Translate this page into:
Unravelling the role of ADAM 33 in asthma
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Asthma, a chronic inflammatory disease of the airways, mediated by a Th2 dependent inflammation is an important cause of morbidity in both children and adults worldwide1. It is associated with recurrent bouts of cough and wheezing and some of the main concerns are non-responsiveness to steroids, progressive and accelerated lung function decline in a sub-set of patients1. The prevalence of asthma in many countries around the world is around 5 per cent in adults and 10 per cent in children1. In a large multicenter study in India, the prevalence of asthma was lower and estimated to be about 2.4 per cent among the Indian adults2. The smaller percentage still translates to a huge burden of disease in the community taking into account the population of India.
Asthma is a complex disease which needs significant genetic and environmental interactions for the disease to manifest34. A large number of genes have been identified to have an association with asthma in case-control, family and twin studies56. One of the first genes to be discovered in the Caucasian population was ADAM33 by Eerdewegh et al in 20027. Since then, many studies have confirmed the association of ADAM33 polymorphisms and its association with asthma, though many studies have not been able to replicate the same polymorphisms in different ethnic populations5. ADAM33 polymorphisms have been associated with asthma in the Caucasian, African American, Dutch, US White, US Hispanic, Korean, Japanese, and North Indian but not in Latino, Mexican and south Indian population8910.
ADAM 33 is a disintegrin and metalloproteinase glycoprotein11 involved in intercellular and cell-matrix interactions and plays an important role in both health and disease. In normal subjects, these proteins are involved in fertilization, myogenesis, neurogenesis, inflammatory response and apoptosis112 and exert their role by proteolysis, cleavage or influencing cell adhesion and cell signalling11. It could be important for normal lung development in the embryo as the expression of ADAM 33 can be observed as early as 8-12 wk after gestation311. It could be involved in determining lung functions throughout life13. Several studies have demonstrated an association between ADAM33 and various features of asthma such as bronchial hyperresponsiveness1415, progression of wheezing illness16, airway remodelling1718, lower lung functions19, accelerated lung function decline17, higher specific airway resistance in children 3 yr of age2021 and in one study, even though subjects used steroids (inhaled and in some cases even oral) regularly, it did not influence ADAM33 expression suggesting steroid non-responsiveness in these subjects1. ADAM33 has been associated with intermediate asthma phenotypes such as atopy or elevated total and specific serum IgE levels and skin test responsiveness in some studies1218 but not in others1620. Identification of ADAM33 paved the way for recognition of non-atopic mechanisms involving proliferation of fibroblasts and smooth muscles and deposition of matrix proteins causing sub-epithelial fibrosis, leading to airway remodelling, an important mechanism for maintaining disease chronicity and progression (Figure). Airway remodelling is postulated to be due to aberrant communication between airway epithelium and mesenchymal tissue with ADAM33 playing an important role22.
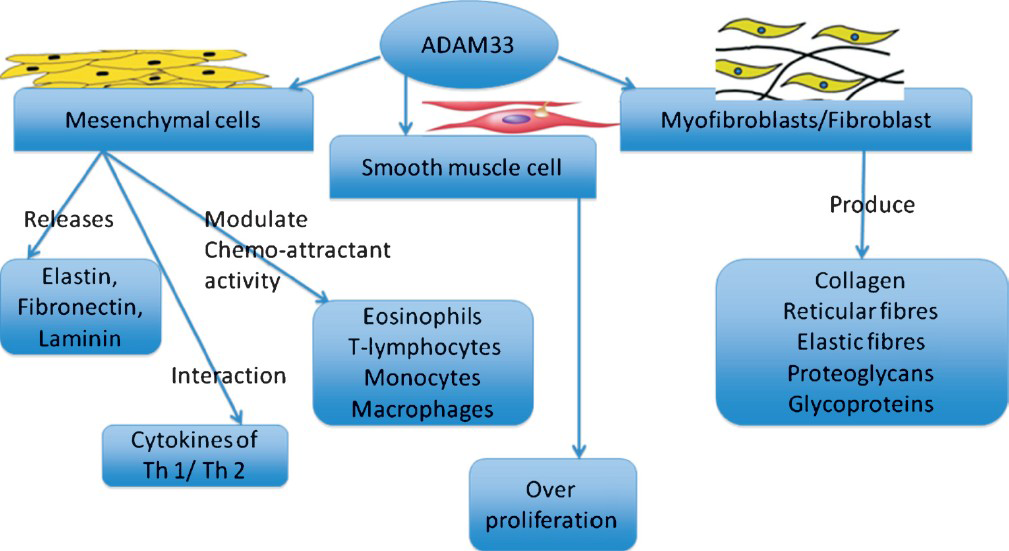
- Key cells influenced by ADAM33 in airway remodelling in asthma.
