
Translate this page into:
Clinical & radiological evaluation of atherosclerotic changes in carotid & coronary arteries in asymptomatic & clinically symptomatic individuals as a tool for pre-symptomatic diagnosis of cardiovascular disease
Reprint requests: Dr Venkatraman Bhat, 309, Greenwoods Apt, Royal Gardenia, Bommasandra, Bengaluru 560 099, Karnataka, India e-mail: bvenkatraman@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
An increase in prevalence of atherosclerosis has been noted worldwide with reports of higher incidence of atherosclerotic vascular changes in Asian Indians. There is a need to measure vascular atherosclerotic changes and provide objective parameter to predict cardiac and cerebrovascular adverse events. Atherosclerotic changes in carotids and coronaries are generally accepted as an association. We attempted in this study to relate intimal-luminal changes in carotid arteries to luminal changes in coronary arteries. Our study presents results of high resolution ultra sonographic (HRUS) evaluation of intimal-medial-thickness (IMT) in carotid with luminal changes in coronaries on multidetector-CT (MDCT) in clinically asymptomatic and symptomatic individuals.
Methods:
In this prospective study, HRUS examination of the carotid bifurcation was performed in 151 individuals to measure IMT in asymptomatic and symptomatic groups. Assessments of coronary arteries of the same group of patients were evaluated by MDCT within a week interval. IMT changes were associated with age, sex, predisposing factors, calcium burden of coronaries and structural atherosclerotic changes in coronary arteries.
Results:
A linear association of IMT was observed with increasing age. IMT of 0.5-0.69 mm was noted in 50 per cent of patients between 51-56 yr with higher number of symptomatic patients in this group. Linear increases in coronary vascular changes were noted with increasing IMT thickness. Changes were more prevalent in diabetic, hypertensive, treadmill test (TMT) positive and clinically symptomatic patients.
Interpretation & conclusions:
Age-related progression of atherosclerosis was evident in internal carotid arteries. Significant association was observed in the IMT thickness of right common carotid (RCC) and coronary disease in symptomatic group; whereas IMT of left common carotid and internal carotid arteries did not show any association. RCC IMT between 0.5-0.7mm showed maximal association with significant symptomatic narrowing of coronary arteries. Patients with IMT beyond 0.7mm had no association with symptoms.
Keywords
Atherosclerosis
carotid plaque
coronary CT angiography
HRUS
IMT
presymptomatic tool

High prevalence rates of premature coronary artery disease (CAD) have been reported in western literature in migrant Asian Indians1. In Chennai Urban Population Study, prevalence of CAD has been shown to be rising rapidly in urban India as substantiated with biochemical evidence in the study group2. Since Pignoli et al3 have demonstrated that ultrasound can be used to measure carotid intimal medial thickness (IMT) as an indicator of atherosclerosis, several studies have documented that increased carotid IMT correlates well with generalized changes of atherosclerosis, in particular coronary atherosclerosis456789101112. Monitoring vascular changes in major arterial tree has a critical role in predicting occurrence of adverse cardiovascular and cerebrovascular events789101112. Non-invasive, simple, robust and cost-effective technology like ultrasonography can make an immense impact in mass scale monitoring of vascular changes of atherosclerosis. The BioImage Study13 using imaging as an important parameter attempted to observe carotid plaque changes with relation to changes in rest of the major arteries. Quantitative estimation of plaque burden can be a surrogate marker for severity of atherosclerosis as well as practical tool for follow up of patients and monitoring response to therapy1415. Many recent studies have substantiated the direct correlation between carotid IMT and coronary atherosclerosis in general population and in patients with diabetes utilizing carotid sonography and coronary angiography1617. In a recent study, clinical selection criteria have been refined using SYNTAX score (synergy between percutaneous coronary intervention with TAXUS and cardiac surgery) and automated plaque measurement tools for better correlation18. We undertook this study to evaluate positive association of carotid intimal changes with coronary vascular changes in the Indian context using imaging based structural analysis and to explore feasibility of utilizing IMT as surrogate marker for evaluation of preclinical cardiovascular disease.
