A total of 2786 trials were found. The inclusion criteria for the final evaluation were predominantly aimed to prospective, randomized, double-blind, placebo or active-controlled trials that were written in English language. Finally, a total of 30 clinical trials (28 randomized and 2 non-randomized) were included in this review. In most of selected trials, the effect of angiotensin receptor blockers on ED was investigated in patients with hypertension. Initially, only randomized clinical trials were planned to be included in this review. Thus, the Jadad scoring system19 was used to assess the methodological quality of each randomized clinical trial of interest. The Jadad score ranged between 1 and 5, for the most part with median score 2, whereas only two studies were scored above 3 (Table). Hence, due to poor to moderate methodological quality of the reviewed studies, it was decided to additionally include two non-randomized clinical trials. Finally, to provide a better insight in signalling mechanisms associated with action of angiotensin receptor blockers on ED, corresponding references with relevant experimental data were additionally considered.
Clinical studies related to angiotensin receptor blockers and endothelial dysfunction
Losartan
The effect of losartan on ED was evaluated in a double-blind, prospective study by Schiffrin et al20. In this study, 19 patients with hypertension were randomly assigned to one of two following treatment arms for a given period of one year: losartan 50 mg/day or beta adrenoceptor blocker atenolol 50 mg/day. If the diastolic blood pressure was higher than 90 mmHg, dosage of used drugs was raised to 100 mg or alternatively hydrochlorothiazide (12.5-25 mg) was added (Table). Gluteal subcutaneous biopsies were obtained under local anaesthesia and small arteries (lumen diameter = 150-350 µm) were isolated from subcutaneous tissue. Immediately after the biopsy, arteries were mounted on a pressurized myograph, thus media thickness (MT) and media width to lumen diameter (M/L) ratio were determined. After one year of therapy MT and M/L in resistance arteries were significantly smaller in patients treated with losartan compared to the baseline, while in atenolol-treated patients, these values remained aberrant. Maximal acetylcholine (ACh)-induced endothelium-dependent relaxation, measured with myograph, was significantly improved in vessels after losartan treatment, but not after atenolol treatment, even though the relaxation was similar in these groups at the beginning of study.
In order to investigate the effect of inhibition of RAS on free fatty acid-induced ED, Watanabe et al21 initially induced ED with intra-arterial infusion of lipid/heparin in 10 male volunteers. After that, the subjects were involved in the planned protocol. Namely, each subject received a single oral dose of losartan (50 mg), ACE inhibitor perindopril (8 mg) or placebo four hours before the experiment with forearm blood flow (FBF) in a cross-over fashion, and this was performed over three consecutive days with an interval of at least seven days. Endothelial function was evaluated by changes in FBF during intra-arterial infusion of ACh, which was measured by plethysmography. Lipid/heparin infusion produced a significant reduction in the FBF response to ACh, which could be completely and comparably prevented with a single dose of losartan or perindopril. Additional evidence that RAS inhibition can alter endothelial function was reported by Yavuz et al22. This open-labelled, active-controlled, prospective trial lasted for six months. Twenty four patients with essential hypertension were initially included in the study, as well as 12 normotensive volunteers. Patients were divided into two groups: losartan (50-100 mg/day) and ACE inhibitor-enalapril (5-40 mg/day). Endothelial function was evaluated with flow-mediated dilation (FMD) of the brachial artery, while serum nitrate and nitrite determinations were made by a colorimetric assay. FMD was significantly lower in hypertensive patients than healthy controls at baseline, while it increased significantly in both of the treatment groups at the end of trial. Serum NO metabolite levels were significantly increased in both groups if compared with the baseline values. These results are indicative for the presumption that inhibition of the RAS can improve ED in patients with essential hypertension.
Suzuki et al23 examined if the colony number of endothelial progenitor cells (EPCs), which is an important marker of endothelial damage reparation and neovascularization, was affected by losartan (50 mg/day) or trichlormethiazide (4 mg/day) in patients with essential hypertension compared to the normotensive control subjects. In this prospective, randomized, cross-over and controlled open-label clinical trial, patients were randomly selected to receive losartan at first for four weeks and then trichlormethiazide for four weeks, or vice versa. At the beginning, the number of EPC colonies was notably lower in patients with essential hypertension than in normotensive control subjects, whereas at the end of the planned protocol EPC colony number was significantly increased by treatment with losartan in patients with essential hypertension but not affected by treatment with trichlormethiazide. It was suggested that an improvement of the impaired EPC function in hypertensive patients could be considered as one of the key cardiovascular protective effects linked to the therapeutic use of Ang II receptor blockers.
Candesartan
Since hypercholesterolaemia-induced AT1 receptor overexpression is one of the representative events in the development of ED, Wassmann et al18, conducted a double-blind, randomized, prospective study to investigate whether short-term treatment with the candesartan can influence endothelium-dependent vasorelaxation, as well as inflammation events known to be involved in early and advanced atherosclerosis (Table). In this study, 47 middle-aged, normotensive patients with low-density lipoprotein cholesterol >160 mg/dl were enrolled. These patients were randomized in one of the three treatment groups. The first group received placebo, the second group Ca2+ channel blocker felodipine (5 mg/day), and the third group was treated with candesartan (16 mg/day). Endothelial function was assessed by the measurement of FBF by venous occlusion plethysmography, also venous blood samples were taken to quantify the markers of oxidative stress and inflammatory processes. After six weeks of treatment, hyperaemic FBF was significantly improved by candesartan compared to felodipine. Although blood pressure and cholesterol levels were not significantly altered by any of the drugs used, the level of serum markers monocyte chemotactic protein-1 (MCP-1), soluble intercellular adhesion molecule-1 (s-ICAM-1) and 8-isoprostane were significantly reduced in the group of patients treated with candesartan.
