Translate this page into:
Clinical, biochemical & cytomorphologic study on Hashimoto's thyroiditis
Reprint requests: Dr Suja Sreedharan, Professor & Head, Department of Otorhinolaryngology Head & Neck Surgery, Kasturba Medical College, Manipal University, Mangalore 575 001, Karnataka, India e-mail: sujasreedharan@yahoo.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Despite, the extensive salt iodization programmes implemented in India, the prevalence of goiter has not reduced much in our country. The most frequent cause of hypothyroidism and goiter in iodine sufficient areas is Hashimoto's thyroiditis (HT). This study records the clinical presentation, biochemical status, ultrasonographic picture and cytological appearance of this disease in a coastal endemic zone for goiter.
Methods:
Case records of patients with cytological diagnosis of HT were studied in detail, with reference to their symptoms, presence of goiter, thyroid function status, antibody levels and ultrasound picture. Detailed cytological study was conducted in selected patients.
Results:
A total of 144 patients with cytological proven HT/lymphocytic thyroiditis were studied. Ninety per cent of the patients were females and most of them presented within five years of onset of symptoms. Sixty eight per cent patients had diffuse goiter, 69 per cent were clinically euthyroid and 46 per cent were biochemically mildly hypothyroid. Antibody levels were elevated in 92.3 per cent cases. In majority of patients the sonographic picture showed heterogeneous echotexture with increased vascularity. Cytological changes were characteristic.
Interpretation & conclusions:
Our study showed predominance of females in the study population in 21-40 yr age group with diffuse goiter. We suggest that in an endemic zone for goiter, all women of the child bearing age should be screened for HT.
Keywords
Antithyroid antibody
cytology
FNA
goiter
Hashimoto's thyroiditis
hypothyroidism
lymphocytic infiltration

Endemic goiter is a major health problem in India. Widespread national salt iodization programmes implemented by the Government of India have not shown a dramatic decline in the prevalence of endemic goiter1. The reason for the high prevalence of goiter is not fully understood. A genetic predisposition of the Indian population for development of autoimmune goiter has been suggested2. Secondly, iodine itself could induce autoimmunity in patients. Iodine induced thyroiditis is well established in animal studies3. It has also been seen that iodine supplementation in iodine deficient areas increases the prevalence of lymphocytic infiltration of thyroid by three-fold; with 40 per cent increase in prevalence of antithyroid antibodies in serum over 0.5 to 5 years4.
This study was carried out at a tertiary care hospital located in the western coastal area known for endemicity of goiter, where sea food is the staple diet of the population. Moreover, there is a widespread use of iodized salt in the population. In spite of this, increasing numbers of goiters diagnosed to have Hashimoto's thyroiditis (HT) have been observed. We undertook this study to understand the clinical presentation, biochemical status and ultrasonographic picture of HT in this area. We also did a cytological analysis on a few patients to analyse the typical cytomorphologic features of HT and associated the clinical features, biochemical thyroid status and cytological parameters with each other to understand the pathogenesis of the disease.
Material & Methods
This study was conducted in the department of Otorhinolaryngology, Head and Neck surgery, Kasturba Medical College, Mangalore, Karnataka, India, on 144 patients with HT. This was a cross-sectional study conducted on patients with cytologic diagnosis of Hashimoto's thyroiditis/lymphocytic thyroiditis (LT) during January 2001 to July 2011. Retrospective analysis of the medical records of patients was carried out from 2001 to 2009 and prospective study of patients was done from July 2009 to July 2011. Patients with cytology proven HT/LT with or without associated pathology were included in the study. Patients with cytology of multinodular or colloid goiter were excluded. The study protocol was approved by the ethics committee of the hospital. Informed written consent was obtained from patients of prospective study group.
Information on clinical presentation with emphasis on age, sex, presenting complaints, duration of complaint, clinical signs of hyperthyroidism or hypothyroidism, presence of goiter and tenderness was recorded. Investigations noted were thyroid function tests namely T3 (triiodothyronine) (normal values 0.6-2.02 IU/ml), T4 (thyroxine) (normal values 5.13-14.06 IU/ml), TSH (thyroid stimulating hormone) (normal values 0.27-5.5 IU/ml), FreeT4 (normal values 0.93-1.71 IU/ml). Antithyroid antibody levels namely anti thyroid peroxidase (anti TPO) (normal values <35 IU/ml) and antithyroglobulin (anti Tg) antibody levels (normal values <35 IU/ml) were documented. The thyroid function tests and antithyroid antibody levels were estimated in our hospital lab by ECLIA (Electro chemilumniscence immune assay) method. (Automated Roche Cobas e411 Analyser, Roche Diagnostics, USA).