Material & Methods
This study was conducted at Narayana Multispecialty Hospital and Narayana Hrudayalaya of Narayana Health, Bengaluru, India, between August 2010 and December 2013. Individuals who attended the executive health check up programme and cardiology clinic for general check up (without specific cardiac symptoms) were included in asymptomatic group. Those with known cardiac, renal or any chronic systemic disease were excluded. Patients attending the cardiology clinic for cardiac ailments and those symptomatic patients who had positive clinical or treadmill test (TMT) results or prior multidector computed tomography (MDCT) or angiographic evidence of coronary artery disease were included in symptomatic group. Patients were selected consecutively for study enrollment. The study was approved by the institutional ethics committee.
All patients were examined for clinical vital signs, blood pressure recording, laboratory assessment of biochemical profile, specifically to exclude a familial hyperlipidaemia and diabetes. High resolution sonographic examination and MDCT examination were performed. Informed written consent was obtained from all asymptomatic and symptomatic individuals. Carotid artery scanning was performed with a high resolution scanner (iU22 Philips, Netherlands) with a linear phased array transducer of L12-5 MHz frequency. In principle, IMT was taken as the distance between the leading edge of the first echogenic line of the far wall of the carotid artery (lumen-intimal interface) and the leading edge of the second echogenic line (media-adventitia interface). End-diastolic measurements of IMT were utilized at three segments of common carotid artery just one cm before the bifurcation, the carotid bifurcation, and the proximal 1 cm of internal carotid artery (ICA). Measurements were taken only on longitudinal scans. For each individual, the maximum and average of all measurements at the six predefined sites were considered for further analysis. Q lab tool developed by Philips was utilized for automated IMT measurement. Additionally, volume of carotid artery centered on the bifurcation in transverse orientation was obtained by 3D probe (PhilipsVL13-5 MHz 3D volume probe). Imaging data including the distal common carotid and proximal internal carotid were stored for subsequent analysis of plaque volume. Similar volume acquisition of left carotid artery was performed.
Imaging of coronary arteries was done by plain and contrast angiography using MDCT- VCT 64 scanner (GE, Milwaukee USA). Study was done with ECG gating and with regular cardiac rhythm with heart rate, preferably between 55-65 beats/min (bpm). Heart rate was lowered in patients with heart rates exceeding 65 bpm by using ß-blocker metaprolol, 50 to 100 mg, 1 h prior to study, unless contraindicated. Nitroglycerin 0.4 mg was administered sublingually immediately prior to study. Patients were screened for renal function, only those with serum creatinine <1.5 unit were included for the procedure.
Preliminary low dose non-ionic contrast scan was performed for calcium scoring. Examinations were performed while patient holding breath in expiration, after bolus triggering the contrast injection at aortic root. Technical parameters included kV 120, effective mAs 700-900, detector collimation 0.6 mm, slice thickness 0.75 mm, rotation time 0.33 sec (0.37 sec for heart rate <50 bpm), reconstruction interval 0.6 mm, kernel B30f. Seventy to 100 ml iodixanol 350 mg/ml was injected intravenously with a saline chaser (40 ml for contrast opacification) with injection rate 5.5 ml/sec. ECG gated retrospective data reconstruction was performed.
Volumetric data of CT angiography (CTA) were used for retrospective reconstruction. Reference data for image reconstruction were obtained from specific parts of the cardiac cycle, typically at late diastole. Retrospective reconstruction datasets, typically 30, 55, and 70 per cent of the R-R interval were utilized for evaluation. However, in all patients, data throughout the cardiac cycle were examined, reconstructing at 10 per cent intervals. On post-processing optimal phase for coronary artery reconstruction was chosen. Source images were reviewed to confirm findings at advantage v4.4 (GE Milwaukee, USA) workstation for reconstructions.
Basic component in image analysis included estimation of luminal caliber in major coronary arteries, estimation of calcified and non-calcified plaques and coronary calcium burden in both coronary arteries. Structural changes in coronary arteries were analyzed for left main coronary, left anterior descending artery (LAD), circumflex artery and right coronary artery (RCA) (Figure). Coronary vascular changes were grouped into normal, insignificant disease (luminal narrowing <50%) and significant disease category (luminal reduction>50%).
