Translate this page into:
Tsunami, post-tsunami malaria situation in Nancowry group of islands, Nicobar district, Andaman and Nicobar Islands
Reprint requests: Dr Paluru Vijayachari, Director, Regional Medical Research Centre (ICMR), Post Bag No.13, Dollygunj Port Blair 744 101, Andaman and Nicobar Islands, India e-mail: sathyamanimunda@rediffmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Due to tsunami in 2004 a large proportion of population in Nicobar group of Islands become homeless, and in 2006 large scale labour migration took place to construct the houses. In 2008, a significant increase in malaria incidence was observed in this area. Therefore, in March 2008, the situation of malaria was assessed in Nancowry Islands in Nicobar District to study the reasons for the observed upsurge in the number of cases, and to suggest public health measures to control the infection.
Methods:
The methods included a retrospective analysis of long term trend in the behaviour of malaria over the years from 2001 to 2008, analysis of the acute malaria situation, and rapid fever and malaria parasitemia survey along with environmental component. Mass radical therapy (MRT) and post-intervention parasitemia survey were carried out. The malaria situation in the aftermath of MRT was analysed.
Results:
During the post tsunami year (2005) there was a large increase in the incidence of malaria and this trend continued till 2008. The percentage of Plasmodium falciparum increased from 23 to 53 per cent from 2006 to 2007 that coincides with the labour influx from mainland. The study showed that Nancowry was highly endemic, with high transmission setting, and high risk area for malaria. Though, more number of migrant labourers suffered fever (75 vs 20%) and sought malaria treatment over past month but parasitemia survey showed higher point prevalence of malaria among native tribes (7.4 vs 6.5%). Post-MRT, there was a decline in the occurrence of malaria, though it did not last long.
Interpretation & conclusions:
The study findings suggest that the migrant workers hailing from non-endemic or moderately endemic settings became victims of malaria in epidemic proportion in high endemic and high transmission setting. To find out the reasons for deterioration of malaria situation at Nancowry in the aftermath of tsunami requires further research.
Keywords
Andaman and Nicobar Islands
construction
labour migration
malaria
Plasmodium falciparum
tsunami

About half the world’s population (3.3 billion) live in areas that have some risk of malaria transmission and one fifth (1.2 million) live in areas with a high risk of malaria (more than 1 reported case per 1000 population per year). India had an estimated 10.6 million malaria cases in 2006 that account for approximately 60 per cent of cases in the WHO South- East Asia region1.
Andaman and Nicobar Islands, a union territory of India, has historically been known for high malaria transmission2. Nicobar group of islands lie 143 miles south of Port Blair, capital of archipelago3. During the recent past the malaria situation in Nicobar group of islands is worse in comparison with Andaman group of islands4. The tropical climate prevailing throughout the year provides ideal environment for mosquito proliferation and breeding in Nicobar group of islands5. Entire land mass in the islands has network of creeks which results in an ideal brackish water habitats for the breeding of Anopheles sundaicus, the predominant vector of malaria in Andaman and Nicobar Islands6–9.
December 26, 2004 earthquake and subsequent tsunami caused inundation of sea water in to inland up to 1000 m10. The intense geological activity resulted in raising of north Andaman between 0.5 and 0.8 m, whereas the south Andaman and Nicobar experienced subduction of similar intensity1011. Natural disaster, particularly meteorological events such as cyclones, hurricanes, flooding, and tsunami can affect vector breeding sites and vector-borne disease transmission12. The crowding of infected and susceptible hosts, a weakened public health infrastructure and interruption of ongoing control programmes are all risk factors for vector- borne disease transmission1314.
In the aftermath of tsunami the spread and risk of malaria in the affected places was anticipated by experts15. As anticipated, in 2005, there was an increase of 1243 per cent in annual parasite incidence (API) (from 0.64 to 8.15) for Andaman District and it was almost 816 per cent (from 8.0 to 73.27) for Nicobar District. In the subsequent years after 2005, in the Nicobar group of Islands the malaria situation differed from island to island. A control was achieved in Car Nicobar but it deteriorated in Nancowry16.
Due to tsunami entire 45000 population of Nicobar group of Islands rendered homeless. Hence, from mid 2006 onwards large scale labour migrations from the districts of West Bengal started and were engaged in the construction of permanent shelters for the tsunami affected population. Population mobility due to various economic pressures and necessities is incriminated as one of the reason for complicating, as well changing the epidemiology of malaria17–21.