Though ADAM33 is associated with airway remodelling via non-inflammatory mechanisms, it can also promote inflammation via altered ADAM33 protein function leading to impaired or enhanced release of cytokines and growth factors22. Interactions between ADAM33 proteins and environmental factors could be important in the pathogenesis of asthma22. It has been demonstrated that the loss of membrane anchor and regulatory cytoplasmic domain of ADAM33, leads to a soluble form of ADAM33 (sADAM33), that can result in a disease-related gain of function wherein the abnormal localization of the ADAM33 metalloproteases results in inappropriate cleavage of angiogenic substrates to cause increased angiogenesis in the airway wall, contributing to airway wall thickening, one of the key findings in airway remodelling in asthma23. This leads to fixed airway obstruction and accelerated lung function decline in patients with asthma23.
There is a change in the perception that airway remodelling from being due to long-term uncontrolled chronic inflammation, seen only in adults, to being programmed in utero in the foetus and in young children even before they develop symptoms of asthma2224. ADAM33 is ubiquitously expressed in the foetal tissue and is one of the prime candidates for these changes in the foetal lungs22. In the normal foetus, ADAM33 is likely to be responsible for epithelial mesenchymal cross talk, branching of the airways and differentiation of the cells in the lungs25. Multiple single nucleotide polymorphisms in ADAM33 have been identified as being associated with asthma and it has been observed that combinations of SNPs confer a higher risk of asthma than single polymorphisms722. Subjects with both moderate and severe asthma have shown an increased expression of ADAM33 mRNA in endobronchial biopsy specimens as compared to normal subjects and subjects with mild asthma1.
Though ADAM33 located on chromosome 20p13 was identified to be important in asthma pathogenesis a decade ago, there is a need for concerted effort to elucidate its full implications, including its role in normal physiology, which is still unclear. The key reason for this is the complexity of the gene itself with multiple SNPs having been associated with asthma. Unravelling the ADAM33 would necessitate completely mapping all the SNPs in that gene region in all ethnic populations of the world, understanding the role of each SNP in health and disease, effect of these SNPs on gene transcription and resultant changes in the protein structure, protein levels and conformational changes in the tertiary protein structure that could potentially affect its functioning, thus leading to disease. It is also observed that alternative splicing could lead to different proteins with loss of or altered functions22. Studies have demonstrated that the downstream effects of the SNPs are complex and may not be related to simple gain or loss of function of ADAM33 proteins131326 since the amount of protein seems to be similar in bronchial biopsies of both asthmatic subjects and normal controls3. In addition, the role of other ADAMs such as ADAM8 which has been identified to be important in asthma1 and its interactions with ADAM33 need to be evaluated. Finally, all the potential interactions between other related pathways in asthma and ADAM33 may need to be studied in a systematic manner using a systems biology approach which will explain differential responses in different individuals and populations.
In this issue, Tripathi et al27 have demonstrated the presence of ADAM33 protein not only in the airway smooth muscle and mesenchymal cells but also in the airway epithelium, which is an important finding. Earlier studies has demonstrated that ADAM33 is expressed in fibroblasts and smooth muscle cells but not in airway epithelium722 and only a few studies have demonstrated that ADAM33 is expressed in the airway epithelium1. Higher expression of both isoforms of ADAM 33 proteins have been demonstrated in the airway smooth muscle, but not in airway epithelium22. Though the study by Tripathi et al27 has multiple limitations, it is a step in the right direction for unravelling the complex role of ADAM33 in asthma. The key limitations include, small sample size, paucity of controls, selection bias in including both cases and controls for the study as both cases and controls had additional co-morbidities other than asthma which could have confounded the results and the majority of the subjects were smokers. No significant difference was observed between moderate and persistent asthma, which could be due to low sample size. They observed a higher expression of ADAM33 protein in the asthmatic airway epithelium and smooth muscle cells as compared to controls. The role of ADAM33 in the airway epithelium and its role in the pathogenesis of asthma need to be further elucidated. With impaired epithelial barrier function identified as one of the key factors in the initiation of asthma20, the presence of ADAM33 in the airway epithelium warrants further research into its role in epithelial barrier function in health and disease. Further, study in ADAM33 proteins should expand into identifying the isoforms and splice variants and functional assays of these proteins need to be performed. In this era of biomarker discovery, whether total or different isoforms of ADAM33 protein levels could be an important biomarker to determine susceptibility for asthma in children and adults, accelerated decline in lung functions, airway remodelling and poor steroid responsiveness make an exciting field for future research.