The additional evidence that candesartan can affect ED was shown in a double-blind, randomized, prospective study conducted by Perrone-Filardi et al24. The objective of this study was to verify if candesartan could improve endothelial function in patients with hypertension, stable coronary artery disease (CAD) and ED. With regards to correctly designed inclusion and exclusion criteria, 26 patients who were receiving β-blockers were randomly assigned into two groups for the treatment with placebo or candesartan (16 mg/day). Endothelial function was assessed by FMD of the brachial artery. Two months post-therapy, FMD significantly increased in the candesartan group, but remained unchanged in the placebo group.
Since it has been shown that ACE inhibitors and AT1 receptor blockers can affect endothelial function, Koh et al25 conducted a double-blind, randomized, cross-over trial (three treatment arms and two washout periods) to determine whether ACE inhibitors ramipril and candesartan combined together led to the enhancement of endothelial function in patients with hypertension. The total number of patients enrolled in the trial was 38, while final data from 34 patients were analysed. All patients were randomly assigned to one of the three following groups: ramipril 10 mg/day and placebo, ramipril 10 mg/day and candesartan 16 mg/day or candesartan 16 mg/day and placebo. To determine the endothelial function FMD was performed, also blood samples were obtained in order to quantify insulin, malondialdehyde, adiponectin, leptin and resistin. The results of this study suggest that combined therapy improves ED, insulin resistance, and plasma adipocytokines’ profiles to a greater extent than the monotherapy.
The influence of candesartan on ED in hypertensive patients was also investigated in a randomized, single-blind, placebo-controlled, parallel study performed by Koh et al26. In this study, they compared the effects of several different classes of antihypertensive drugs on ED. After adequately applied inclusion and exclusion criteria, patients were divided into one of the following groups: placebo (n = 31), atenolol 100 mg (n = 31), amlodipine 10 mg (n = 30), thiazide 50 mg (n = 31), ramipril 10 mg (n = 30) and candesartan 16 mg (n = 31). Data from total of 184 patients were analysed. FMD was performed at the beginning of treatment and after eight weeks. The significant improvement in FMD from the baseline was obtained in all groups. However, ramipril and candesartan improved FMD to a higher extent than any other group. Moreover, these two drugs significantly reduced plasma malondialdehyde levels compared to the baseline, although these reductions were not significantly different when compared with other drugs. Patients treated with candesartan were detected with increased levels of adiponectin and resistin, and decreased levels of leptin, when compared with the baseline.
Irbesartan
In order to investigate the effects of RAS-blocking drugs on ED Sozen et al27 designed a double-blind, randomized, prospective study, which included 44 drug-naïve patients with hypertension (Table). Patients were treated with one of the following drugs: irbesartan (300 mg/day), valsartan (160 mg/day), ACE inhibitor fosinopril (10 mg/day) or ACE inhibitor quinapril (20 mg/day). Endothelial function was evaluated by measuring brachial artery diameter, at the baseline, then after six weeks, one and three years of treatment. After six weeks of treatment, all drugs improved endothelial function to a similar extent; but these effects were not maintained during the study, indicating only acute effects of these drugs on endothelial function.
The efficacy of irbesartan and quinapril in improving ED was confirmed in an investigation conducted by Souza-Barbosa et al28. The authors compared whether endothelial function in hypertensive patients would be auxiliary improved after combined therapy with quoted drugs compared to monotherapy-based approach. This was an open, prospective, randomized trial. Sixty three hypertensive patients were divided into four groups (hydroclorothiazide 25 mg/day, irbesartan 150 mg/day, quinapril 20 mg/day or irbesartan plus quinapril), while placebo group consisted of 25 healthy individuals. ED was evaluated with FMD. The results demonstrated that a single-drug antihypertensive therapy improved ED to the same extent as combined treatment.
Vitale et al29 conducted a randomized, double-blind study to examine the effects of irbesartan or beta adrenoceptor blocker - nebivolol (both co-administered with hydrochlorothiazide) on endothelial function in arterial hypertension drug-naïve patients. Thus, 65 patients received irbesartan/hydrochlorothiazide (150 mg/12.5 mg day; n = 34) or nebivolol/hydrochlorothiazide (5 mg/12.5 mg day; n = 31). Endothelial function, which was assessed by the peripheral arterial tonometry, was changed in a similar manner in both groups at the end of treatment.
Persson et al30 conducted a post hoc analysis from the irbesartan in patients with type 2 diabetes and microalbuminuria (IRMA 2) study population to investigate, among other issues, the effects of irbesartan on ED and inflammation biomarker levels. The IRMA 2 study was a 2-year multicentre, randomized, double-blind trial in patients with hypertension, type 2 diabetes and persistent microalbuminuria. Several biomarkers’ levels were determined in 269 patients treated with placebo or irbesartan (300 mg/day). The results showed that irbesartan reduced C-reactive protein (CRP) and fibrinogen and increased interleukin-6 (IL-6) levels, with no effects on any other investigated biomarker.
