
Translate this page into:
Comparison of Disease Activity Score in 28 joints with ESR (DAS28), Clinical Disease Activity Index (CDAI), Health Assessment Questionnaire Disability Index (HAQ-DI) & Routine Assessment of Patient Index Data with 3 measures (RAPID3) for assessing disease activity in patients with rheumatoid arthritis at initial presentation
Reprint requests: Dr B. Siddhartha Kumar, Department of Medicine, Sri Venkateswara Institute of Medical Sciences, Tirupati 517 507, Andhra Pradesh, India e-mail: bsk.svims@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
In patients with rheumatoid arthritis (RA), disease severity assessment is done using Disease Activity Score in 28 joints with ESR (DAS28). Computing DAS28 is time-consuming, requires laboratory testing and an online calculator. There is a need to validate rapid methods of disease severity assessment for routine daily use. This study was conducted to compare DAS28, Clinical Disease Activity Index (CDAI), Health Assessment Questionnaire Disability Index (HAQ-DI) and Routine Assessment of Patient Index Data with 3 measures (RAPID3) to assess the disease activity in patients with RA.
Methods:
We prospectively studied the utility of CDAI, HAQ-DI and RAPID3 scoring in 100 consecutive newly diagnosed, disease modifying antirheumatic drugs (DMARDs) naïve adult patients with RA seen during January 2013 and June 2014 at a tertiary care teaching hospital in south India.
Results:
The mean age of the patients was 42.1±11.6 yr, there were 82 females. The median [interquartile range (IQR)] symptom duration was 6 (range 4-12) months. The median (IQR) DAS28, CDAI, HAQ-DI and RAPID3 scores at presentation were 7 (6-7), 36 (28-43), 2 (1-2) and 17 (13-19), respectively. A significant positive correlation was observed between DAS28 and CDAI (r=0.568; P<0.001); DAS28 and HAQ-DI (r=0.304; P=0.002) and DAS28 and RAPID3 (r=0.404; P<0.001). A ‘slight-to-fair’ agreement was observed in between DAS28 and CDAI (kappa-statistic=0.296). The agreement between DAS28 and HAQ-DI (kappa-statistic=0.007) and RAPID3 (kappa-statistic=0.072) was less robust.
Interpretation & conclusions:
In adult patients with RA, in the setting where illiteracy is high, CDAI emerged as the preferred choice for rapid assessment of severity of disease at the time of initial presentation.
Keywords
Arthritis
CDAI
DAS28
disease severity assessment
rheumatoid arthritis

Rheumatoid arthritis (RA) is a common systemic autoimmune disorder affecting approximately 0.5 to 1 per cent of the population worldwide1. It has a female preponderance affecting women 3 to 4 times more commonly than men1. The disease is associated with progressive disability, systemic complications, socio-economic constraints and early death. Pathologically, RA is characterized by polyarticular synovial inflammation, antibody production [rheumatoid factor (RF) and anti-cyclic citrullinated protein/peptide (anti-CCP) antibodies] cartilage and bone destruction (deformity) and systemic features including cardiovascular, pulmonary and psychological disorders2. The aetiology of this condition is still elusive, and no single test defines RA. The American College of Rheumatology (ACR) criteria 20103 are designed to see that a patient with early arthritis is not denied the benefit associated with the early initiation of disease modifying anti-rheumatic drugs (DMARDs).
The progression of RA is highly variable. Sometimes RA can be very mild (with spontaneous remission), and thus remain undiagnosed, or it can be rapidly progressive and debilitating. However, the majority of patients present with an intermediate form of RA, in which episodes of exacerbation occurs4. Early initiation of aggressive treatment and frequent assessment and monitoring of RA activity allows timely adoption of appropriate therapies. This is important in preventing progression of the disease. Tight control of disease activity prevents radiographic disease progression and improves physical function and quality of life5. Disease Activity Score in 28 joints (DAS28) is being used as a measurement for assessing disease activity in patients with RA for the past several years6.