Ultrasonographic reports were also evaluated. Volume of gland, echo texture, echogenicity and vascularity were recorded in all possible cases. Volume was calculated using the formula: length x width x thickness x 0.52 (correction factor) for each lobe. A volume of 18.6 ± 4.5 ml was considered to be normal5. Treatment modalities offered to patients were also evaluated. A detailed cytological study was done in selected 52 cases from fine needle aspiration (FNA) smears from the last two years (2009-2011). The main parameters studied were amount of lymphocytes, lymphocytic infiltration and destruction of follicular cells and Hurthle cell change.
Statistical analysis was done using SPSS 17.0 (Chicago: SPSS Inc). Chi-square test and ANOVA were used and P<0.05 was considered as significant. Biochemical values of thyroid function, ultrasound characteristics of HT, cytological parameters and antithyroid antibody levels were correlated with one another using the Karl Pearson's correlation coefficient.
Results
A total of 144 patients with cytology proven HT/LT were included in the study. Of these, 46 patients were included retrospectively, while the prospective group had 98 patients. These were 129 females and 15 males (Table I), which indicated a significantly higher percentage of females having HT as compared to males (P<0.001). The age of the patients ranged from 9 to 75 yr. Mean age was 34.18 ± 12.71 yr. Maximum number of cases were noted in the 3rd decade (20-30 yr age group, n=46) followed by the 4th decade (31-40 yr age group, n=40). Patients in the third decade were significantly more affected than those in other age groups (P<0.001).
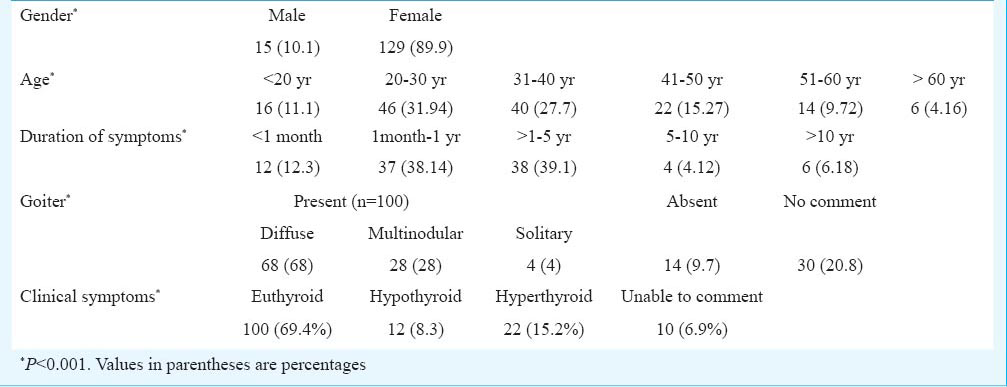
Ninety seven patients had documentation about the duration of their symptoms; 87 (89.6%) patients presented to hospital within 5 years of symptom manifestation (Table I). The difference was significant when compared with patients presenting at a later date (P<0.001).
Goiter was present in 100 cases, 14 cases were documented as absent goiter and no comment was documented in 30 cases. A significant number of patients had a goiter at presentation (P<0.001). Of these 100 cases, goiter was diffuse in 68 cases, multinodular in 28 cases and solitary nodule in four cases. Clinically majority (n=100) of patients had no features of hypothyroidism or hyperthyroidism, only 12 cases were identified to have hypothyroid features and 22 had hyperthyroid features (Table I). This showed that a significant number of patients were clinically euthyroid (P<0.001). Vague symptoms like generalized fatigue and malaise were reported by some patients. Pain/tenderness of thyroid gland was present in seven cases among the total 144 cases.