In March 2008, a large increase in the occurrence of malaria was observed in Nancowry group of islands, Nicobar District. In response to this, a team from the Centre was deputed to these islands to assess the situation of malaria. This study was carried out to confirm the diagnosis and the increase in the incidence of malaria as well to identify the possible causes of this increase, and to suggest measures for control of malaria in Nancowry group of islands.
Material & Methods
Study area:
The study was carried out in the jurisdiction of Community Health Centre (CHC), Nancowry, situated at Kamorta. Nancowry is the central group of islands in Nicobar District with hilly terrain covered with grass, forming undulating meadows. It consists of 12 villages, many are islands connected only by sea route. The population of the CHC area in 2008 was 4875, all aboriginal Nicobarese tribe3. Though the 2004 earthquake and subsequent tsunami damaged the dwellings of aborigines but loss of life was less than 20 persons. From mid 2006 onwards around 600 migrant male labourers from the districts of West Bengal were engaged in construction of permanent shelters in these islands. There was constant movement of labourers between these islands and main land India since mid 2006 with fresh batch replacing the one which went back. No batch stayed more than four months. The main reason for return was illness with fever presumed to be malaria. During February 2008 a fresh contingent of around 300 labourers arrived to Nancowry. During the time of study there were around 600 migrant male labourers aged between 18 to 55 yr. They were living in 6 of 12 villages of Nancowry in labour camps.
The methods of investigations included:-
A retrospective analysis of long-term trend in the behaviour of malaria over the years from 2001: Number of smears examined and positive cases over a period of seven years was collected from malaria surveillance data (Sur SK, personal communication). The number of tribal population during the years 2001-2008 was obtained from the register maintained in CHC, Nancowry, and migrant labourers were obtained from the Office of the Assistant Commissioner (AC), Nancowry. Monthly parasite incidence (MPI) and annual parasite incidence (API) were plotted to understand the long term and seasonal trend in the occurrence of malaria. The break-up of proportion of blood smears examined by active and passive surveillance was calculated. The statistical significance in change of API over previous year, the change in proportion of Plasmodium falciparum (Pf) cases over previous year, and the change in annual blood examination rate (ABER) over previous year (all from 2001-2007) was tested by χ2 test.
Analysis of the acute malaria situation: The daily number of confirmed cases of malaria detected from March 1, 2008 was compared with that during the same months for the previous year. The number of confirmed cases of malaria attending CHC, Nancowry, and the demographic details of patients such as age, sex, ethnicity, etc. were collected for a period of past three months. Incidence of acute malaria infections (percentage by age) among stable indigenous Nicobarese population from January 2008 to March 2008 was calculated to know the endemicity level of malaria at Nancowry22. Monthly incidence of malaria for preceding three months was calculated from the hospital registry of CHC, Nancowry; among native tribes and migrant labourers separately and the statistical significance in difference was tested by χ2 test. Slide positivity rate (SPR) was calculated for past three years and past three months separately to analyze the parasite buildup in the community2324.
-
Rapid fever and malaria parasitemia survey: A cross-sectional survey was carried out in March 2008 to estimate the point prevalence of fever and malaria among indigenous tribal population and migrant labourers. This was carried out in six villages where 2743 tribal population and almost all 600 odd migrant labourers lived, prior to mass radical therapy (MRT). In these six villages every third household was surveyed from the list maintained in CHC, Nancowry, and first household being a random choice. Similarly every third labourer was chosen from each camp first being a random choice, from a list maintained in Office of AC, Nancowry. Informed consent from all the subjects was taken. Information about the history of fever during past month and bed net usage was also sought.
The difference in point prevalence of fever and slide positivity among indigenous tribes and migrant labourers, the difference in slide positivity of young tribal children (aged < 10 yr) and elder tribal, as well the difference in proportion of history of having fever over past month among indigenous tribes and migrant labourers were tested by χ2 test.
Environmental observation: An observation was made for the possible breeding sites of vector mosquito.
