Translate this page into:
Brown-Séquard syndrome
* For correspondence: senthilkumarpgi@yahoo.co.in
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 57 yr old male was brought to Radiology department, Saveetha Medical College Hospital, Thandalam, Tamil Nadu, India, for evaluation of cervical spine in June 2013. He had history of stab injury to the right side of neck following which the patient developed ipsilateral hemiparesis and contralateral sensory loss below C6 dermatome. On right side, positive Babinski's sign was noted with no abdominal and cremasteric reflexes. No leakge of cerebrospinal fluid (CSF) was noted from the wound. Magnetic resonance imaging (MRI) of cervical spine revealed C6-C7 block vertebra with focal linear hyperintensity in right side of cervical spinal cord at the same level (Figs. 1, 2). Diagnosis of Brown-Séquard syndrome (BSS) due to cord hemitransection was made. The patient was managed conservatively with cervical spine stabilization and supportive and physical therapy. He is under follow up for the past six months and has shown progressive improvement in muscle power and sensation with only mild residual paresis of right lower limb.
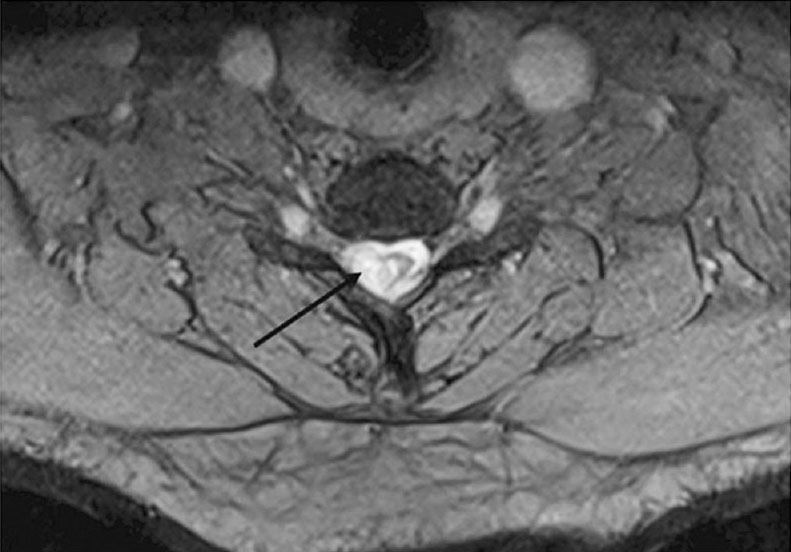
- Axial gradient MR image showing hyperintensity (black arrow) in right side of lower cervical spinal cord. Involved part of cord also appears oedematous.
-
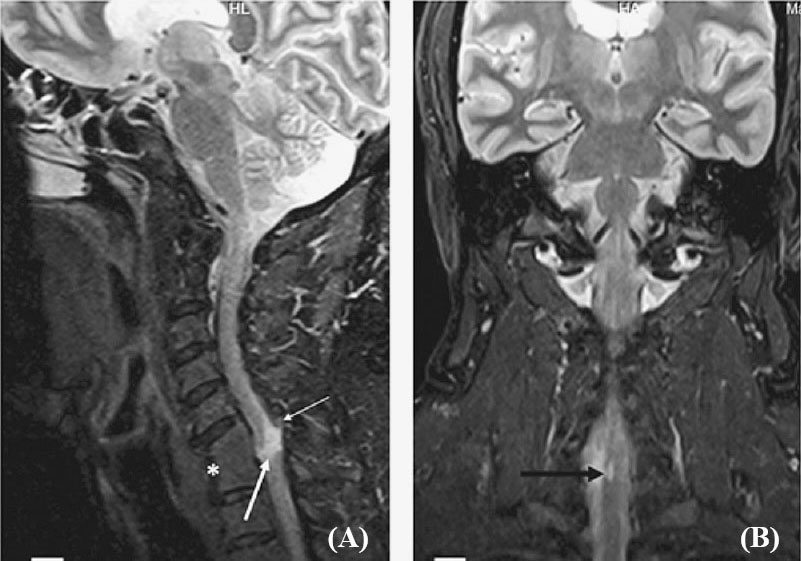
(A) Sagittal short tau inversion recovery (STIR) MR image showing C6-C7 block vertebra (white asterisk) with a focal linear hyperintensity in spinal cord (thick white arrow) at this level. Focal disruption of ligamentum flavum is also noted (thin white arrow). (B) Coronal STIR MR image showing focal hyperintensity confined to right side of cervical spinal cord (black arrow).
Brown-Séquard syndrome is characterized by anatomical disruption of nerve fibre tracts in one half of spinal cord. Disruption of descending lateral corticospinal tracts, ascending dorsal column and ascending spinothalamic tracts leads to ipsilateral hemiplegia and loss of proprioception and vibration with contralateral loss of pain and temperature sensation below the level of injury1. Common causes of BSS include cord trauma, neoplasms, disk herniation, demyelination, infective/ inflammatory lesions or epidural hematomas with penetrating trauma to cord being commonest cause123. In literature, very few cases of penetrating stab cord injury presenting with pure BSS have been described14. Management of BSS depends on the causative pathology. Need for conservative or surgical management depends on patient's neurological status and clinico-radiological findings. Surgery intervention is advised in post-traumatic BSS if there is presence of retained foreign objects, CSF leakage, infection or signs of extrinsic spinal cord compression. Medical management is preferred for infective/ inflammatory or demyelinating causes of BSS while surgical treatment is performed for pathologies causing extrinsic cord compression23.
References
- Brown-Séquard syndrome in a 11-year-old girl due to penetrating glass injury to the thoracic spine. Eur J Orthop Surg Traumatol. 2013;23(Suppl 2):S141-3.
- [Google Scholar]
- Cervical epidural haematoma causing Brown-Sequard syndrome: a case report. J Orthop Surg (Hong Kong). 2013;21:372-4.
- [Google Scholar]
- Management of Brown-Sequard syndrome in cervical disc diseases. Turk Neurosurg. 2013;23:470-5.
- [Google Scholar]
- Radiographic and intraoperative imaging of a hemisection of the spinal cord resulting in a pure Brown-Séquard syndrome: case report and review of the literature. J Neurosurg Sci. 2013;57:81-6.
- [Google Scholar]