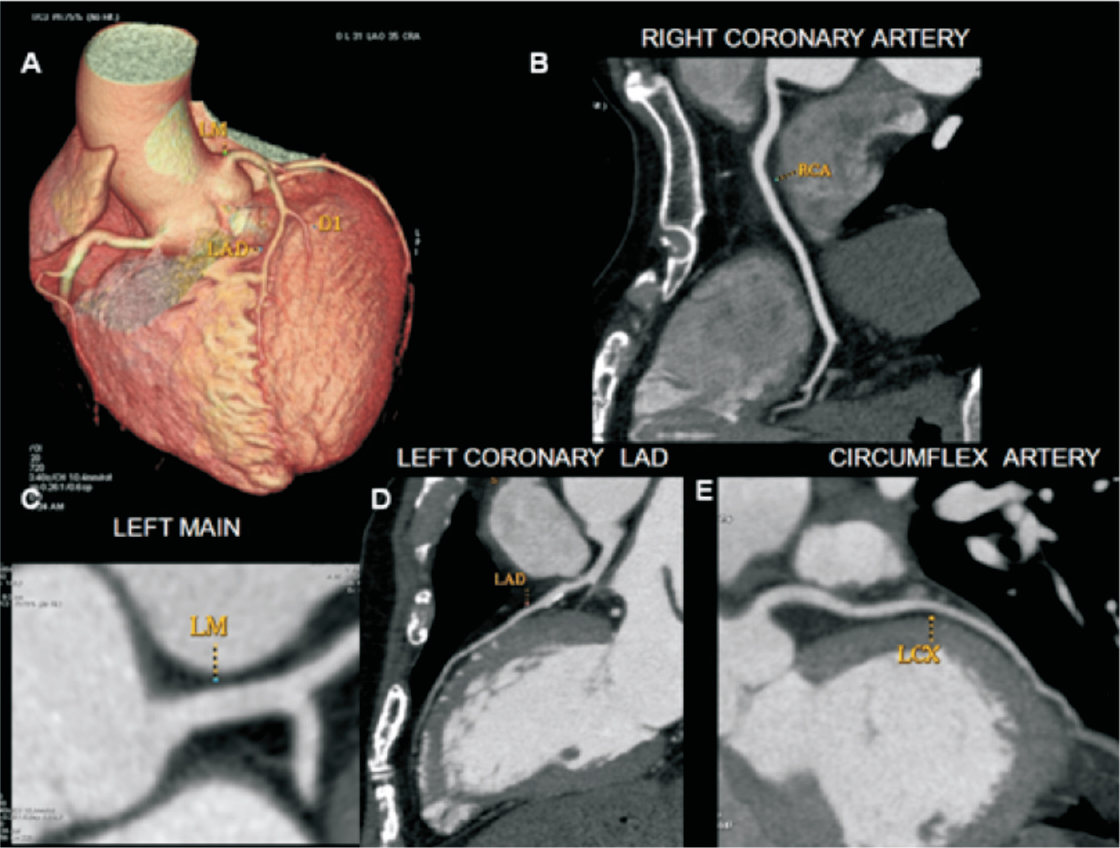
- Multidetector computed tomography (MDCT) reconstructed images (A) Surface rendered volumetric image, (B) Reconstructed image of right coronary artery, (C) Left main coronary artery (LM), (D) Left anterior descending artery (LAD), and (E) Circumflex branch of left coronary artery (LCX). Illustrated arteries are analyzed for calcification, luminal narrowing and occlusion.
Statistical analysis was performed by STATA11.1 (College station TX USA). Student's t test and/or Mann-Whitney U test were used to find the significant difference between the groups. Gender, pain, TMT results, diabetic state, hypertension and CT coronary parameters of proximal, distal RCA, proximal, mid, distal LCA, circumflex arteries and arterial dominance were compared between the groups. Chi square and Fisher exact test were performed, results expressed as frequency and percentage. Logistic regression analysis was performed for factors associated with the symptoms.
Results
Study groups consisted of 151 patients, in the age range of 19 and 73 yr, with a mean age of 50.3 yr (Table I); 87 (57.6%) patients were in asymptomatic group against 64 (42%) in symptomatic. IMT measurements were possible in 100 per cent of patients for evaluation for common carotid artery (CCA), in comparison to the internal carotid (93-96%), failed studies mostly on left side due to technical limitations. IMT thickness of right common carotid showed a range of 0.4 to 1 mm, with a mean value of 0.53. Left CCA showed IMT thickness of 0.4 -1.2 mm, with a mean value of 0.56. The mean IMT thickness of right internal carotid was 0.64 mm and left internal carotid was 0.65 mm. IMT thickness showed gradual increase with age. There was significant association with right common carotid (RCC) IMT thickness, [t (151)=-2.57, P=0.006] in symptomatic patients as against asymptomatic. Rest of the arteries did not show significant association. Decreasing association was noted from RIC, LIC and LCC respectively (Table I).