Mass intervention: MRT was carried out in all the 12 villages and entire 4875 tribal people and 600 odd migrant labourers by Health Services, 600 mg of chloroquine and 45 mg of primaquine was administered from April 05-07, 2008. For children age appropriate dose was given and pregnant mothers were exempted. It was supervised and directly observed treatment (DOT) given and informed consent from all the subjects was taken.
Post intervention malaria parasitemia survey: Cross-sectional survey for malaria parasitaemia was repeated 8-10 days after initiating MRT. Information on compliance with MRT was also obtained by interviewing the subjects. This survey was carried out in the same six villages and among same house-holds and subjects. Every second household from the previously surveyed households were chosen, first being a random choice and among migrant labourers every second labourer was chosen from the previously surveyed labourers, first being random choice. Informed consent from all the subjects was taken.
The study of malaria situation post-intervention: Day wise occurrence of malaria in April 2008 was compared with the same in April 2007. The MPI in the subsequent months following MRT was compared with the same months of previous year. The statistical significance was tested by χ2 test. The malaria situation at Nancowry during the year 2008 was analysed by calculating API, percentage (%) of Pf and ABER. The statistical significance of change in API, percentage of Pf, and ABER over previous year was tested by χ2 test.
Results
Fig. 1 shows the MPI of confirmed cases of malaria at CHC, Nancowry for 2001-2007. Malaria occured in all months. There was a peak in the month of June in all years. There was a large increase in API during 2005 (post tsunami year) and percentage of Pf during 2007 (Table I). Almost 2/3rd of the smears examined were by active surveillance.
| Year (population) | Smears examined, No. (%) | Total confirmed cases | API/1000 | Change in API over previous year (%) | % of Pf | Change in % of pf over previous year (%) | ABER | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Active | Passive | Total | ||||||||
| 2001(4573) | 3706 (64) | 2084 (36) | 5790 | 490 | 107.2 | 23 | 126.6 | |||
| 2002 (4614) | 4072 (70) | 1745 (30) | 5817 | 230 | 49.9** | -53 | 14** | -39 | 126.1 | |
| 2003 (4656) | 3340 (58) | 2419 (42) | 5759 | 373 | 80.1** | +61 | 20* | +43 | 123.7* | |
| 2004 (4699) | 3584 (65) | 1930 (35) | 5514 | 391 | 83.2 | +4 | 15 | -25 | 117.3** | |
| 2005 (4742) | 5920 (70) | 2537 (30) | 8457 | 798 | 168.3** | +102 | 22* | +47 | 178.3** | |
| 2006 (4786+600) | 3917 (60) | 2611 (40) | 6528 | 815 | 151.3* | -10 | 23 | +5 | 121.2** | |
| 2007 (4830+600) | 8299 (70) | 3556 (30) | 11855 | 949 | 174.8** | +16 | 53** | +130 | 218.32** | |
(API=Total confirmed cases in a year/total population×1000); ABER annual blood examination rate (ABER, Total blood smears examined in a year/total population×100);
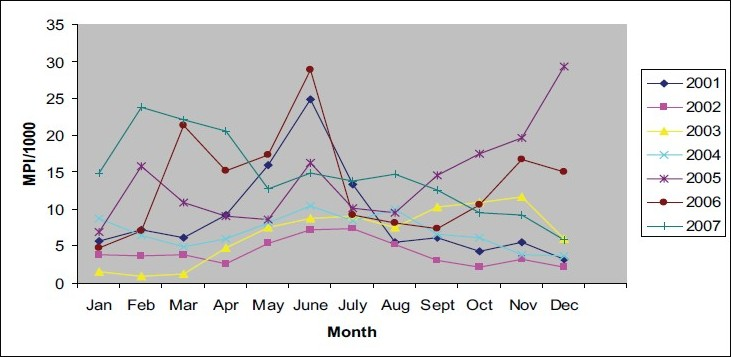
- Monthly parasite incidence (MPI) at CHC, Nancowry, 2001-2007.
There was steady increase in the occurrence of malaria during the last week of March 2008 when compared with March 2007 of the same period (Fig. 2).
