
Translate this page into:
Viral aetiology of wheezing in children under five
Reprint requests: Dr Bhagirathi Dwibedi, Regional Medical Research Centre (ICMR), Chandrasekharpur, Bhubaneswar 751 023, Odisha, India e-mail: bhagirathidwibedi@yahoo.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Wheezing is a common problem in children under five with acute respiratory infections (ARIs). Viruses are known to be responsible for a considerable proportion of ARIs in children. This study was undertaken to know the viral aetiology of wheezing among the children less than five years of age, admitted to a tertiary care hospital in eastern India.
Methods:
Seventy five children, under the age of five years admitted with wheezing, were included in the study. Throat and nasal swabs were collected, and real-time multiplex polymerase chain reaction (PCR) assay was used to screen for influenza 1 and 2, respiratory syncytial virus (RSV), parainfluenza virus (PIV) 1, 2, 3 and 4, rhinovirus, human meta-pneumovirus, bocavirus (HBoV), Coronavirus, adenovirus, Enterovirus and Parechovirus.
Results:
The total viral detection rate was 28.57 per cent. Viral RNA markers were detected from children diagnosed to be having pneumonia (3 cases), bronchiolitis (9 cases), episodic wheeze (2 cases) and multitrigger wheeze (6 cases). RSV was the most common virus (35%) followed by PIV1, 2 and 3 (20%), HBoV (10%) and rhinovirus (5%). However, mixed infection was observed in 30 per cent of cases.
Interpretation & conclusions:
The study reported the presence of respiratory viral agents in 28.57 per cent of children with wheezing; RSV and PIV were most common, accounting to 55 per cent of the total cases. Mixed infection was reported in 30 per cent of cases. Seasonal variation in the occurrence of these viruses was also noted. Further studies need to be done with a large sample and longer follow up period to verify these findings.
Keywords
Asthma
bronchiolitis
child
incidence
India
multiplex polymerase chain reaction

Acute respiratory infection (ARI) with wheezing is a common problem in children under five years of age. It can sometimes be severe enough to warrant admission to paediatric intensive care unit (PICU) and require mechanical ventilation. According to the WHO, ARIs account for 16 per cent of deaths in children under five years of age worldwide1. It appears very difficult to enumerate the exact aetiology of the cases of wheezing among paediatric age group, especially 0-5 yr. As further investigations such as viral isolation are costly and require specialized infrastructure and not done routinely2 and also pulmonary function testing is not possible in this age group, most cases of wheezing either get empirically treated as bronchiolitis in the young infants or as asthma in an older child.
Wheezing is a prolonged, high-pitched, musical respiratory sound of varying intensity, heard more commonly in the expiration that occurs when smaller intrathoracic airways are narrowed by presence of bronchospasm, swelling of mucosal lining, excessive secretions, or inhaled foreign body3. Wheezing is a common clinical presentation with which infants and children present to the hospital and 30 per cent of children report at least one episode of wheezing by their third year of life4.
Viruses are responsible for a considerable proportion of ARIs in childhood5 and cause considerable mortality. The most important viruses involved in ARI are respiratory syncytial virus (RSV), influenza viruses A and B, parainfluenza (PIV), adenovirus (AdV), human rhinovirus and human meta-pneumovirus (hMPV)6. Though some of these viruses cause significant morbidity requiring hospitalization and lead to repeated attacks of wheezing and asthma in later years, there is very little information available on them, particularly from India. This study was conducted to look at the viral aetiological causes of wheezing in children under five admitted in a tertiary care hospital in eastern India.
Material & Methods
This study was conducted from August 2013 to August 2014. Patient enrolment was done by the department of Paediatrics at Hitech Medical College and Hospital, and laboratory investigations were carried out at virology Grade I laboratory of Regional Medical Research Centre, Bhubaneswar. Children below the age of five years, admitted to the paediatric ward and the PICU with diagnosis of lower respiratory tract infection (LRTI) and having wheezing (either auscultatory or audible), were selected consecutively as the study patients for virological investigations. Exclusion criteria were children above the age of five years, those presenting with or developing status asthmaticus and children whose parents did not provide consent for inclusion in the study. Every patient admitted to the paediatric ward or PICU with wheezing during the study period after screening for exclusion criteria was included in the study, and throat and nasopharyngeal swabs were taken for viral investigation.