In order to evaluate the effects of irbesartan and lipoic acid on endothelial function in patients with metabolic syndrome, Sola et al31 created a double-blind, randomized, prospective study named ISLAND (the Irbesartan and Lipoic Acid in Endothelial Dysfunction study). Fifty eight patients were assigned into four groups: (i) irbesartan 150 mg/day plus matching placebo, (ii) lipoic acid 300 mg/day plus matching placebo, (iii) irbesartan 150 mg/day plus lipoic acid 300 mg/day, and (iv) placebo group. Endothelial function was evaluated with FMD. After four weeks of therapy, the significant increase in FMD was observed in all groups, excluding placebo group, with the highest increase in patients concomitantly treated with irbesartan and lipoic acid.
With an aim to test the effects of long-term therapy with irbesartan on both, coronary and peripheral endothelial function in patients with CAD, Warnholtz et al32 designed a prospective and double-blind trial. Initially, 72 patients were randomly assigned into two groups: one treated with irbesartan (300 mg/day) and the other with placebo. Endothelial function of coronary arteries was assessed by measurement of artery diameter change after infusion of cumulative doses of ACh, while in brachial artery, it was assessed by FMD. The results of this study showed that irbesartan improved peripheral, but not coronary ED in patients with CAD without affecting inflammation and oxidative stress markers.
Telmisartan
Considering a pivotal role of kidneys in maintaining overall homeostasis, and also the knowledge that diabetes and hypertension can attenuate vascular system functions, Schmieder et al33 presented results from double-blind, double-dummy, randomized, prospective study, which was aimed to evaluate an impact of telmisartan and ramipril on renal endothelial function (Table). This study included 96 patients with hypertension, type 2 diabetes and filtration rate >80 ml/min, but analysed data of 87 patients finally. The change in renal plasma flow in response to NG -monomethyl-L-arginine (a blocker of NO synthase) served as a measure of renal endothelial function. Consequentially, both drugs significantly increased NO activity.
One study comparing ACE inhibitors and AT1 receptor blockers was performed by Endtmann et al34. In this double-blinded clinical study, 36 patients with chronic stable CAD were enrolled. Patients were randomized to one of the following groups: placebo (n = 12), ramipril (10 mg/day; n = 12) or telmisartan (80 mg/day; n = 12). All patients also received acetylsalicylic acid, β-blocker and statin, except for one patient who did not receive a statin treatment. The primary endpoint of the study was to determine the number of circulating CD34/KDR-positive EPCs in peripheral blood after three months of treatment. The results showed that only telmisartan, but not ramipril or placebo treatment led to significant increased number of circulating CD34/KDR-positive cells.
Since there are only a few treatment options for patients with PAD, Zankl et al35 designed a single-blinded, prospective study in which the effects of telmisartan on absolute walking distance (WD) and endothelial function in 36 patients with hypertension and PAD were studied. Patients were randomized to receive telmisartan or placebo for 12 months. FMD was used to assess the endothelial function, while the effects on PAD were evaluated with absolute treadmill WD. After 12 months, absolute WD and FMD were significantly increased only in the telmisartan group, indicating its positive effects on ED.
ED can also be a consequence of drug-eluting stent implantation (DES) and may be associated with future cardiovascular events. Thus, Terashima et al36 conducted a prospective, randomized study with an aim to compare the effects of telmisartan or amlodipine in patients with DES induced ED. A total of 42 patients finished the trial and were randomized into one of the two groups: telmisartan (40-80 mg/day; n = 21) or amlodipine (5-10 mg/day; n = 21). ED was evaluated by measuring the mean luminal diameter of a 20-mm coronary segment, beginning five mm distal to the stent, before and after infusion of intracoronary ACh and nitroglycerine. The measurements were performed at baseline and three months later. Vasoconstriction induced by ACh infusion was more pronounced in amlodipine compared to the telmisartan group after three months from DES, while results obtained after nitroglycerin infusion did not differ between the groups. These results showed that telmisartan, but not amlodipine significantly ameliorated ED after DES.
There is still not enough evidence that can clarify whether telmisartan is the best choice for improvement of ED compared to other angiotensin receptor blockers. One of the studies that have investigated influence of different angiotensin receptor blockers on ED was performed by Hu et al37. The aim of this study was to examine the effect of combined treatment with angiotensin receptor blocker, telmisartan or losartan and hydrochlorthiazide on blood pressure levels and ED. In detecting the improvement of ED, different biological markers such as hepatocyte growth factor, NO, von Willebrand factor (vWF) and ET were measured before treatment and after eight weeks. All patients were randomly assigned to telmisartan/hydrochlorthiazide (n = 30 patients) or losartan/hydrochlorthiazide (n = 31 patients) group, while 20 healthy individuals were enrolled as controls. The results of this study suggested that the markers of ED were higher in patients with hypertension compared to controls. After eight weeks of treatment, in both groups of patients the parameters representing ED were reduced. However, telmisartan/hydrochlorthiazide (40 mg/12.5 mg) combination was more effective in reducing the level of ET, vWF and ET/NO ratio, compared to losartan/hydrochlorthiazide (50 mg/12.5 mg), while the rest of markers were decreased to a similar extent in both groups. These results indicated telmisartan superiority, if compared to losartan for the improvement of ED. An additional confirmation of telmisartan therapeutic dominance was obtained in a double-blind, randomized, cross-over trial study that investigated vascular and metabolic effects of telmisartan and losartan38. In this trial, endothelial function was assessed by FMD, whereas insulin resistance was assessed by the homeostatic model assessment. This trial included 24 patients with both hypertension and IGT. The results of this study demonstrated that treatment with telmisartan, but not losartan improved ED and insulin resistance. The additional evidence of a significant increase in FMD induced by telmisartan, thus putting in positive correlation between telmisartan administration and an improvement of ED was provided by Takagi and Umemoto48 in the recently published meta-analysis.
