
Translate this page into:
Polyarticular tuberculosis: A rheumatoid arthritis mimic
*For correspondence: adarshmb@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 35 yr old male† construction labourer presented to the Clinical Immunology department, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry, India, in June 2018, with a history of additive deforming polyarthritis involving bilateral ankle and wrist joints (Figure A and B) with prominent tenosynovitis for four months. X-ray of the hand showed carpal crowding, erosions of carpal bones and base of the second to fifth metacarpals. Differentials of rheumatoid arthritis, crystal-associated arthritis, amyloidosis, sarcoidosis, leprosy, septic arthritis, tuberculosis and paraneoplastic arthritis were considered. Rheumatoid factor and anti-citrullinated peptide/protein antibody were negative. Synovial fluid was milky, thick and opaque in appearance and negative for crystals. Synovial fluid culture for bacteria, tuberculosis and fungi was negative. Serum angiotensin-converting enzyme level was normal, and slit-skin smear was negative for acid-fast bacilli. Limited malignancy screening did not reveal any pathology. Magnetic resonance imaging of the right wrist showed distal radius and ulna erosions (Figure C and D). Biopsy from right wrist synovial tissue and adjacent bone showed confluent granulomas with caseous necrosis with evidence of bony erosion (Figure E). Culture from synovial biopsy tissue was positive for Mycobacterium tuberculosis. The patient was started on anti-tubercular therapy with which his arthritis improved over three months and was doing well on follow up. In such cases tuberculosis can mimic rheumatoid arthritis and synovial biopsy may help when there is an uncertainty in diagnosis.
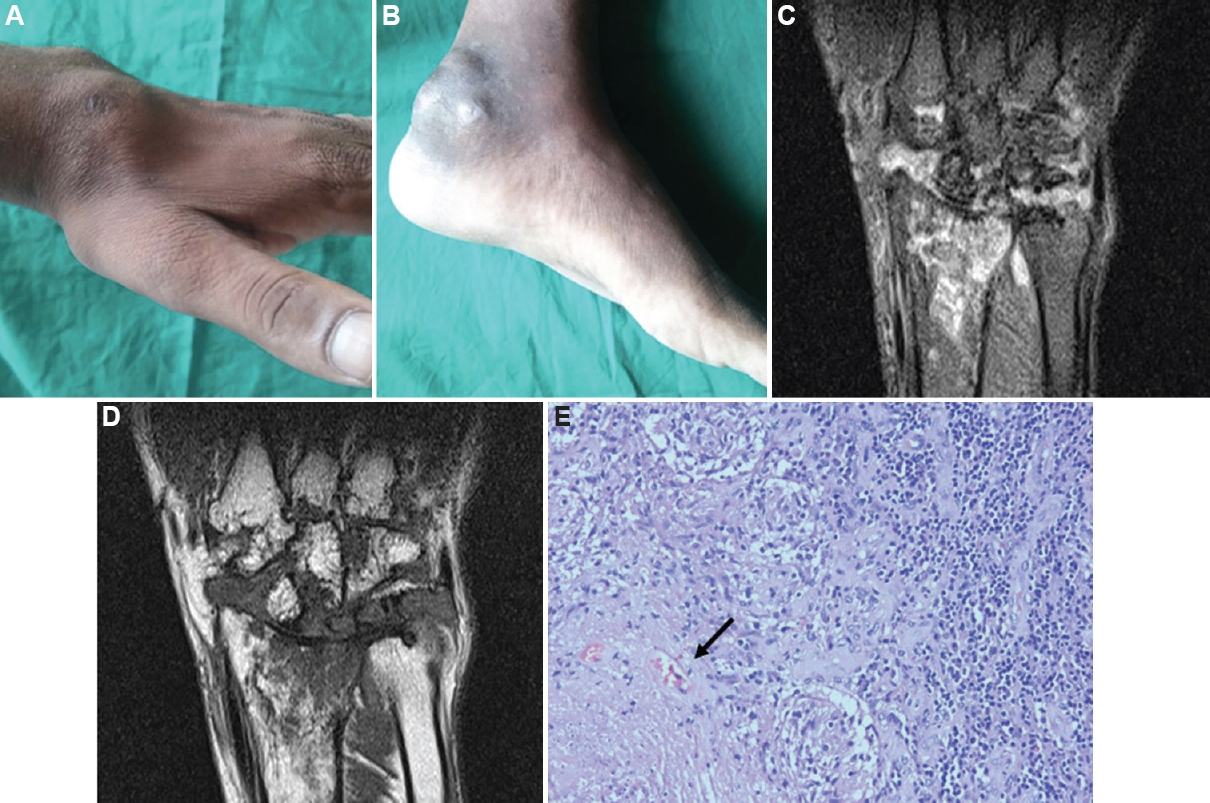
- (A and B). Soft-tissue swelling at wrist joint and ankle joint, respectively. (C) Magnetic resonance imaging proton density image of right wrist shows bone marrow oedema and periarticular soft-tissue involvement. (D) Magnetic resonance imaging wrist T1-weighted image shows erosions at distal ulna, radius and carpal bones. (E) Biopsy of the synovium (HPE staining, ×400) showing granuloma with caseous necrosis (black arrow).
Conflicts of Interest: None.