The DAS28 requires measurement of acute phase reactants, and a complex formula requiring a calculator, computer or access to an internet-based online calculator for computing it. Newer tools such as Clinical Disease Activity Index (CDAI)7, Indian version of Health Assessment Questionnaire Disability Index (HAQ-DI)8, Routine Assessment of Patient Index Data with 3 measures (RAPID3)9 are scoring systems that do not need any of the above tools for calculation. These can be easily employed in the evaluation of patients with RA, consistently at a greater frequency and without complex mathematical calculations.
There are scarce data regarding utility of DAS28, CDAI, HAQ-DI and RAPID3 in the assessment of disease activity in patients with RA from India. The present study was undertaken to compare DAS28, CDAI, HAQ-DI and RAPID3 to assess the disease activity in patients with RA at initial presentation.
Material & Methods
Consecutive patients newly diagnosed to have RA presenting to the Medicine Outpatient Department (OPD), Rheumatology Clinic and Medicine Wards at Sri Venkateswara Institute of Medical Sciences, a tertiary care teaching hospital in Tirupati, Andhra Pradesh, between February 2013 and July 2014 were studied. Adult patients (aged ≥18 yr), with newly diagnosed RA who had never received treatment with corticosteroids or DMARDs, were included in the study. Pregnant women, patients unwilling to participate in the study were excluded from the study. The study was approved by the Institutional Ethics Committee. After obtaining written informed consent, all the patients were subjected to a thorough clinical evaluation which included detailed history and physical examination. All the details were recorded in a structured proforma. RA was diagnosed as per the ACR/European League Against Rheumatism (ACR/EULAR) 2010 criteria3.
In all patients included, disease activity severity was assessed as described below. DAS286 was computed utilizing total join count (TJC), swollen joint count (SJC), visual analogue scale and erythrocyte sedimentation rate (ESR). CDAI7 was calculated using TJC, SJC, patient global assessment and provider global assessment. Indian version of HAQ-DI8 was administered to the patients and the responses were recorded. RAPID39 was also administered and the responses were recorded.
A patient with a DAS28 score of less than 2.6 is in remission; a score greater than or equal to 2.6 and less than 3.1 indicates low activity; a score greater than or equal to 3.1 and <5.1 indicates moderate activity and a score 5.1 or more indicates high activity6. A CDAI score of 0-2.8 indicates remission; 2.9-10 indicates low activity; 10.1-22 indicates moderate activity and 22.1-76 indicates high activity7. HAQ-DI scores of 0 to 1 represent mild-to-moderate difficulty, 1 to 2 moderate-to-severe disability and 2 to 3 severe-to-very severe disability8. A patient who scores a weighted RAPID3 score between 0 and 1.0 indicates near remission; a score 1.3-2.0 indicates low severity; a score 2.3-4.0 indicates moderate severity and a score of 4.3-10.0 as high severity9.
Elevated ESR was defined as 20 or more (in women), 15 or more (in men) participants aged under 50 yr and 30 or more (in women), 20 or more (in men) in participants aged 50 or more10. As per the Government of Andhra Pradesh criteria, persons with annual household income less than ₹ 75,000/- per annum in urban areas and less than ₹ 60,000/- per annum in rural areas who were ‘White Ration Card holders’ were categorized as ‘below poverty line’ (BPL) [G.O. Ms. No. 27, Dated: 23-07-2008, Department of Consumer Affairs, Food and Civil Supplies (C.S.I), Government of Andhra Pradesh, http://goirarchive.ap.gov.in/reports.aspx].
Statistical analysis: Descriptive statistics for the categorical variables were performed by computing the frequencies (percentages) in each category. For the quantitative variables, approximate normality of the distribution was assessed. Variables following normal distribution were summarized by mean and standard deviation; the remaining variables were summarized as median [interquartile range (IQR)]. The extent of agreement of CDAI, HAQ-DI and RAPID3 with DAS28 was tested using Kappa-statistic. Pearson's correlation coefficient was computed for DAS28 and CDAI, HAQ-DI and RAPID3. All tests were two-tailed; a P<0.05 was considered as significant. Statistical softwares IBM SPSS, Version 20, (IBM SPSS Statistics, Somers NY, USA); Stata/IC 12.0 for windows (Stata corp, Texas, USA); and MedCalc Version 11.3.0 for Windows 2000/XP/Vista/7 (MedCalc Software bvba, Belgium) were used for statistical analysis.