Based on TSH levels, there were 64 cases of hypothyroidism, 46 cases of euthyroidism and 30 of hyperthyroidism. Information was incomplete in rest of the cases (Table II). There was a significant difference in the thyroid function status of the patients (P<0.01). The hypothyroid patients were classified into mild, moderate and severe based on the TSH levels (mild 5.5 - 45.5, moderate 45.5 - 85.5, severe >85.5 IU/ml). Significant number of patients had mild hypothyroidism (P<0.01). T4 levels were normal in 32 cases (subclinical hypothyroidism) and low in 24 cases (overt hypothyroidism) (Table II). Volume, echo texture, echogenicity and vascularity of the gland were also recorded (Table II).
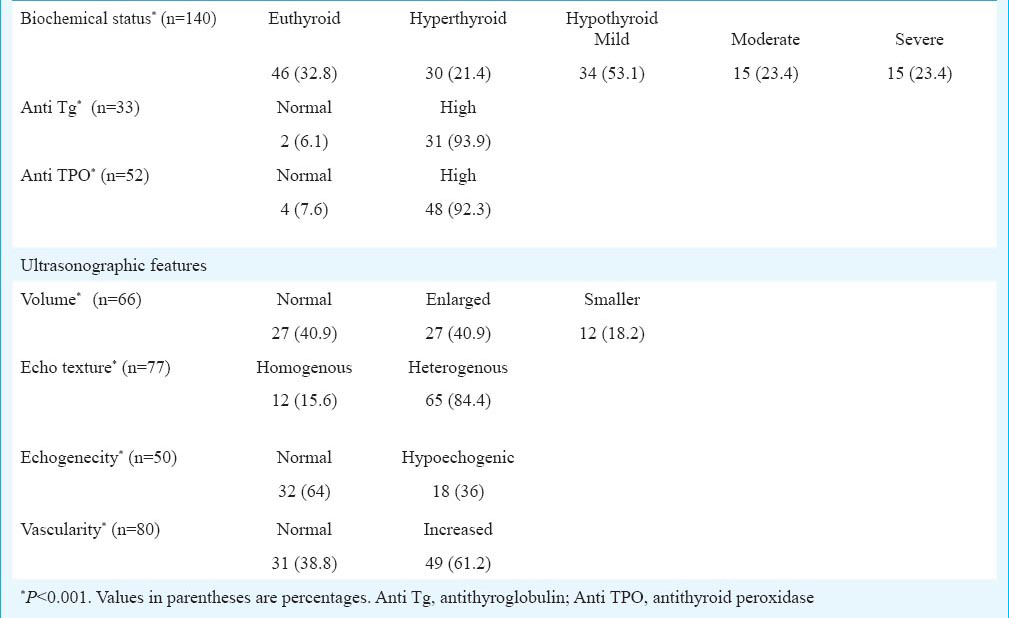
AntiTg antibody levels were available in 33 cases, 31 cases had high value. Anti TPO antibody levels were available in 52 cases, of whom 48 had high value indicating that a significant number of patients had high antithyroid antibody levels (P<0.001).
Of the 81 patients treated thyroxine supplementation was given to 63 patients, antithyroid drugs (neomercazole/carbimazole) to 19 and symptomatic treatment given to six patients (propranolol, alprazolam, paracetamol, diclofenac); 46 patients received no treatment and surgery was done in 17 cases. Among patients with cases with cytologic diagnosis of HT, nine were proven to be HT by histopathology also while two were shown to be multinodular goiter and colloid goiter. Among patients diagnosed as papillary carcinoma with LT, two cases underwent total thyroidectomy with neck dissection and one was treated with completion thyroidectomy after hemithyroidectomy. One patient of papillary carcinoma with LT was proven to be Hurthle cell adenoma with colloid adenomatous goiter with LT after histopathologic examination. Another patient of papillary carcinoma with LT also had a lymph node with adult T cell lymphoma.