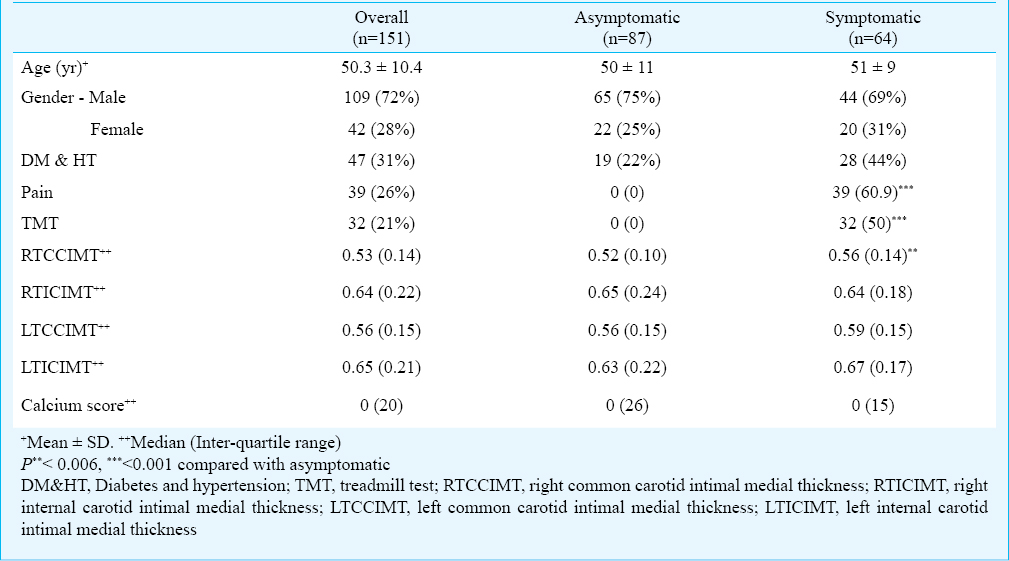
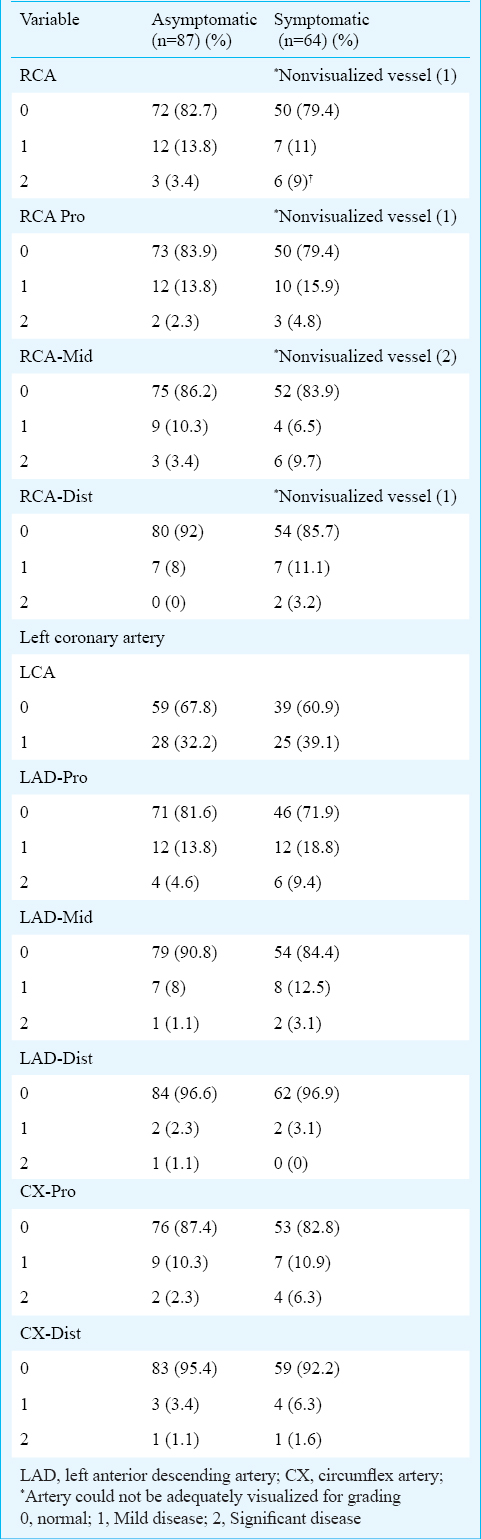
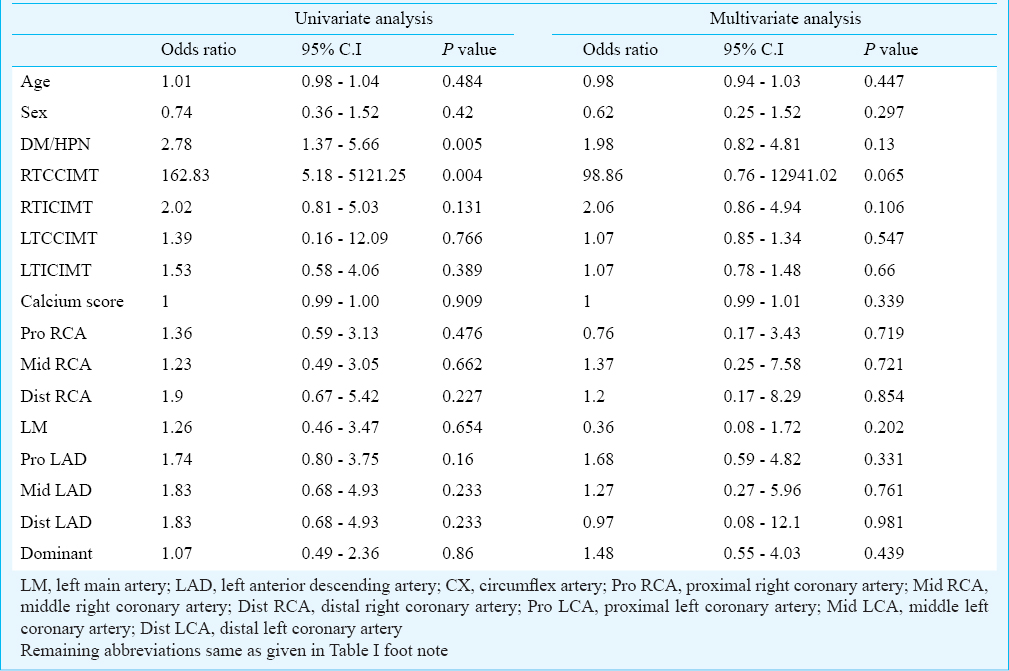
On MDCT evaluation of the asymptomatic group, right coronary artery (RCA) was normal in 72 (82.7%); LAD in 71 (81.6%). RCA showed significant disease in three (3.4) per cent, insignificant plaque changes in 12 (13.8%). RCA was not visualised in one patient and at middle third in another. Left coronary artery had disease in 28 (32.2%). LAD was normal in 71 (81.6%), showed insignificant disease in 12 (13.8%) and significant disease in four (4.6%). Circumflex artery (CX) showed normal anatomy in 76 (87.4%) with significant disease in two (2.3%) and asymptomatic disease in nine (10.3%). In the symptomatic group right coronary and LAD were normal in 50 (79.4%) and 46 (71.9%), respectively. RCA showed significant disease in six (9.5%), insignificant plaque changes in seven (11%). Left coronary artery had disease in 25 (39.1%). LAD was normal in 46 (71.9%), showed insignificant disease in 12 (18.8%) and significant disease in six (9.4%). Circumflex artery showed normal anatomy in 53 (82.8%) with a significant disease in four (6.3%) and asymptomatic disease in seven (19.9%). Incidence of luminal changes at different segments of the arteries are documented in Table II. Maximal vessel changes were noted in the proximal arteries. Coronary calcium score ranged between 0-1093, with a mean of 47 for asymptomatic group and 49.5 in the symptomatic. Forty seven (31%) patients had predisposing conditions like diabetes or hypertension. Majority of patients in the symptomatic group 39 (60.9%) had pain as the predominant symptom. Half of the symptomatic patients 32 (50%) had positive TMT examination. There was no significant difference in IMT in symptomatic vs. asymptomatic groups within the same sex. Within the symptomatic group male had higher IMT (72.2%) although gender difference was not significant. Patients with a significant disease (>50% narrowing) in LCA (6, 9.4%) (mostly in LAD) and RCA (6, 9.5%) had higher association with symptoms. Similar observations were noted for the involvement of middle and distal third of the arteries and their branches. Overall, extent of RCA disease compared to LCA showed poor association with symptoms. Also, dominance of the vessel did not show association with clinical symptoms. Univariate and multivariate analyses of data on risk factors indicated an association of IMT at both CCA, both ICA, diabetic state, significant disease at left main coronary and proximal LAD with symptomatic disease (Table III). Most significant association was noted with IMT of right CCA (P=0.004). Predisposing factors of diabetes and/or hypertension were seen in a significantly larger number in symptomatic patients compared to asymptomatics (43.8 vs. 21.8%). Pain was predominant presentation of symptomatic disease. Similar relation was noted in patients with positive TMT test which showed significant association with clinical disease (Table I).