Results
During the study period, 228 consecutive patients with newly diagnosed RA were screened for inclusion in the study. Of these, 86 were excluded for the following reasons: use of corticosteroids (n=52), hydroxychloroquine (HCQs) (n=22), sulphasalazine (n=18), both corticosteroids and HCQs (n=9); 142 were further evaluated, and of these, 42 were excluded because of non-availability of ESR; the remaining 100 patients were included in the study. All these patients were treatment-naïve, had never received corticosteroids or DMARDs and were using only non-steroidal anti-inflammatory drugs for pain relief.
The mean age of the patients was 42.1±11.6 yr; majority of them (35%) belonged to the fourth decade of life. Female patients outnumbered males (male:female=1:4.5). The median IQR symptom duration was 6 (6-12) months. Of the 100 patients studied, 54 per cent belonged to BPL. Among women (n=82), 39 (47%) were homemaker; 37 (45%) were daily wage labourers; four were working women and two were students. Among men (n=18), 10 were daily wage labourers; six were government employees and two were self-employed.
Most commonly involved small joints were left wrist (90%) followed by the right wrist second and third metacarpal phalangeal joints in that order. Most common large joint involvement was observed to be knee (80%) followed by elbow and shoulder joint (78%). The details of tender and swollen joints observed in the study participants at the time of initial presentation are shown in Fig. 1. Ninety five of the 100 patients had elevated ESR. Symptom duration and summary statistics of some of the parameters used to calculate disease activity scores and indices are shown in Table I. The disease activity scores of DAS28, CDAI, HAQ-DI and RAPID3 are summarized in Table II. Disease severity at the time of initial presentation as assessed by different disease severity assessment scores6789 is shown in Fig. 2.
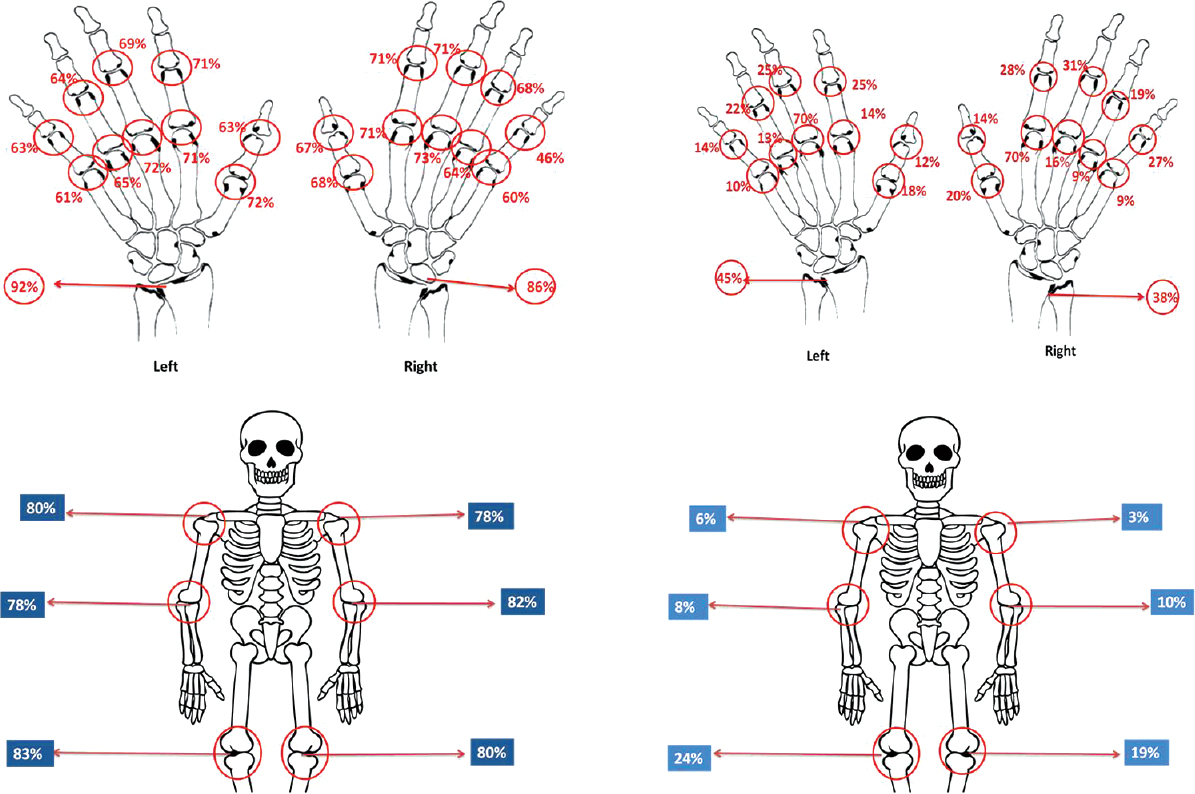
- Tender joint distribution among small joints (upper panel right); and swollen joint distribution among small joints (upper panel left). Tender joint distribution among large joints (lower panel right); and swollen joint distribution among large joints (lower panel left).