The study was performed as per the predesigned proforma. Written informed consent was obtained from the parents/guardian of the child. The permission to conduct this study was obtained from the Institutional Ethics Committees of both, Hitech Medical College and Hospital and Regional Medical Research Centre, Bhubaneswar. The history and clinical findings were recorded in detail. Routine investigations were carried out, and special investigations were performed wherever necessary. The aetiological causes were divided based on the recommendation by the European Respiratory task force into allergic (multitrigger wheeze-which was defined as wheezing, both during discrete exacerbations and between episodes, triggered by both viral and non-viral agents such as allergens, exercise and cigarette smoke) and infective causes i.e., bronchiolitis (which was defined as the first episode of wheezing in a child <24 months of age, who has physical findings of a viral lower respiratory infection and no other explanation for wheezing), pneumonia (clinically defined as tachypnoea with fever) and episodic wheeze or viral wheeze (which was defined as wheezing occurring during discrete time periods with symptom-free period between episodes, usually associated with viral respiratory tract infection)78.
The nasopharyngeal and throat swabs collected from 70 children (5 children were excluded from the study based on the exclusion criteria) were sent for viral diagnosis by multiplex real-time PCR assay (ABI 7500, USA) using a commercially available kit (Fast Track Diagnostic, Luxembourg). Samples were collected within 24 h of admission and sent to the laboratory immediately in viral transport medium in ice packs. The swabs were screened for influenza A/B, RSV, PIV 1, 2, 3 and 4, rhinovirus, hMPV, bocavirus (HBoV), Coronavirus, AdV, Enterovirus and Paricovirus by multiplex PCR assay.
Results
A total of 188 children were admitted with respiratory complaints (LRTI) during the study period, of which 75 children had wheezing (either audible or auscultatory). This included episodic wheeze (13), multitrigger wheeze (19), bronchiolitis (24), bronchopneumonia (7), pneumonia (6), whooping cough (1), congenital heart disease with cardiac failure (3) and foreign body aspiration (2). Of these 75 children, five were excluded from the study based on the exclusion criteria, and samples of 70 children were sent for viral RNA markers. The viral aetiology could be observed in 28.57 per cent (n=20) of cases. Viral genome could be detected in three cases of pneumonia, nine cases of bronchiolitis, two cases of episodic wheeze and six cases of multitrigger wheeze. Details of viral RNA markers are given in the (Table). In this study, wheezing was observed in 40 per cent of children with respiratory infection, with a mean age of 14.11±12.74 months. Of the 75 children, 56 (75%) were male. Cough was the main presenting complaint (93%, n=70), followed by nasal discharge and respiratory distress (74%, n=55) and fever (64%, n=48). Additional symptoms such as watering of the eyes and skin rashes were seen in seven (n=5) and five (n=4) per cent cases, respectively. While all the children had auscultatory rhonchi, 36 per cent of them had audible wheeze. Tachypnoea and crepitation were seen in 71 per cent of children, retractions in 60 per cent, nasal flaring in 59 per cent and grunting was seen in four per cent children.