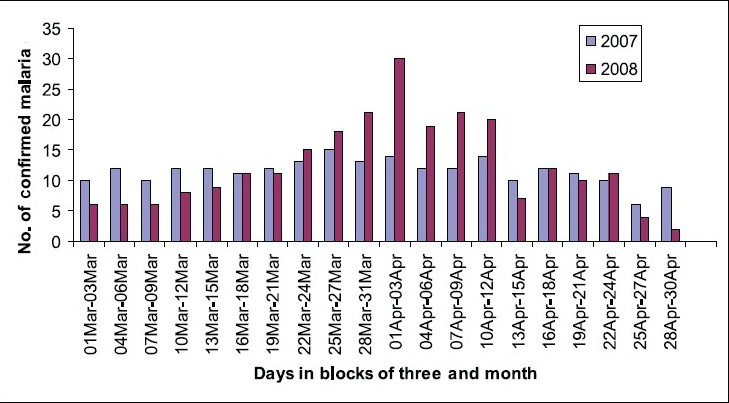
- Occurrence of malaria March 2007 versus March 2008 and April 2007 versus April 2008 at CHC, Nancowry.
Incidence of acute malaria infections (percentage by age) among the Nicobarese showed high age specific incidence in late infancy or early childhood and among adolescents less and still less in adults indicative of high endemicity (Fig. 3).
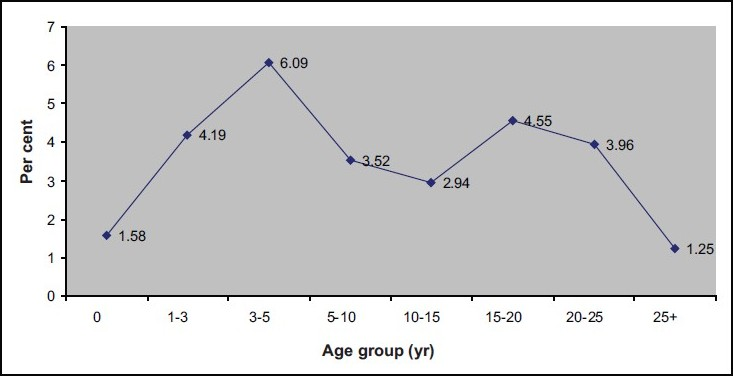
- Incidence of acute malaria infections (percentage by age) among stable indigenous Nicobarese population (January-March 2008).
It was found that the monthly incidence of malaria during January, February and March 2008 among migrant labourers was significantly higher (P,<0.01) than that among the Nicobarese (Table II).
| Malaria incidence, 2008 (%) | |||
|---|---|---|---|
| Population | January | February | March |
| Nicobarese tribe | 0.84 (41/4875) | 0.92 (45/4875) | 0.73 (36/4875) |
| Migrant labourers | 4.5* (27/600) | 10.83* (65/600) | 12.5* (75/600) |
The slide positivity rate (SPR) for the year 2008 till April 4 was 8.60 per cent (277/3218). The SPRs for preceding three years, i.e. 2007, 2006, and 2005 were 8.0 per cent (949/11855), 12.48 per cent (815/6528), and 9.43 per cent (798/8457) respectively (Mean: 9.97). There was no increase in the SPR till April 4th 2008 in comparison with preceding three years.
The SPR for initial four days of April 2008 was 20 per cent (70/350). The SPR for preceding three months, i.e. January, February, and March 2008 was 4.94, 7.90, and 8.88 respectively (mean ± SD: 7.24 ± 2.05). The SPR during the first week of April 2008 exceeded by more than three times of the standard deviation observed in SPR of the preceding 3 months of the same year.
Almost 30 per cent (823/2743) of the Nicobarese tribes and 30 per cent (217/600) of the migrant labourers were included in the rapid fever and malaria parasitemia survey. Among aborigines 51 per cent (420/823) were males and 49 per cent (403/823) were females and around 8 per cent (66/823) were aged <5 yr and almost 16 per cent (130/823) were aged <10 yr. This figure was comparable to the gender and age composition of CHC, Nancowry. The migrant labourers were aged between 18 and 55 yr and all were males.
Overall point prevalence of fever was 12.0 per cent [95% Confidence Interval (CI):10.1, 14.2] (125/1040). The point prevalence of fever among persons belonging to indigenous tribe was 10.3 per cent (95% CI: 8.3, 12.6) (85/823). Among migrant labourers it was 18.4 per cent (95% CI: 13.5, 24.2) (40/217). This difference in point prevalence of fever was statistically significant (P<0.01).