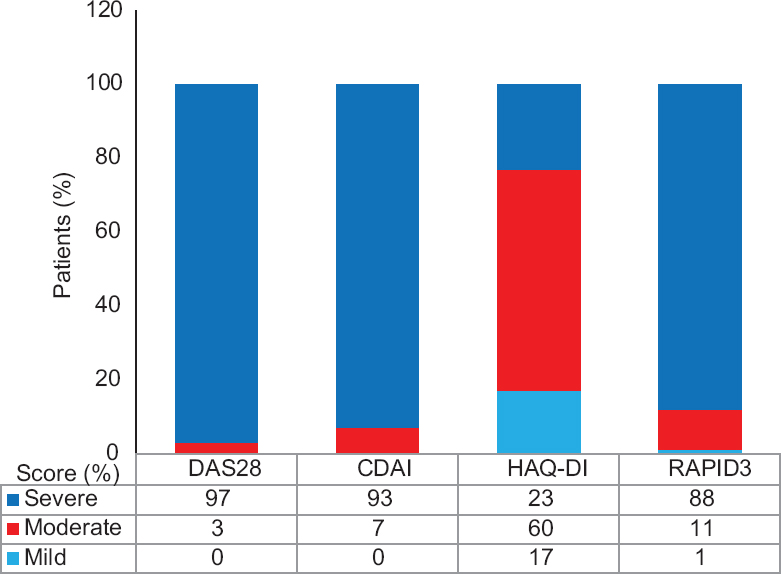
- Disease severity at the time of initial presentation in 100 treatment-naive patients with rheumatoid arthritis as assessed by different disease severity assessment scores. DAS28, Disease Activity Score in 28 joints with erythrocyte sedimentation rate; CDAI, Clinical Disease Activity Index; HAQ-DI, Health Assessment Questionnaire Disability Index, RAPID3, Routine Assessment of Patient Index Data with 3 measures.
A significant positive correlation was observed between DAS28 and CDAI (r=0.568; P<0.001); DAS28 and HAQ-DI (r=0.304; P=0.002) and DAS28 and RAPID3 (r=0.404; P<0.001) (Fig. 3). A slight-to-fair agreement was observed in the severity assessment between DAS28 and CDAI (kappa-statistic=0.296). The agreement between DAS28 and HAQ-DI (kappa-statistic=0.007) and RAPID3 (kappa-statistic=0.072) was less robust.
