
Translate this page into:
An intervention to evaluate & improve handling of cancer drugs in a tertiary care hospital in India
*For correspondence: anax.navin@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Cancer chemotherapeutic agents have a relatively lower safety margin, and medication errors can be potentially fatal in these patients. Oncology nurses and ancillary support personnel are at risk of exposure to cancer drugs in their workplaces due to environmental contamination or personal exposure. Evidence in support of adverse reproductive outcomes and increased cancers in healthcare workers is available1. The presence of drug residual on several surfaces in hospitals suggests that healthcare workers may be susceptible to exposure through dermal contact2. A study conducted in Italy revealed a large amount of cyclophosphamide on various surfaces in a hospital with no such findings in another comparable hospital. These results could be attributed to the efficacy of cleaning procedures and working practices by hospital staff3. The hospital staff should be aware of the potential health risks of handling hazardous drugs and recommended guidelines to prevent occupational exposure4. This study was conducted with an objective of evaluating the medication management practices associated with cancer drugs in a tertiary care teaching hospital in north India.
The study team developed a set of guidelines based on the American Society of Health-System Pharmacists Guidelines5 for handling of cancer drugs. This was used as an interventional tool for educating the hospital staff, patients and their attendants. A cross-sectional questionnaire-based study was conducted at Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, India, from October 2014 to April 2015 to evaluate the impact of this intervention. Amongst the main stakeholders associated with cancer chemotherapeutic drugs in the hospital (i.e. nursing staff, housekeeping staff and patients and their attendants), 110 consented to participate in the study. The study participants were provided training through lectures and a booklet prepared by the study team. The knowledge and practice of the participants regarding cancer drugs were evaluated pre- and post-intervention using a self-administered semi-structured questionnaire developed in-house. This questionnaire was validated by doing a pilot study on a sample of target population, which was subsequently reviewed and approved by the Ethics Committee of the PGIMER, Chandigarh. For every question, a correct response was given a score of two and a wrong answer was given a score of zero. Many questions had multiple-correct answers, in which case a participant getting it entirely right was given a score of two, partially right a score of one and zero for a completely wrong answer. The study participants provided written informed consent and the study was approved by the institutional ethics committee (vide reference number NK/1534/MHA/5674-75).
Paired t test was used as a test of significance. All statistical tests were two-sided and performed using SPSS for Windows (version 17.0; SPSS Inc., Chicago, IL, USA).
The study sample consisted of 25 nurses, 22 housekeeping staff, 27 patients and 36 attendants of patients. Females comprised 56 per cent (n=62) of this sample and 90 per cent of the sample had an age of <50 yr. The work experience of the participating nurses ranged from a minimum of one year to a maximum of 10 yr, with a mean of 3.3±2.6 yr. The participating housekeeping staff had a mean work experience of 4.5±2.5 yr ranging from a minimum of one year to a maximum of 10 yr.
The housekeeping staff scored 79 of a maximum possible of 176, with a mean score of 3.59 per staff (of a maximum possible of eight), ranging from a minimum score of one to a maximum score of seven. The staff showed a significant improvement post-intervention with a total score of 172 and mean score of 7.81 per staff (P =0.001) (Table). There was a significant improvement shown with respect to knowledge of procedure regarding cleaning of drug spills and disposal of cancer chemotherapeutic drugs (P <0.05). None of the housekeeping staff was found to be using all the required personal protective equipment (PPE), but post-intervention, 95.45 per cent were found using them. The nurses managed a score of 278 of a maximum possible of 500, with a mean score of 11.12 per nurse out of a maximum possible of 20. The pre-intervention scores ranged from a minimum of six to a maximum of 17. Post-intervention, the total score of the nurses increased to 446 with a mean score of 17.84 per nurse. Thus, the results showed a significant improvement in the practice and knowledge level of the nurses in the post-intervention phase (P =0.001) (Table). The results showed that only 40 per cent of the nurses verified drug-related relevant aspects such as drug name, drug dosage and expiry date before drug administration in the pre-intervention phase. The knowledge and practices amongst the nurses related to these factors showed a significant improvement in the post-intervention phase (P <0.05). However, some practices such as preparation of cancer drug in a designated area did not show a significant improvement amongst the nurses. Only 64 per cent of the nurses (n=25) had undergone some skill enhancement programme or continuing medical education.