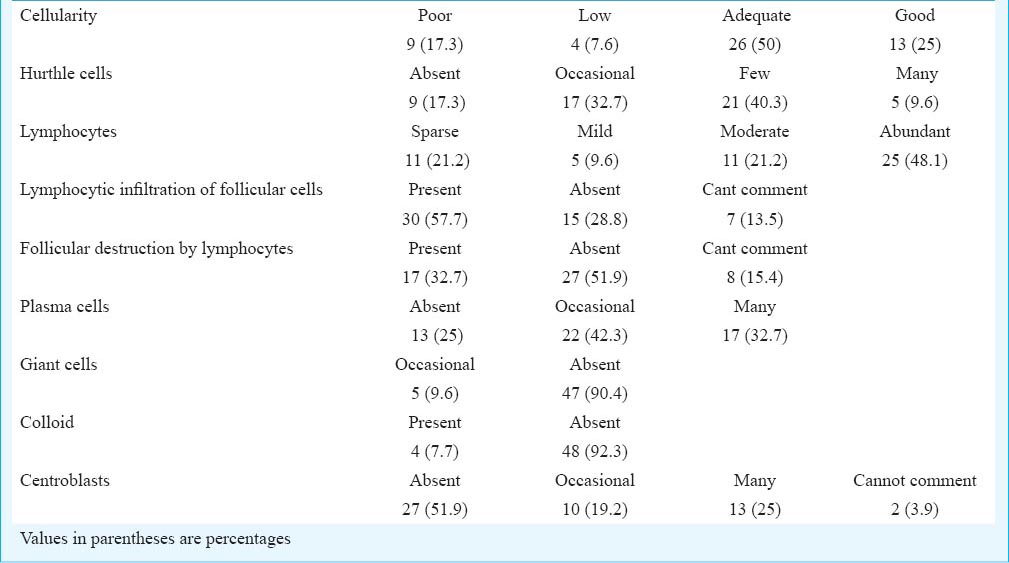
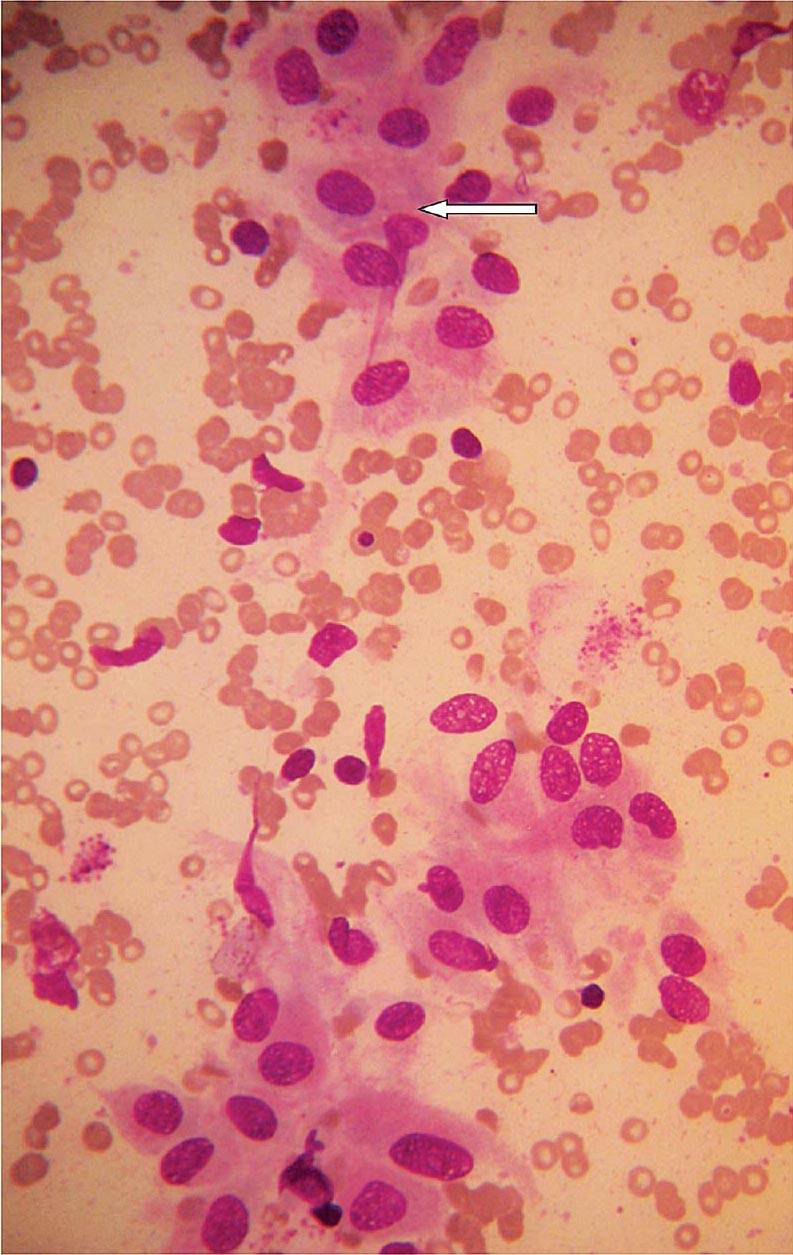
The various aspects studied in cytology were cellularity of smear, presence of follicular cells, Hurthle cells, degree of lymphocytes, presence of lymphocytic infiltration and destruction of follicular cells, presence of giant cells, colloid and lymphoepithelial (L:E) ratio (Table III). Cellularity of smears was assessed as good, adequate, low and poor. Lymphocytes seen in the smears were graded as sparse, mild, moderate, moderately dense or abundant (Fig. 1). Hurthle cells were absent in some smears, seen as occasional cells or small groups, or seen in many large groups (Fig. 2). Lymphocytic infiltration and destruction were graded as present or absent (Fig. 3). Centroblasts were absent, occasional or many. Colloid was absent in most with only two slides showing small blobs. Lymphoepithelial ratio ranged from 1:1 to 30:1.
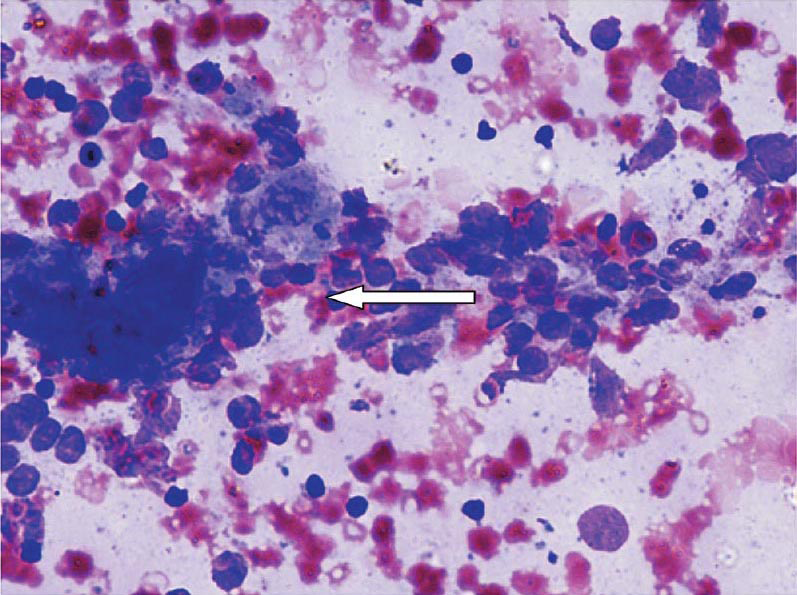
- Prominent lymphoplasmacytic infiltrate of thyroid (arrow) in Hashimoto's thyroiditis (May-Grunwald-Giemsa stain, ×400).
- Hashimoto's cell change of follicular cells of thyroid (arrow) in Hashimoto's thyroiditis (May-Grunwald-Giemsa stain, ×400).

- Follicular cell infiltration by lymphocytes of thyroid (arrow) in Hashimoto's thyroiditis (Papanicolaou stain, ×400).
The duration of symptoms was found to have a significant association with presence of goiter (P<0.05). There was no significant association between thyroid status and echogenicity of thyroid gland, antithyroid antibody, and intensity of lymphocytes, Hurthle cells, lymphocytic infiltration and destruction of follicular cells.
Discussion
Most of our patients with HT belonged to the 21-40 yr age group. In a study from Puducherry, maximum patients with HT were in their 3rd decade6. In another study from Chandigarh, majority of patients were in 3rd and 4th decades7. Unlike the Indian studies, studies from the West reported Hashimoto's thyroiditis being diagnosed between the 4th and 6th decades of life8. Thyroid diseases are always reported to be higher in the female population. The reported female to male ratio in Hashimoto's thyroiditis ranges from 15:1 to 3:167. Our gender ratio falls in this range. Most of our patients (61%) presented with symptoms of one year duration. The association of goiter with duration of symptoms before presentation was significant. But the biochemical thyroid status when associated with the same variable was found to have no significance. This shows that in our population, goiter but not symptoms of altered thyroid hormone status is a reason for seeking medical care.