Discussion
Many studies support the observation that IMT assessed by B-mode ultrasound in extracranial carotid arteries, either in a single segment (common carotid) or in multiple segments (aggregate of measures in common carotids, bifurcations, and internal carotids), is a valuable indication of coronary risk status and a predictor of subsequent coronary heart disease (CHD)34561617. CHD constitutes a leading source of cardiovascular death, morbidity and healthcare expenditure19. Most studies have evaluated carotid IMT thickness either with coronary angiography or multiple surrogate clinical parameters of CAD. There are scanty studies relating carotid IMT with observations on CT coronary angiography17. Coronary CT angiography is noninvasive and has potential for evaluation of additional parameters like calcium scoring, soft plaque assessment and vessel remodelling20. It has been shown in two pioneering prospective population based studies46 that markedly increased IMT above one mm is associated with a 12-16 per cent 10-year CHD incidence. Incidence varied slightly depending on age, sex, and carotid segment(s) measured, whereas the lowest percentiles of IMT distribution were associated with a CHD incidence of consistently 0.5 per cent46. Some other studies have further substantiated the role of carotid plaque burden assessment and IMT measurement as a measure of subclinical atherosclerosis151921. Thus, our observations also provided data in support of this association in the Indian context utilizing carotid IMT and MDCT coronary angiography.
We observed IMT of RCC to be most sensitive parameter for predicting coronary arthrosclerosis. This observation needs further substantiation in view of a wide confidence interval. The gradual age related increase in carotid IMT is known to be closely associated with silent, as well symptomatic progression of coronary atherosclerosis, as also observed in our study. In our study IMT of 0.6 mm and above was associated with a higher incidence of coronary intra-luminal disease and clinical symptoms. However, further increase beyond 0.7 mm in IMT was not associated with increase in symptomatic disease, probably suggesting stability of plaque with increasing thickness. IMT values noted in our study for symptomatic patients were lower than the ones observed in other studies456 indicating a role of multiple parameters. We have not studied plaque morphology, plaque evolution and vessel remodelling, factors which appear to have better relation in understanding plaque stability and causation of symptoms. Distribution of luminal disease was similar in right and left coronary arteries and branches. There was no significant difference in the intimal thickness between male and female patients. There was association with RCC IMT though the values did not stratify symptomatic vs. asymptomatic patients. Occurrence of atherosclerosis, as assessed by intralumial changes in carotid and coronary arteries, did not indicate either early onset or more severe manifestations in our study.
There were a few limitation in the study; firstly, the design of categorizing patients into asymptomatic and symptomatic groups was simplistic, hence indicated values and inferences should be validated with a larger study sample along with risk stratification. Second, there was a lack of defining objective criteria for estimating coronary risk based on clinical risk profile. Utilization of these parameters will enable more linear assessment of association. Thirdly, relatively small sample size of our study did not allow clear, valid conclusion to be inferred regarding grade of coronary disease in relation to carotid disease. Fourth limitation was regarding technical limitation of coronary angiography which lacks ability to precisely document coronary atherosclerosis. New technical advances in speed and precision of image acquisition are likely to improve the evaluation20. Our observations on association of atheromatous changes in carotid and the relation with coronary atherosclerosis were in line with the observations of other studies41722. In this ongoing study we intend to stratify clinical risk profile for better correlation, to optimize grading of coronary vascular changes, evaluate role of plaque volume as against IMT and analyze our observations in a large data-set and define a image based surrogate for monitoring atherosclerosis.