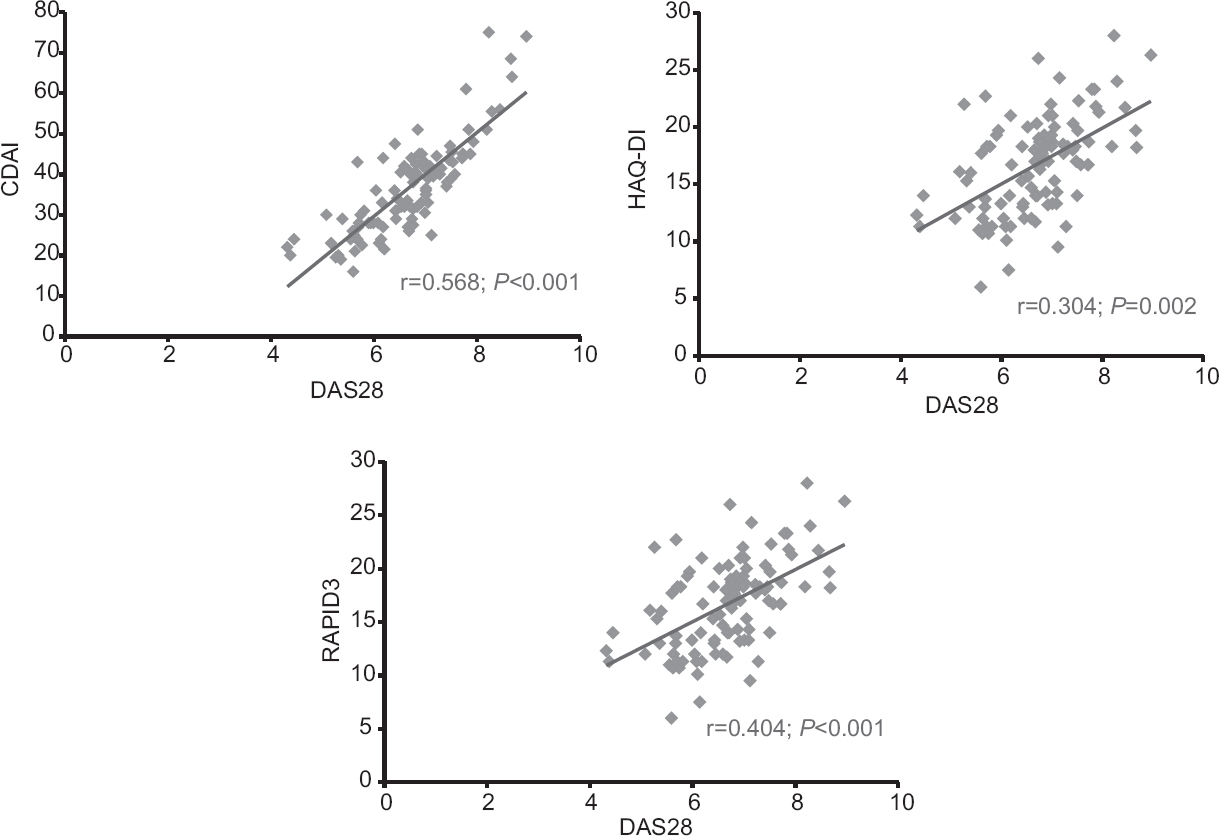
- Scatter plot showing correlation between CDAI, HAQ-DI and RAPID3 with DAS28.
Discussion
The disability suffered by patients with RA is the consequence of both disease-related factors (33%) and non-disease-related factors (26%) such as low socio-economic status and low educational standards4. Among the disease-related factors, poorer prognosis with joint destruction is associated with the presence of rheumatoid nodules, depression, persistent elevation of ESR, positive RF, positive anti-CCP antibody and presence of shared epitope on class II major histocompatability complex (MHC) genes. Apart from these factors, the intensity of disease activity has a major role in determining the prognosis of the patient. Thus, assessment of disease activity at an early stage in patient's disease and early initiation of DMARDs forms the cornerstone of treatment of RA. It has been shown that the disease activity has to be measured not only early in the disease but also repeated periodically so that any increase in activity is flattened out by an appropriate change in the DMARDs therapy and thus bone and cartilage damage prevented11. Majority of the patients with RA in the present study were in their fourth decade of life; women outnumbered men. These findings were similar to other published studies51213.
Assessment of disease activity and early initiation of DMARDs forms the cornerstone of treatment of RA. Although many methods have been described to assess the disease activity in patients with RA, DAS28 is still considered as the gold standard. The disadvantage with DAS28 is that it requires measurement of acute phase reactants, and a complex formula requiring a calculator or computer for calculation. Newer tools such as CDAI, HAQ-DI and RAPID3 are scoring systems that do not need any of the above. Further, HAQ-DI and RAPID3, which include a measure of function, are preferred as compared to DAS-28 or CDAI, which do not include a measure of physical function. These can be easily employed not only in the evaluation of patients with early RA but also can be consistently repeated at greater frequency, and thus study the course of the disease and response to treatment. As majority of our patients (54%) were poor and belonged to BPL, undergoing laboratory investigations periodically would have been expensive for them, and a simple clinically calculated disease severity assessment score was beneficial for such patients.