The overall slide positivity rate was 7.2 per cent (95% CI: 5.7, 8.9) (75/1040). The percentage of Pf was 56 per cent (42/75). The slide positivity rate among tribal was 7.4 per cent (95% CI: 5.7, 9.4) (61/823). The positivity rate among tribal children aged < 10 yr was 13 per cent (17/130), whereas that among older tribal people was 6.3 per cent (44/693). The difference was statistically significant (P<0.01). The slide positivity rate among migrant labourers was 6.5 per cent (95% CI: 3.6, 10.6) (14/217). The difference in the slide positivity rate among Nicobarese tribe (7.4%) and among migrant labourers (6.5%) was statically not significant. Out of the 40 tribal children aged <10 yr who had fever during the time of cross-sectional survey, 17 (42.5%) tested positive for malarial parasite.
Almost 10 per cent (6/61) of the tribal adults had asymptomatic parasitemia and none among migrant labourers. Over the past one month almost 75 per cent (163/217) of the migrant labourers and 20 per cent (165/823) aborigines reported having suffered fever. The difference was statistically significant (P<0.01). Bed net usage among the population of the island was almost 100 per cent (1039/1040). Impregnated bed net was not used by migrant labourers.
The heavy rain fall during the study period helped in better understanding of possible ecological reasons aiding vector proliferation. Four important observations were made: (i) The contact of sea water to the inland has increased due to geographic tilt. (ii) The habitat of tribal was shifted from sea shore to interior jungles to open temporary shelters following tsunami and this might have increased the chances of getting bitten by vector mosquito. (iii) The ongoing large scale construction activity and digging of land has created numerous artificial habitats for the breeding of mosquitoes. (iv) In the low lying areas the inundation of sea water and subsequent trapping has created numerous pools of water and the monsoon streams have become more stagnant in the aftermath of tsunami.
The reported coverage of MRT was 90 per cent among aborigines and 96 per cent among migrant labourers. Post MRT the peripheral blood smear of 500 subjects in the same six villages were taken and examined for malarial parasites. This included 15 per cent (410/2743) of the aborigines and 15 per cent (90/600) of the migrant labourers. Only two subjects of native tribe tested positive for malarial parasite and both were Pf species. One did not receive MRT and the other was a child aged 3 yr. None of the migrant labourers were positive for malaria parasite. Almost 5 per cent (4/90) of the migrant labourers and 7 per cent (30/410) of the native tribes missed MRT for one or the other reasons.
There was a fall in occurrence of malaria in April 2008 at CHC, Nancowry following the administration of MRT (Fig. 2). Table III shows the occurrence of malaria cases at CHC, Nancowry, during the subsequent months of 2008 following MRT and the comparison between the occurrences of malaria cases during the same months in 2007. The decrease in the occurrence of malaria was statistically significant (P<0.01) only in the month of June, 2008.
| Month | Number of malaria cases | P | |
|---|---|---|---|
| 2007 (MPI/1000) | 2008 (MPI/1000) | ||
| May | 69 (12.7) | 53 (9.7) | 0.14 |
| June | 81 (14.9) | 51 (9.3) | < 0.01 |
| July | 75 (13.8) | 58 (10.6) | 0.13 |
| August | 80 (14.7) | 83 (15.2) | 0.81 |
| September | 68 (12.5) | 76 (13.9) | 0.50 |
| October | 52 (9.6) | 123 (22.5) | < 0.01 |
| November | 50 (9.2) | 128 (23.4) | < 0.01 |
| December | 32 (5.9) | 134 (24.5) | < 0.01 |
MPI, monthly parasite incidence
The API for 2008 was 207.5/1000 (1136/5475), percentage of Pf was 53.3 per cent (606/1136), and ABER was 243.0 per cent (13307/5475). In 2008 there was an increase of 18.7 per cent in API in comparison with 2007 (Table I) The increase in API and ABER during 2008 was statistically significant (P<0.01).
Discussion
Our results showed a large increase in the incidence of malaria in the post tsunami year (2005) and the trend continued till 2008. The geological and environmental changes happened due to tsunami might have contributed to this. The consequent construction activity and labour influx further complicated the malaria situation. A study carried out in the districts of south Andaman in the aftermath of tsunami has highlighted increased salinity of inland water as one of the important risk factor favouring the breeding of An. sundaicus25.