Acknowledgment
Authors acknowledge the contribution of all colleagues of Radiology department and Shri Jeyeram Illyaraja for statistical help. Special thanks to Dr Devi Shetty for providing institutional support. The authors thank Koninklijke Philips Electronics N.V. Netherlands, for initiating this research work and providing infrastructure support for image acquisition and analysis.
Conflicts of Interest: None.
References
- Malignant coronary artery disease in young Asian Indians: thoughts on pathogenesis, prevention, and therapy. Coronary Artery Disease in Asian Indians (CADI) Study. Clin Cardiol. 1995;18:131-5.
- [Google Scholar]
- Prevalence of coronary artery disease and its relationship to lipids in a selected population in South India: The Chennai Urban Population Study (CUPS No. 5) J Am Coll Cardiol. 2001;38:682-7.
- [Google Scholar]
- Intimal plus medial thickness of the arterial wall: a direct measurement with ultrasound imaging. Circulation. 1986;74:1399-406.
- [Google Scholar]
- Relationship between carotid intima-media thickness and coronary angiographic findings: a prospective study. Am J Cardiol. 2007;99:1196-200.
- [Google Scholar]
- Usefulness of carotid ultrasound to improve the ability of stress testing to predict coronary artery disease. Am J Cardiol. 2007;99:1196-200.
- [Google Scholar]
- The value of carotid artery plaque and intima-media thickness for incident: Cardiovascular disease: The multi-ethnic study of atherosclerosis. J Am Heart Assoc. 2013;2:e000087.
- [Google Scholar]
- Risk factors for coronary heart disease in African Americans: the Atherosclerotic Risk in Communities Study, 1987-1997. Arch Intern Med. 2002;162:2565-71.
- [Google Scholar]
- Coronary heart disease statistics. London: British Heart Foundation; 2007.
- World Health Organization (WHO) In: The global burden of disease: 2004 update. Geneva: WHO; 20085. p. :17-26. Part 2
- [Google Scholar]
- Comprehensive assessment of mortality and disability from disease, injuries and risk factors in 1990 and projected to 2020. The global burden of disease: A. Boston, USA: Harvard University Press; 1996.
- High-Risk Plaque Initiative. The BioImage Study: novel approaches to risk assessment in the primary prevention of atherosclerotic cardiovascular disease - study design and objectives. Am Heart J. 2010;160:49-57.
- [Google Scholar]
- 3D Ultrasound measurement of change in carotid plaque volume. A tool for rapid evaluation of new therapies. Stroke. 2005;36:1904-9.
- [Google Scholar]
- Measurement of carotid plaque volume by 3-dimensional ultrasound. Stroke. 2004;35:864-9.
- [Google Scholar]
- Relationship between carotid intima-media thickness and the presence and extent of coronary stenosis in type 2 diabetic patients with carotid atherosclerosis but without history of coronary artery disease. Diabetes Care. 2011;34:468-70.
- [Google Scholar]
- Association of carotid artery parameters of atherosclerosis in coronary artery disease. J Cardiovasc Ultrasound. 2013;21:72-80.
- [Google Scholar]
- Improved correlation between carotid and coronary atherosclerosis SYNTAX score using automated ultrasound carotid bulb plaque IMT measurement. Ultrasound Med Biol. 2015;41:1247-62.
- [Google Scholar]
- Intima-media thickness: a new tool for diagnosis and treatment of cardiovascular risk. J Hypertens. 2002;20:159-69.
- [Google Scholar]
- Carotid plaque burden as a measure of subclinical atherosclerosis: comparison with other tests for subclinical arterial disease in the High Risk Plaque BioImage Study. JACC Cardiovas Imaging. 2012;5:681-9.
- [Google Scholar]
- Carotid intima-media thickness and coronary artery disease: an Indian perspective. Asian Cardiovasc Thorac Ann. 2003;11:217-21.
- [Google Scholar]