Valsartan
Tzemos et al39 designed a randomized, double-blind, placebo-controlled, cross-over study to determine whether valsartan improved ED (Table). Twenty five patients with essential hypertension were recruited for this trial. The patients received either valsartan or amlodipine in a cross-over design, each for 16 wk, with a 3 wk washout period between treatments. The results showed that valsartan, but not amlodipine, produced a significant dose-dependent increase in forearm vasodilatory response to intra-arterial infusions of ACh, as compared with the baseline. The superiority of valsartan in improvement of ED compared to amlodipine in hypertensive patients has been also demonstrated in an open-labelled study by Hirooka et al40. Endothelial function, assessed by FMD, was significantly improved in patients treated with valsartan. Also, markers of oxidative stress were significantly reduced in this group of patients. Additional confirmation of valsartan positive effects on endothelial function was obtained in another study where ED was induced with a sustained hyperglycaemic clamp (12 mmol/l)41. Although hyperglycaemic clamp induced a 40-50 per cent reduction in FMD, the administration of valsartan improved it, which was accompanied with reduction of cytokine in response to an inflammatory stimulus.
To determine the influence of valsartan and amlodipine on ED in patients with chronic kidney disease (CKD), Yilmaz et al42 carried out a randomized prospective study. Only patients with CKD stage 1, with diabetes mellitus type 2 (as the only cause of nephropathy) and hypertension were included. Patients were randomly assigned to one of the following treatment groups: amlodipine (10 mg/day; n = 35), valsartan (160 mg/day; n = 37), amlodipine + valsartan (n = 36). They were followed for 12 wk. This study also included 35 healthy individuals. Soluble tumor necrosis factor (TNF)-like weak inducer of apoptosis (sTWEAK) and long pentraxin-3 (PTX3) concentrations were measured. FMD was also performed during the study period. Consequently, FMD was improved, and PTX3 and proteinuria were reduced in all groups, while sTWEAK values were increased in patients treated with valsartan alone, or in combination with amlodipine.
Except the valsartan/amlodipine combination, valsartan concomitant therapy with statins was also investigated in different clinical trials that assessed the effects of these drugs on ED. A study concerning the effects of valsartan and fluvastatin combined therapy was performed by Lunder et al43. The investigators recruited 40 apparently healthy middle-aged men (between 30 and 50 yr) who were randomly assigned to receive either placebo (n = 20) or a combination of fluvastatin and valsartan (10 mg/20 mg; n = 20) during the period of 30 days. To determine endothelial function, FMD, pulse wave velocity (PWV) and common carotid artery β-stiffness were performed at baseline (0 day), after 30 days, and again 5, 7 and 10 months after the therapy was discontinued. The FMD, PWV and common carotid artery β-stiffness were improved after 30 days in fluvastatin/valsartan treated group. Beneficial arterial effects existed to a certain percentage even after a period of seven months after treatment, but declined substantially after 10 months.
The previous study43 underlined the effect of combined therapy of valsartan and fluvastatin on endothelial function, but it did not evaluate the individual effects of these drugs or their potential additive effects. A prospective, randomized, open-label trial by Han et al44 was aimed to examine potential additive effects of valsartan and another statin (rosuvastatin) on ED. This was a two phase study. In the first phase, patients were treated with valsartan (80 mg/day) for a period of six months. In the second phase, patients were randomized into the first group (n = 41) that continued to receive valsartan, or into the second group (n = 37) that received valsartan + rosuvastatin (10 mg/day) for the additional period of six months. To examine vascular and endothelial function, as well as arterial stiffness, FMD and brachial-ankle PWV (baPWV) were performed. After the first six months, an improvement of FMD and baPWV was noticed in the group treated with valsartan compared to the baseline. In the second part, the significant improvement in FMD and baPWV was spotted only in the group that received combined therapy.
Olmesartan and eprosartan
The effects of olmesartan on ED were investigated in a double-blind, randomized, prospective trial by Bahlmann et al45. In this study, 18 patients with type 2 diabetes mellitus randomly received olmesartan 40 mg/day or placebo for a period of 12 wk (Table). The effect of olmesartan on ED was investigated by determining the number of circulating EPCs. The results of this study demonstrated that treatment with olmesartan significantly increased number of EPCs, but not haematopoietic progenitor cells.