The high occurrence (61%) of diffuse goiter in our study was similar to previous studies from India. In the study from Chandigarh on cytology proven Hashimoto's thyroiditis7, 93 per cent of patients had goiter, of whom 90 per cent were diffuse and 3 per cent were nodular. Nodules are seen in early stages of disease when clinical and hormonal changes are not yet established7. A study from Malaysia has reported that Indians have increased prevalence of diffuse goiter while Chinese have more of nodular presentation2.
Most of our patients were hypothyroid (subclinical and overt), and of these only 38 per cent showed overt hypothyroidism. These results were similar to previous studies from India67 and abroad2. In our study, 21 per cent patients had hyperthyroidism, not seen in other studies. It is interesting to note that 66 per cent of the hyperthyroid patients presented in less than one year duration for evaluation.
We found 93 per cent of our patients were anti TPO positive and 92 per cent of them were anti Tg positive. There is a well-recognized discrepancy between antibody levels and cytology in Hashimoto's thyroiditis in children and young adults9. This could be because that in early stage of disease, antibody production is confined to intrathyroidal lymphocytes10. On the other hand, patients with significant titres may not have cytology proven Hashimoto's thyroiditis. This can be explained by the fact that focal LT which is an early lesion may be missed by cytology9.
Ultrasonography reports were studied in a limited number of cases. In our study, the volume of gland was enlarged in 41 per cent and normal in another 41 per cent of patients. Studies have shown that thyroid volume changes as the disease progresses from euthyroid to overtly hypothyroid with smaller volumes found in overt hypothyroidism11. Our study showed 64 per cent cases with normal thyroid echogenicity and 36 per cent cases with diffuse hypoechogenicity. Low echogenicity is due to altered thyroid structure because of disruption of follicles and diffuse lymphocytic infiltration12. Studies from India13 and abroad12 have shown 80-85 per cent of cases having normal echogenicity.
In fine needle aspiration cytology of thyroid, L:E ratio (lymphoid:epithelial ratio) in Hashimoto's thyroiditis ranges from 2:1 to 10:16. We found moderate to abundant lymphocytic infiltrate in 69.3 per cent cases and lymphocytic infiltration of follicular cells in 57.7 per cent cases. An increase in number of epithelial cells raises suspicion of epithelial proliferative process associated with HT like malignancy6. Plasma cells were seen in 75 per cent of our cases. Plasma cells are useful in diagnosing early Hashimoto's thyroiditis where lymphocytic infiltration of follicles is insignificant6. A wide range of Hurthle cell change in Hashimoto's thyroiditis (48-98%) has been reported6. As seen in our study, absent or scanty colloid is a usual feature in Hashimoto's thyroiditis, but paradoxical presence of colloid1415 is not unusual due to a combination of iodine supplementation and autoimmunity6.
Our study showed no association between the thyroid status and antibody positivity, sonographic hypoechogenicity or cytologic parameters. Though many previous studies resemble ours6716, a few studies have shown positive correlation of biochemical parameters with reduction in echogenicity in sonography1213, lymphocytic infiltration1314 and antibody status13. A study with long term follow up has reported presence of raised TSH along with positive TPO antibodies which raises the risk of developing overt hypothyroidism17.
Various neoplastic and non-neoplastic lesions are shown to be associated with HT on FNA like colloid goiter, cellular adenoma, follicular neoplasm, Hurthle cell neoplasm, papillary carcinoma, non-Hodgkins lymphoma (NHL) and follicular carcinoma6. Therefore four cases of malignancies associated with HT on cytology in our study group, three of whom were papillary carcinoma and one was medullary carcinoma.