Most of the treatment naïve RA patients in the present study had severe disease activity at presentation. On comparing the results of the present study with another Indian study14 while we observed a significant correlation between DAS28 and all the indices (CDAI, RAPID3) measuring disease activity; a significant correlation was seen only with CDAI in the Kolkata study14. In the present study, a slight-to-fair agreement was observed in the severity assessment by DAS28 and CDAI. The agreement between DAS28 and HAQ-DI and RAPID3 were not very robust in our study, whereas in the other study14, all the three indices had good agreement. In the Kolkata study14, a significant agreement was observed between DAS28, CDAI and HAQ-DI. In a study15 from Austria that evaluated the agreement between the RAPID3 and a modified version of the rheumatoid Arthritis Disease Activity Index (RADAI5), DAS28-ESR and CDAI in routine daily practice, the reliability of questionnaires (RAPID3 and RADAI5) was significantly higher than that of the indexes. The authors had observed that the questionnaires (RAPID3 and RAPID5) as well as the indexes (DAS28-ESR, CDAI) proved to be in moderately high in agreement.
The major limitation of the present study was that it was a hospital-based study. Therefore, the observations from the present study might not reflect the scenario in the community. The sample size in the present study was small (n=100). Further, this study evaluated treatment naïve RA patients, at the time of initial presentation only. The ability of the disease activity severity scores in assessing the change in disease severity with DMARDs treatment was not evaluated due to logistic reasons.
Conflicts of Interest: None.
References
- Clinical features of rheumatoid arthritis. In: Firestein GS, Budd RC, Harris ED, McInnes IB, Ruddy S, Sergent JS, eds. Kelley's text book of rheumatology (8th ed). Philadelphia: Saunders Elsevier; 2009. p. :1087.
- [Google Scholar]
- Rheumatoid arthritis. Pathophysiology and implications for therapy. N Engl J Med. 1990;322:1277-89.
- [Google Scholar]
- 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62:2569-81.
- [Google Scholar]
- What are the consequences of early rheumatoid arthritis for the individual? Best Pract Res Clin Rheumatol. 2005;19:117-36.
- [Google Scholar]
- Prevalence of rheumatoid arthritis in the adult Indian population. Rheumatol Int. 1993;13:131-4.
- [Google Scholar]
- A simplified twenty-eight-joint quantitative articular index in rheumatoid arthritis. Arthritis Rheum. 1989;32:531-7.
- [Google Scholar]
- The Simplified Disease Activity Index (SDAI) and the Clinical Disease Activity Index (CDAI): A review of their usefulness and validity in rheumatoid arthritis. Clin Exp Rheumatol. 2005;23(5 Suppl 39):S100-8.
- [Google Scholar]
- Validation of an Indian version of the Health Assessment Questionnaire in patients with rheumatoid arthritis. Rheumatology (Oxford). 2002;41:1457-9.
- [Google Scholar]
- RAPID3-an index of physical function, pain, and global status as “vital signs” to improve care for people with chronic rheumatic diseases. Bull NYU Hosp Jt Dis. 2009;67:211-25.
- [Google Scholar]
- Etiology and pathogenesis of rheumatoid arthritis. In: Harris ED, Budd RC, Firestein GS, Genovese MC, Sergent JS, Ruddy S, eds. Kelley's text book of rheumatology Vol 2. (7th ed). Philadelphia: W.B. Saunders Company; 2005. p. :996-1042.
- [Google Scholar]
- Thyroid disease in systemic lupus erythematosus and rheumatoid arthritis. Rheumatology (Oxford). 2001;40:353-4.
- [Google Scholar]
- Rheumatoid arthritis is associated with a high prevalence of hypothyroidism that amplifies its cardiovascular risk. Ann Rheum Dis. 2008;67:229-32.
- [Google Scholar]
- Comparison between DAS28, CDAI and HAQ-DI as tools to monitor early rheumatoid arthritis patients in Eastern India. Indian J Rheumatol. 2011;6:116-22.
- [Google Scholar]
- A comparison of patient questionnaires and composite indexes in routine care of rheumatoid arthritis patients. Joint Bone Spine. 2009;76:658-64.
- [Google Scholar]