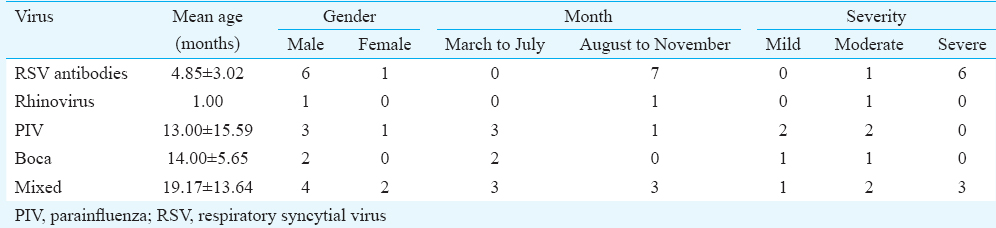
Seasonal variation was observed in the presentation of different viral cases in different age groups. It was observed that more children were brought to the hospital with respiratory symptoms during monsoon and autumn, with a peak incidence in the months of October (24%) and August (23%). The RSV (7 cases) and rhinovirus (1 case) were more in the months of August-November (autumn and winter), while parainfluenza (3 of the 4 cases) was more in March-July (summer). RSV (7 cases) and rhinoviruses (1 case) were isolated more in younger children (<1 yr) and parainfluenza (4 cases) and boca (2 cases) in older children (>1 yr). RSV was the most common virus observed, with a total of seven cases (35%) followed by PIV in four children (20%), HBoV was identified in two children (10%) and mixed infection was reported in 30 per cent of the cases. Viral isolates were positive in cases of infective origin (pneumonia in 3 cases, bronchiolitis in 9 cases and episodic wheeze in 2 cases) and allergic origin (multitrigger wheeze in 6 cases).
Discussion
The mean age of presentation of wheezing in this study was 14.11±12.74 months, and 78 per cent of children were less than two years old, which was more than that observed in earlier studies910. This study reported higher (75%) proportion of males admitted with wheezing, similar to many other studies1011121314.
The viral isolation rate was 28.57 per cent which was comparable to the study by Chanock et al15 on respiratory infection in 10 countries, showing viral isolation rate between 27 and 52 per cent. RSV was the single most common virus isolated and accounted for 30-70 per cent of cases in Indian studies161718. Other studies reported rhinovirus to be the most common followed by RSV619. Horn et al19 isolated rhinovirus in almost half of the cases with wheezy bronchitis, while PIV was isolated only from upper respiratory tract infections, para 1 and 2 in croup and para 3 in severe LRTI20.
We observed mixed infection in 30 per cent of the cases which was similar to other studies132122. HBoV was observed in 20 per cent of patients with mixed infection in our study, however, others have shown high rates of co-infection (50-60%) with HBoV1618.
In the present study, RSV infection was observed in younger age groups similar to Costa et al6 where children less than three months of age were most affected. PIV infection was recorded more in older children similar to a multinational study by Chanock et al15.
Mansbach et al23 have reported that though rhinovirus infection is milder and of shorter duration, it has more risk of recurrent wheezing and asthma in later years when compared to RSV infection. In the present study, rhinovirus infection was found to cause moderate severity of symptoms, and the study period was short to follow up for the development of asthma. The severity of presentation was more severe in RSV infections and mixed infections compared to PIV and HBoV infections. HBoV infection produced only mild symptoms in our study while HBoV was found to cause severe hypoxia requiring hospitalization in another study14. Though influenza virus was isolated and reported as a common viral pathogen causing severe disease in children under five years of age101724, and AdV and hMPV each accounted for 10 per cent of respiratory infections in this age group2425, we did not observe these viruses.
Seasonality was earlier reported as clustering of cases in specific seasons9151619202627. We observed RSV and rhinovirus more in August-November months (autumn-winter), while PIV and HBoV in March-July months (summer), but mixed infections occurred throughout the year.
Though this study provided information on respiratory viral agents in children under five years in the region, it was limited by small sample size and short follow up, that needs further investigation.
Acknowledgment
Authors thank ICMR for providing funding towards the virological tests under the VDRL project.
Conflicts of Interest: None.
References
- World Health Organisation; Causes of death in children under 5 years-2015; Child Mortality: Maternal, newborn, child and adolescent health. Available from: http://www.who.int/maternal_child_adolescent/topics/child/mortality/en/
- [Google Scholar]
- Viruses causing severe acute respiratory infections (SARI) in children ≤5 years of age at a tertiary care hospital in Rajasthan, India. Indian J Med Res. 2016;144:877-85.