The most commonly encountered neoplasms in association with HT are papillary thyroid carcinoma (PTC) and primary thyroid lymphoma. Several studies have attempted to define relationship between HT and PTC. In a population of patients with thyroid cancers, 1.9 times higher rate of HT were seen in patients with PTC, when compared with other cancers. On the other hand, there is a 2-3 times increased risk of development of PTC in presence of HT18. The presence of a dominant nodule, decreased response to suppressive therapy or clinical signs of metastasis should raise suspicion of PTC in patients with HT. FNA is useful in diagnosis of patients with HT associated lesions with a sensitivity of >90 per cent18. Many studies have been done on the prognosis of LT in PTC, majority of these reporting protective role of autoimmunity in terms of less aggressive disease at presentation, low recurrence19 and improved survival18.
Our study had several limitations. The lack of complete data for all variables in all patients has reduced the sample size in the analysis of the various parameters. Antithyroid antibody levels were available only in a few patients, cost constraints being the main limiting factor. T3, T4, TSH and antibody levels at the time of presentation to hospital were taken.
In conclusion, Hashimoto's thyroiditis was diagnosed in goiter in our patients who came from the iodine sufficient western coastal belt. The presence of goiter and hypothyroidism points towards the necessity of further evaluation of disease. Ultrasound compliments diagnosis with its characteristic features but cytology is confirmatory. Association of HT with malignancy requires a close follow up of these patients.
Acknowledgment
The study was partially supported by the TMA Pai Research grant (Manipal University), Manipal, India.
References
- Thyroid disorders in India: an epidemiological perspective. Indian J Endocrinol Metab. 2011;15(Suppl 2):78-81.
- [Google Scholar]
- The role of iodine in thyroid autoimmunity: from chickens to humans: a review. Autoimmunity. 1992;13:61-8.
- [Google Scholar]
- Cytomorphologic study of Hashimoto's thyroiditis and its serologic correlation: a study of 150 cases. Acta Cytol. 2009;53:507-16.
- [Google Scholar]
- Lymphocytic thyroiditis - is cytological grading significant? A correlation of grades with clinical, biochemical, ultrasonographic and radionuclide parameters. Cyto Journal. 2007;4:10.
- [Google Scholar]
- Increased incidence of well-differentiated thyroid cancer associated with Hashimoto's thyroiditis and the role of the PI3k/Akt pathway. J Am Coll Surg. 2007;204:764-73. discussion 773-5
- [Google Scholar]
- Hashimoto's thyroiditis: countrywide screening of goitrous healthy young girls in postiodization phase in India. J Clin Endocrinol Metab. 2000;85:3798-802.
- [Google Scholar]
- Seronegative Hashimoto thyroiditis with thyroid auto antibody production localized to the thyroid. Ann Intern Med. 1988;108:26-30.
- [Google Scholar]
- Thyroid sonography in autoimmune thyroiditis. A prospective study on 123 patients. Acta Endocrinol (Copenh). 1990;122:391-5.
- [Google Scholar]
- Thyroid ultrasonography helps to identify patients with diffuse lymphocytic thyroiditis who are prone to develop hypothyroidism. J Clin Endocrinol Metab. 1991;72:209-13.
- [Google Scholar]
- Clinical, biochemical and cytomorphological observations in juvenile chronic lymphocytic thyroiditis. Indian Pediatr. 1998;35:967-73.
- [Google Scholar]
- Aspiration cytology of Hashimoto's thyroiditis in an endemic area. Cytopathology. 2002;13:31-9.
- [Google Scholar]
- Hashimoto's thyroiditis: fine-needle aspirations of 50 asymptomatic cases. Diagn Cytopathol. 1994;11:141-5.
- [Google Scholar]
- Correlation of number of intrathyroid lymphocytes with antimicrosomal antibody titer in Hashimoto's thyroiditis. Diagn Cytopathol. 2003;28:63-5.
- [Google Scholar]
- Natural history of autoimmune thyroiditis. Br Med J (Clin Res Ed). 1981;282:258-62.
- [Google Scholar]
- Coexistent Hashimoto's thyroiditis with papillary thyroid carcinoma: impact on presentation, management, and outcome. Surgery. 1999;126:1070-6. discussion 1076-7
- [Google Scholar]
- Clinical and pathological implications of concurrent autoimmune thyroid disorders and papillary thyroid cancer. J Thyroid Res 2011 2011 387062
- [Google Scholar]