Positive effects of olmesartan on ED were confirmed in a randomized, parallel-group and active-controlled study, which included 55 hypertensive patients at the baseline46. Forty eight patients completed the study. The participants were randomized into two groups, the first treated with Ca2+ channel blocker nisoldipine (10 mg/day; n = 23) and the second group treated with olmesartan (20 mg/day; n = 25). Twenty eight matched normotensive individuals served as healthy controls. This study lasted for eight weeks. Endothelial function was determined with FMD and also by measuring plasma levels of NO, ET-1, 8-isoprostane (also named 8-isoPGF2α), and asymmetric dimethylarginine (ADMA). At the end of the treatment, FMD was found to be improved, while plasma concentrations of ADMA and ET-1 were reduced in both treatment groups. Plasma levels of NO and 8-isoprostane were not significantly different before and after the treatment.
In a study conducted by Sendur et al47, the positive correlation between antihypertensive therapy consisting of olmesartan or nebivolol and improvement of FMD and serum endothelial markers was shown eight weeks after the beginning of treatment. In this randomized, open label study that included 85 newly diagnosed patients with stage 1 hypertension, NO, plasminogen activator inhibitor 1 (PAI-1) and CRP levels were measured and compared before and after the selected treatment. The FMD was significantly and comparably improved after treatment in both nebivolol and olmesartan groups, CRP and PAI-1 levels decreased, while NO levels increased to the same extent in both groups of treated patients. This represents an additional piece of evidence that at least in terms of the therapeutic use of Ang II receptor blocker olmesartan, there is a positive association with endothelial function improvement.
To evaluate whether the inhibition of RAS can affect endothelial function, Leu et al17, conducted a double-blind, randomized, prospective trial in 42 patients with mild to moderate essential hypertension. From the total number of patients who finished the study, 22 patients were randomly assigned to the eprosartan group and 20 to the enalapril group. In this study, NO and vWF were determined, as well as changes in platelet activation indices, such as plasma beta-thromboglobulin (β-TG) and platelet factor 4 (PF-4). After 10 wk of treatment eprosartan (800 mg) significantly decreased the levels of platelet activation (β-TG, PF-4, β-TG/PF-4) and improved endothelial function (vWF). The results were more prominent than after enalapril treatment. Still, the benefit of reduction of platelet activation and endothelial damage was not correlated with the extent of blood pressure reduction.
Pleiotropic actions of angiotensin receptor blockers
Clinical studies as described have shown that angiotensin receptor blockers exerted more than plain antihypertensive action. Thus, molecular mechanisms responsible for the off-target/pleiotropic effects beyond the lowering of elevated blood pressure are still under investigation. Li et al49 in a comprehensive meta-analysis provided an evidence that angiotensin receptor blockers improved peripheral ED as measured by flow-mediated vasodilatation, a widely-used indicator for endothelial function and a surrogate marker of endothelial NO availability. Several other protective mechanisms that are not connected to the angiotensin receptor binding site have been suggested to be important in improving or reversal of ED, both in clinical and experimental conditions.
Losartan was characterized to be positively correlated with an increase of NO metabolite levels, as well as with augmentation of EPCs’ colony number in hypertensive patients2223. In experimental setting, losartan was recently shown to induce positive angiogenic action through neovascularization in peri-infarct area after myocardial infarction in male Wistar rats, thus inducing an increase in capillary density in the infarct border zone50. In Sprague-Dawley nephrectomized rats losartan treatment largely prevented the loss of EPCs and the additional decrease of vascular endothelial growth factor, an important angiogenic factor and another marker of endothelial cell survival51. In isolated thoracic aortas of Wistar rats low-dose atorvastatin or losartan and, especially their combination increased the expression of NOS3 gene (encoding an endothelial NO synthase 3), related to vasodilatation, and decreased the expression of EDNRA gene (encoding an ET receptor type A), related to vasoconstriction52. Treatment with losartan ameliorated the loss in the number and function of EPCs in salt-loaded, stroke-prone, spontaneously hypertensive rats through the significant inhibition of oxidative stress detected by notable decrease of gp91phox, p22phox and p47phox mRNA expression in tissues53.
Hypertensive patients treated with candesartan have been noticed with an improvement in certain markers of endothelial function. Namely, serum markers monocyte chemoattractant protein-1, soluble intercellular adhesion molecule-1, 8-isoprostane, TNF-alpha and PAI-1 were significantly reduced during candesartan treatment in clinical conditions1854. Experimental evidences further indicated that candesartan markedly increased EPCs’ colony number and significantly decreased the expression of NADPH oxidase components (related to excessive production of radical oxygen species), which was shown in salt-loaded, stroke-prone, spontaneously hypertensive rats55.
In patients with type 2 diabetes and microalbuminuria irbesartan reduced CRP and fibrinogen and increased interleukin-6 levels, a finding positively linked to the improvement of ED30. In obese, insulin-resistant JCR: LA-cp rats (representing an animal model of the metabolic syndrome) that exhibited micro- and macro-vascular disease with ischaemic myocardial lesions and renal disease irbesartan was shown to improve ED through the reduction of elevated concentrations of adiponectin, monocyte chemoattractant protein-1 and PAI-156.