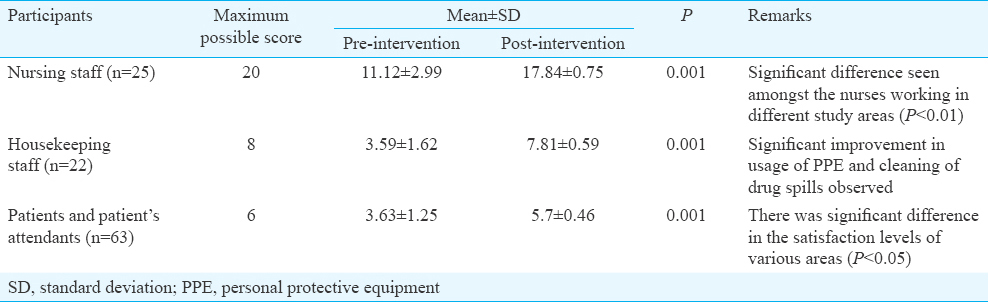
The patients and their attendants were evaluated for issues concerning their knowledge regarding various aspects related to cancer drugs such as use of PPE, drug side effects and response to adverse drug reactions. The patients/attendants scored a total of 228 of a maximum possible of 378 in the pre-intervention phase with a mean score of 3.63 of a maximum possible of six per participant and ranging from a minimum of one to a maximum of six. On evaluation after intervention, the participants scored a total of 354 with a mean score of 5.7 per participant and ranging from a minimum of five to a maximum of six. This improvement in the knowledge level was found to be significant (P <0.05). In the post-intervention phase, 96.82 per cent of the patients/attendants claimed that they were fully informed about their treatment by their caregivers. This was found to be a significant (P <0.001). Similarly, 73 per cent of the participants said that nursing staff had cross-checked their identity every time before administering drug while 26.98 per cent conveyed that the staff occasionally checked their identity in the pre-intervention phase. This improved significantly in the post-intervention phase (P =0.001) with all the participants claiming that their identity was cross-checked every time before drug administration.
This study showed that knowledge and practice of hospital staff about cancer drugs were not to the level required to mitigate the risks associated with handling of these drugs. The post-intervention evaluation revealed a significant improvement in the knowledge levels and practice. Hanafi et al6 obtained similar results in their study. Pagliaro et al7 claimed to have prevented 12 cases of misidentification of patients while administering drugs by following the practice of double-checking. In our study, only 56 per cent of nurses were found to be double-checking the identity of their patients which increased to 100 per cent post-intervention. A study done in Turkey8 found that improvement in knowledge was seen with both verbal and written information. This study showed that 44 per cent of the nurses gained information and training through experience only which corresponded with the results of another study on nurses in Malaysia9.
This study had two important limitations. First, the study period was short. Second, the study findings could not be applied to all the health professionals in the healthcare setting. Therefore, studies of similar kind should be conducted among all treatment areas and various cancer chemotherapy centres so as to improve knowledge, awareness and practice of cancer drug management.
Acknowledgment
Authors thank the study participants, Nursing Department and Sanitation Department of Post Graduate Institute of Medical Education & Research (PGIMER), Chandigarh.
Conflicts of Interest: None.
References
- Preventing occupational exposures to antineoplastic drugs in health care settings. CA Cancer J Clin. 2006;56:354-65.
- [Google Scholar]
- Antineoplastic drug contamination on the hands of employees working throughout the hospital medication system. Ann Occup Hyg. 2014;58:761-70.
- [Google Scholar]
- A case study: Surface contamination of cyclophosphamide due to working practices and cleaning procedures in two Italian hospitals. Ann Occup Hyg. 2005;49:611-8.
- [Google Scholar]
- Safe handling of hazardous drugs: Are you protected? Clin J Oncol Nurs. 2009;13:433-9.
- [Google Scholar]
- American Society of Health System Pharmacists. ASHP guidelines on handling hazardous drugs. Am J Health Syst Pharm. 2006;63:1172-93.
- [Google Scholar]
- An educational intervention to improve nurses’ knowledge, attitude, and practice toward reporting of adverse drug reactions. Iran J Nurs Midwifery Res. 2014;19:101-6.
- [Google Scholar]
- Do undereducated patients read and understand written education materials. A pilot study in Isparta, Turkey? Scand J Rheumatol. 2001;30:99-102.
- [Google Scholar]
- Improving safety-related knowledge, attitude and practices of nurses handling cytotoxic anticancer drug: Pharmacists’ experience in a general hospital, Malaysia. Asian Pac J Cancer Prev. 2013;14:69-73.
- [Google Scholar]