Acknowledgment
The author thanks Ms. Sangeetha V. for help in preparing the Figure.
References
- Increased expression of ADAM33 and ADAM8 with disease progression in asthma. J Allergy Clin Immunol. 2007;119:863-71.
- [Google Scholar]
- Prevalence and risk factors for bronchial asthma in Indian adults: a multicentre study. Indian J Chest Dis Allied Sci. 2006;48:13-22.
- [Google Scholar]
- ADAM33 expression in asthmatic airways and human embryonic lungs. Am J Respir Crit Care Med. 2005;171:958-65.
- [Google Scholar]
- The genetics of asthma and allergic disease: a 21st century perspective. Immunol Rev. 2011;242:10-30.
- [Google Scholar]
- Discovering susceptibility genes for asthma and allergy. Nat Rev Immunol. 2008;8:169-82.
- [Google Scholar]
- An understanding of the genetic basis of asthma. Indian J Med Res. 2011;134:149-61.
- [Google Scholar]
- Association of the ADAM33 gene with asthma and bronchial hyperresponsiveness. Nature. 2002;418:426-30.
- [Google Scholar]
- Association of ADAM33 gene polymorphisms with asthma in Indian children. J Hum Genet. 2011;56:188-95.
- [Google Scholar]
- Association between ADAM33 polymorphisms and adult asthma in the Japanese population. Clin Exp Allergy. 2006;36:884-91.
- [Google Scholar]
- Association of IL-4 and ADAM33 gene polymorphisms with asthma in an Indian population. Lung. 2010;188:415-22.
- [Google Scholar]
- Contribution of ADAM33 polymorphisms to the population risk of asthma. Thorax. 2005;60:274-6.
- [Google Scholar]
- Association of a disintegrin and metalloprotease 33 (ADAM33) gene with asthma in ethnically diverse populations. J Allergy Clin Immunol. 2003;112:717-22.
- [Google Scholar]
- ADAM33: a newly identified protease involved in airway remodelling. Pulm Pharmacol Ther. 2006;19:3-11.
- [Google Scholar]
- ADAM 33: just another asthma gene or a breakthrough in understanding the origins of bronchial hyperresponsiveness? Thorax. 2003;58:466-9.
- [Google Scholar]
- ADAM33 polymorphism: association with bronchial hyper-responsiveness in Korean asthmatics. Clin Exp Allergy. 2004;34:860-5.
- [Google Scholar]
- Positionally cloned asthma susceptibility gene polymorphisms and disease risk in the British 1958 Birth Cohort. Thorax. 2009;64:381-7.
- [Google Scholar]
- Polymorphisms of the ADAM33 gene are associated with accelerated lung function decline in asthma. Clin Exp Allergy. 2004;34:757-60.
- [Google Scholar]
- ADAM33 haplotypes are associated with asthma in a large Australian population. Eur J Hum Genet. 2006;14:1027-36.
- [Google Scholar]
- A disintegrin and metalloproteinase 33 protein in patients with asthma: Relevance to airflow limitation. Am J Respir Crit Care Med. 2006;173:729-35.
- [Google Scholar]
- Polymorphisms in a disintegrin and metalloprotease 33 (ADAM33) predict impaired early-life lung function. Am J Respir Crit Care Med. 2005;172:55-60.
- [Google Scholar]
- The role of ADAM33 in the pathogenesis of asthma. Springer Semin Immunopathol. 2004;25:361-75.
- [Google Scholar]
- The soluble form of a disintegrin and metalloprotease 33 promotes angiogenesis: implications for airway remodeling in asthma. J Allergy Clin Immunol. 2008;121:1400-6.
- [Google Scholar]
- Early thickening of the reticular basement membrane in children with difficult asthma. Am J Respir Crit Care Med. 2003;167:78-82.
- [Google Scholar]
- Factors controlling smooth muscle proliferation and airway remodelling. Curr Opin Allergy Clin Immunol. 2002;2:47-51.
- [Google Scholar]
- Increased expression of ADAM 33 protein in asthmatic patients as compared to non-asthmatic controls. Indian J Med Res. 2013;137:507-14.
- [Google Scholar]