Telmisartan is a unique angiotensin receptor blocker showing a peroxisome proliferator-activated receptor gamma binding activity apart from its primary pharmacological action. Knowing that peroxisome proliferator-activated receptor-gamma (PPAR-γ) activation has been shown to prevent endothelial NO-synthase (eNOS) reduction induced by disturbed hemodynamic conditions57, it is not surprising that there are many different clinical and experimental data available in regard to pleiotropic actions of telmisartan connected to the improvement of ED. Thus, clinical administration of telmisartan was shown to be linked with an increase of NO activity, augmentation of the number of circulating EPCs and the reduction in levels of ET and vWF333437. Experimental studies have provided more complex insight in transduction mechanisms related to telmisartan-induced off-target protective vascular actions. It has been reported that in vascular endothelial cells telmisartan increases eNOS activity through the phosphorylation of the most important phosphorylation site for its enzyme activity, namely Ser1177, mainly via p38 mitogen-activated protein kinase (p38 MAPK) signalling58. In Wistar rats, telmisartan prevented aortic ED induced by subcutaneous administration of nitroglycerin through an increase in Ser1177 phosphorylation and concomitant decrease in Thr495 phosphorylation or S-glutathionylation of eNOS59. By using a genome-wide approach in human umbilical vein endothelial cells it has been shown that telmisartan negatively modulates the expression of key genes involved in cell cycle progression and induces a state of endothelial cell quiescence by affecting the Akt/MDM2/p53 and Akt/glycogen synthase kinase-3 β/cyclin D1 signalling pathways, with additional downregulation of proapoptotic genes60. Furthermore, telmisartan prevented monocytic cell adhesion to human umbilical vein endothelial cells exposed to non-uniform shear stress and TNF-α via significant reduction of endothelial vascular cell adhesion molecule-1 expression, and this effect was shown to be related to the activation of PPAR-γ61. Telmisartan induced proliferation of human peripheral blood-derived EPCs in vitro via the phosphoinositide-3 kinase/Akt pathway, yet again through the signalling cascade dependent upon PPAR-γ activation62.
Valsartan, eprosartan and olmesartan have also been positively correlated with protective effects on endothelial cells that, for the most part, are not directly linked with already confirmed pharmacodynamic profile. Thus, clinical experience with the administration of valsartan indicated a significant reduction of detectable oxidative stress and apoptosis markers, as well as the reduction of cytokine in response to an inflammatory stimulus, while eprosartan was positively connected with the improvement of ED by means of the vWF level reduction17404142. Olmesartan is angiotensin receptor blocker that was shown to increase the number of EPCs and NO levels in clinical conditions, and at the same time, administration of olmesartan was linked with reduction of some of the most prominent markers of ED including ADMA, ET-1, CRP and PAI-144454647. Moreover, olmesartan-related positive effects on ED in humans was also connected to the reduction of high-sensitivity TNF-α, IL-6 or monocyte chemoattractant protein-163.
Concluding remarks
Taking into consideration the previous facts, it can be proposed that treatment with Ang II receptor antagonists can improve ED and further delay the development of atherosclerosis and related cardiovascular disorders. Moreover, it seems that improvement of ED associated with this group of antihypertensive drugs is strongly linked with their off-target/pleiotropic actions. Nevertheless, the knowledge obtained from described studies cannot be taken without consideration of certain limitations. Given that Ang II receptor antagonists are primarily used in the treatment of hypertension, most of evaluated studies involved mainly hypertensive patients, thus leaving the question whether these drugs could affect ED of a different origin. The duration of the majority of analysed studies was mainly sufficient to determine the acute effects of these drugs on ED. Hence, it is clear that short-term effects of Ang II receptor antagonists on ED are positive. On the other hand, since several studies conducted for longer periods of time have provided the opposite results, further investigations are necessary to make better estimation in regard to association between angiotensin receptor blockers and the sustained reversal of ED.
Acknowledgment
This article was supported by the Ministry of Education and Science – Republic of Serbia with the Grant 175023.
Conflicts of Interest: None.
References
- Endothelial function and atherosclerosis: circulatory markers with clinical usefulness. Rev Port Cardiol. 2009;28:1121-51.
- [Google Scholar]
- The endothelium: influencing vascular smooth muscle in many ways. Can J Physiol Pharmacol. 2012;90:713-38.
- [Google Scholar]
- Therapeutic approach in the improvement of endothelial dysfunction: the current state of the art. Biomed Res Int 2013 2013 252158
- [Google Scholar]
- Combined contribution of endothelial relaxing autacoides in the rat femoral artery response to CPCA: an adenosine A2 receptor agonist. Scientific World Journal 2012 2012 143818
- [Google Scholar]
- Pharmacological analysis of the rat femoral artery response to bradykinin. Sci Pharm. 2013;81:749-61.
- [Google Scholar]
- Characterization of adenosine action in isolated rat renal artery. Possible role of adenosine A(2A) receptors. Gen Pharmacol. 2000;35:29-36.
- [Google Scholar]
- L-NAME in the cardiovascular system – Nitric oxide synthase activator? Pharmacol Rep. 2012;64:511-20.
- [Google Scholar]
- Endothelial dysfunction: the early predictor of atherosclerosis. Cardiovasc J Afr. 2012;23:222-31.
- [Google Scholar]
- Endothelium-dependent contractions in hypertension. Br J Pharmacol. 2005;144:449-58.