- [Google Scholar]
- Wheezing in infants and toddlers: New insights. Wien Klin Wochenschr. 2004;116:15-20.
- [Google Scholar]
- Wheezy babies – Wheezy adults. Review on long-term outcome until adulthood after early childhood wheezing? ActaPaediatr. 2008;97:5-11.
- [Google Scholar]
- Estimates of world-wide distribution of child deaths from acute respiratory infections. Lancet Infect Dis. 2002;2:25-32.
- [Google Scholar]
- Respiratory viruses in children younger than five years old with acute respiratory disease from 2001 to 2004 in Uberlândia, MG, Brazil. Mem Inst Oswaldo Cruz. 2006;101:301-6.
- [Google Scholar]
- Definition, assessment and treatment of wheezing disorders in preschool children: An evidence-based approach. EurRespir J. 2008;32:1096-110.
- [Google Scholar]
- Recurrent wheezing in childhood. In: Thora S, Goswami VP, eds. Pediatrics for practitioner. New Delhi: Jaypee Medical Publishers; 2014.
- [Google Scholar]
- Wheezing – associated lower respiratory infections in under 5-year-old children: Study in Takhli District Hospital. J Med Assoc Thai. 2002;85(Suppl 4):S1247-51.
- [Google Scholar]
- Viral etiology of respiratory infections in children under 5 years old living in tropical rural areas of Senegal: The EVIRA project. J Med Virol. 2010;82:866-72.
- [Google Scholar]
- Impaired airway function and wheezing in infancy: The influence of maternal smoking and a genetic predisposition to asthma. Am J Respir Crit Care Med. 1999;159:403-10.
- [Google Scholar]
- Wheezing in infancy: Epidemiology, investigation, and treatment. J Pediatr (Rio J). 2010;86:171-8.
- [Google Scholar]
- High rate of viral identification and coinfections in infants with acute bronchiolitis. Clinics (Sao Paulo). 2010;65:1133-7.
- [Google Scholar]
- Human bocavirus in Iranian children with acute respiratory infections. J Med Virol. 2007;79:539-43.
- [Google Scholar]
- WHO respiratory disease survey in children: A serological study. Bull World Health Organ. 1967;37:363-9.
- [Google Scholar]
- Viral lower respiratory tract infection in infants and young children. BMJ. 2003;327:36-40.
- [Google Scholar]
- Clinical and epidemiological profiles of lower respiratory tract infection in hospitalized children due to human bocavirus in a subtropical area of China. J Med Virol. 2014;86:2154-62.
- [Google Scholar]
- Respiratory viral infection and wheezy bronchitis in childhood. Thorax. 1979;34:23-8.
- [Google Scholar]
- PCR for detection of respiratory viruses: Seasonal variations of virus infections. Expert Rev Anti Infect Ther. 2011;9:615-26.
- [Google Scholar]
- Pertinent issues in diagnosis and management of wheezing in under-five children at community level. Indian Pediatr. 2010;47:56-60.
- [Google Scholar]
- Respiratory syncytial virus in early life and risk of wheeze and allergy by age 13 years. Lancet. 1999;354:541-5.
- [Google Scholar]
- Prospective multicenter study of viral etiology and hospital length of stay in children with severe bronchiolitis. Arch Pediatr Adolesc Med. 2012;166:700-6.
- [Google Scholar]
- Spectrum of respiratory viruses circulating in Eastern India: Prospective surveillance among patients with influenza-like illness during 2010-2011. J Med Virol. 2013;85:1459-65.
- [Google Scholar]
- Pneumonia due to viral and atypical organisms and their sequelae. Br Med Bull. 2002;61:247-62.
- [Google Scholar]
- Respiratory viral infections detected by multiplex PCR among pediatric patients with lower respiratory tract infections seen at an urban hospital in Delhi from 2005 to 2007. Virol J. 2009;6:89.
- [Google Scholar]
- Seasonality of long term wheezing following respiratory syncytial virus lower respiratory tract infection. Thorax. 2004;59:512-6.
- [Google Scholar]