- [Google Scholar]
- Expression of human endothelin-converting enzyme isoforms: role of angiotensin II. Can J Physiol Pharmacol. 2008;86:299-309.
- [Google Scholar]
- The physiological significance of the alternative pathways of angiotensin II production. J Physiol Pharmacol. 2006;57:529-39.
- [Google Scholar]
- Pharmacological evaluation of bradykinin effect on human umbilical artery in normal, hypertensive and diabetic pregnancy. Pharmacol Rep. 2007;59:64-73.
- [Google Scholar]
- Altered response of human umbilical artery to 5-HT in gestational diabetic pregnancy. Pharmacol Rep. 2009;61:520-8.
- [Google Scholar]
- Angiotensin receptor blockers for prevention of new-onset type 2 diabetes: a meta-analysis of 59,862 patients. Int J Cardiol. 2012;155:236-42.
- [Google Scholar]
- Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers for the prevention of migraines. Ann Pharmacother. 2010;44:360-6.
- [Google Scholar]
- A double blind randomized trial to compare the effects of eprosartan and enalapril on blood pressure, platelets, and endothelium function in patients with essential hypertension. Jpn Heart J. 2004;45:623-35.
- [Google Scholar]
- Angiotensin II type 1 receptor antagonism improves hypercholesterolemia-associated endothelial dysfunction. Arterioscler Thromb Vasc Biol. 2002;22:1208-12.
- [Google Scholar]
- Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin Trials. 1996;17:1-12.
- [Google Scholar]
- Correction of arterial structure and endothelial dysfunction in human essential hypertension by the angiotensin receptor antagonist losartan. Circulation. 2000;101:1653-9.
- [Google Scholar]
- Inhibition of the renin-angiotensin system prevents free fatty acid-induced acute endothelial dysfunction in humans. Arterioscler Thromb Vasc Biol. 2005;25:2376-80.
- [Google Scholar]
- Effects of ACE inhibition and AT1-receptor antagonism on endothelial function and insulin sensitivity in essential hypertensive patients. J Renin Angiotensin Aldosterone Syst. 2003;4:197-203.
- [Google Scholar]
- Effects of an angiotensin II receptor blocker on the impaired function of endothelial progenitor cells in patients with essential hypertension. Am J Hypertens. 2014;27:695-701.
- [Google Scholar]
- Effects of AT1 receptor antagonism with candesartan on endothelial function in patients with hypertension and coronary artery disease. J Clin Hypertens (Greenwich). 2009;11:260-5.
- [Google Scholar]
- Additive beneficial cardiovascular and metabolic effects of combination therapy with ramipril and candesartan in hypertensive patients. Eur Heart J. 2007;28:1440-7.
- [Google Scholar]
- Distinct vascular and metabolic effects of different classes of anti-hypertensive drugs. Int J Cardiol. 2010;140:73-81.
- [Google Scholar]
- Drugs with blocking effects on the renin-angiotensin-aldosterone system do not improve endothelial dysfunction long-term in hypertensive patients. J Int Med Res. 2009;37:996-1002.
- [Google Scholar]
- Endothelial vascular function in hypertensive patients after renin-angiotensin system blockade. J Clin Hypertens (Greenwich). 2006;8:803-9.
- [Google Scholar]
- Effects of nebivolol or irbesartan in combination with hydrochlorothiazide on vascular functions in newly-diagnosed hypertensive patients: the NINFE (Nebivololo, Irbesartan Nella Funzione Endoteliale) study. Int J Cardiol. 2012;155:279-84.
- [Google Scholar]
- Irbesartan treatment reduces biomarkers of inflammatory activity in patients with type 2 diabetes and microalbuminuria: an IRMA 2 substudy. Diabetes. 2006;55:3550-5.
- [Google Scholar]
- Irbesartan and lipoic acid improve endothelial function and reduce markers of inflammation in the metabolic syndrome: results of the Irbesartan and lipoic acid in endothelial dysfunction (ISLAND) study. Circulation. 2005;111:343-8.
- [Google Scholar]
- AT1-receptor blockade with irbesartan improves peripheral but not coronary endothelial dysfunction in patients with stable coronary artery disease. Atherosclerosis. 2007;194:439-45.
- [Google Scholar]
- Impact of telmisartan versus ramipril on renal endothelial function in patients with hypertension and type 2 diabetes. Diabetes Care. 2007;30:1351-6.
- [Google Scholar]
- Angiotensin II impairs endothelial progenitor cell number and function in vitro and in vivo: implications for vascular regeneration. Hypertension. 2011;58:394-403.
- [Google Scholar]
- Telmisartan improves absolute walking distance and endothelial function in patients with peripheral artery disease. Clin Res Cardiol. 2010;99:787-94.
- [Google Scholar]
- Protective effect of telmisartan against endothelial dysfunction after coronary drug-eluting stent implantation in hypertensive patients. JACC Cardiovasc Interv. 2012;5:182-90.
- [Google Scholar]
- Fixed-dose telmisartan/hydrochlorothiazide in comparison with losartan/hydrochlorothiazide in decreasing serum hepatocyte growth factor and improving endothelial dysfunction in hypertensive patients. Int Heart J. 2010;51:252-8.
- [Google Scholar]
- Telmisartan improves vascular function independently of metabolic and antihypertensive effects in hypertensive subjects with impaired glucose tolerance. Int J Cardiol. 2010;139:289-96.
- [Google Scholar]
- Valsartan improves endothelial dysfunction in hypertension: a randomized, double-blind study. Cardiovasc Ther. 2009;27:151-8.
- [Google Scholar]
- Effects of valsartan or amlodipine on endothelial function and oxidative stress after one year follow-up in patients with essential hypertension. Clin Exp Hypertens. 2008;30:267-76.
- [Google Scholar]
- Angiotensin II type 1 receptor blockade improves hyperglycemia-induced endothelial dysfunction and reduces proinflammatory cytokine release from leukocytes. J Cardiovasc Pharmacol. 2007;49:6-12.
- [Google Scholar]
- Combined therapy with renin-angiotensin system and calcium channel blockers in type 2 diabetic hypertensive patients with proteinuria: effects on soluble TWEAK, PTX3, and flow-mediated dilation. Clin J Am Soc Nephrol. 2010;5:1174-81.
- [Google Scholar]
- The effects of low-dose fluvastatin and valsartan combination on arterial function: a randomized clinical trial. Eur J Intern Med. 2012;23:261-6.
- [Google Scholar]
- Combined vascular effects of HMG-CoA reductase inhibitor and angiotensin receptor blocker in non-diabetic patients undergoing peritoneal dialysis. Nephrol Dial Transplant. 2011;26:3722-8.
- [Google Scholar]
- Stimulation of endothelial progenitor cells: a new putative therapeutic effect of angiotensin II receptor antagonists. Hypertension. 2005;45:526-9.
- [Google Scholar]
- Effect of nisoldipine and olmesartan on endothelium-dependent vasodilation in essential hypertensive patients. CNS Neurosci Ther. 2012;18:400-5.
- [Google Scholar]
- Effect of antihypertensive therapy on endothelial markers in newly diagnosed stage 1 hypertension: a randomized single-centre study. Anadolu Kardiyol Derg. 2014;14:363-9.
- [Google Scholar]
- A meta-analysis of randomized controlled trials of telmisartan for flow-mediated dilatation. Hypertens Res. 2014;37:845-51.
- [Google Scholar]
- Angiotensin II receptor blockers improve peripheral endothelial function: a meta-analysis of randomized controlled trials. PLoS One. 2014;9:E90217.
- [Google Scholar]
- Effects of angiotensin II blockade on cardiomyocyte regeneration after myocardial infarction in rats. J Renin Angiotensin Aldosterone Syst. 2015;16:92-102.
- [Google Scholar]
- ARB treatment prevents the decrease in endothelial progenitor cells and the loss of renal microvasculature in remnant kidney. Am J Nephrol. 2011;33:550-7.
- [Google Scholar]
- Treatment with low-dose atorvastatin, losartan, and their combination increases expression of vasoactive-related genes in rat aortas. J Cardiovasc Pharmacol Ther. 2013;18:177-83.
- [Google Scholar]
- Losartan improves the impaired function of endothelial progenitor cells in hypertension via an antioxidant effect. Hypertens Res. 2007;30:1119-28.
- [Google Scholar]
- Pleiotropic effects of angiotensin II receptor blocker in hypertensive patients. J Am Coll Cardiol. 2003;42:905-10.
- [Google Scholar]
- Effects of an ARB on endothelial progenitor cell function and cardiovascular oxidation in hypertension. Am J Hypertens. 2008;21:72-7.
- [Google Scholar]
- Irbesartan-mediated reduction of renal and cardiac damage in insulin resistant JCR: LA-cp rats. Br J Pharmacol. 2009;158:1588-96.
- [Google Scholar]
- Pioglitazone and endothelial dysfunction: pleiotropic effects and possible therapeutic implications. Sci Pharm. 2014;82:709-21.
- [Google Scholar]
- Telmisartan activates endothelial nitric oxide synthase via Ser1177 phosphorylation in vascular endothelial cells. PLoS One. 2014;9:E96948.
- [Google Scholar]
- Nitroglycerin-induced endothelial dysfunction and tolerance involve adverse phosphorylation and S-glutathionylation of endothelial nitric oxide synthase: beneficial effects of therapy with the AT1 receptor blocker telmisartan. Arterioscler Thromb Vasc Biol. 2011;31:2223-31.
- [Google Scholar]
- Telmisartan exerts pleiotropic effects in endothelial cells and promotes endothelial cell quiescence and survival. Arterioscler Thromb Vasc Biol. 2013;33:1852-60.
- [Google Scholar]
- Telmisartan prevents VCAM-1 induction and monocytic cell adhesion to endothelium exposed to non-uniform shear stress and TNF-α. Clin Hemorheol Microcirc. 2011;48:65-73.
- [Google Scholar]
- Telmisartan induces proliferation of human endothelial progenitor cells via PPARgamma-dependent PI3K/Akt pathway. Atherosclerosis. 2009;205:376-84.
- [Google Scholar]
- Effect of angiotensin receptor blockade on endothelial function: focus on olmesartan medoxomil. Vasc Health Risk Manag. 2009;5:301-14.
- [Google Scholar]