The other revelation of the study was that of almost doubling of percentage of Pf in 2007 and 2008. The increase in incidence of Pf coincided with the increased influx of labour from the districts of West Bengal and the beginning of large scale construction activity.
The present study arrived at three important epidemiological deductions. One, the incidence of acute malaria infections (percentage by age) among the stable indigenous Nicobarese population was indicative of high endemicity of malaria in Nancowry group of islands22. Two, more than 5 per cent of the tribal children aged < 10 yr presenting with fever turned positive for malaria parasite indicating high transmission setting26. Three, the study identified Nancowry group of islands as high risk area for malaria transmission i.e., SPR for the past three years was more than 5 per cent, Pf proportion was more than 30 per cent, and the tropical aggregation of labour in Nancowry Islands23.
Though, the patient register maintained at CHC, Nancowry, showed higher incidence of malaria among migrant labourers than indigenous tribal people but, the mass malaria pasitemia survey showed higher point prevalence of malaria among indigenous tribe. This could be due to low health seeking behaviour of the tribes. This is evidenced by lower proportion of smears examined by passive surveillance at CHC, Nancowry. The findings that 10 per cent of native tribes had asymptomatic parasitemia, and almost 75 per cent of labourers suffered from fever during the past month is a pointer that the workers hailing from non-endemic or moderately endemic settings became victims of malaria in epidemic proportion in high endemic and high transmission setting. They visited CHC, Nancowry and got treated with anti-malarials. This may be the reason for low point prevalence of malaria among migrant labourers in comparison with indigenous tribe.
The SPR for the first week of April 2008 was more than 3SD of the average for past three months indicating the build up of parasite in the community2324. Though mass drug administration (MDA) or MRT has limited role in the long term control of malaria, these could have a part to play in the management of epidemics27. Moreover, in some cases, it had a marked effect on parasite prevalence and on the incidence of clinical malaria28. The short term effect of MRT was dramatic as evidenced by post-intervention parasitemia survey. It had no effect on long term control of malaria.
In India, insecticide impregnated bed nets (IIBNs) with pyrethroids have been tried for malaria control with variable results29–33. Lambdacyhalothrin IIBNs distributed in an endemic tract of Orissa, showed overall decline in parasite rates among all age groups, while it was well received and accepted by the local tribals of Assam, following which the SPR decreased significantly3031. In Nancowry, though the usage of bed net was almost 100 per cent (with the exception that migrant labourers) but it did not help much in containing malaria in this island. This emphasizes the fact that malaria control needs multi-pronged approach.
The limitation of the study was that the entomological aspect was not looked into. Secondly, the study was carried out in a far flung island almost 350 km away from base station, hence there were innate logistical difficulties in covering larger sample of the population for mass fever and malaria parasitemia survey. Higher sample size in post-intervention survey would have helped in analysing the effect of MRT in better way.
In conclusion, there was a deterioration of malaria situation at Nancowry post tsunami. The MRT had dramatic immediate effect on the occurrence of malaria but from long-term perspective it had no effect. To validate the hypothesized reasons for the increased occurrence of malaria following tsunami further studies are required and this will help evolve appropriate intervention strategy.
The authors acknowledge the support of then Assistant Commissioner of Nancowry Shri Bajaranga Lal, and BDO Shri Rajesh, and thank Dr N. Sadasivan, Director, Directorate of Health Services, A&N Islands for his co-operation. Authors also acknowledge the participation of the entire malaria staff of the DHS, A&N Islands, during the field operation in combating malaria in one of the geographically difficult and dangerous terrain in Bay of Bengal.
Conflicting interest: None.
References
- World Health Organization. In: World Malaria Report. Geneva: Switzerland: WHO; 2008.
- [Google Scholar]
- Malaria’s indirect contribution to all-cause mortality in the Andaman Islands during colonial era. Lancet Infect Dis. 2008;8:564-70.
- [Google Scholar]
- District Administration, Nicobar District, Andaman and Nicobar Islands, Introduction, Nicobars - land and its people. available from: http://nicobar.nic.in/island_wise_info.htm, accessed on March 20, 2009
- Malaria Research Centre document. Car Nicobar (Andaman and Nicobar Islands). Available from: www.mrcindia.org/idvc-profile/14.pdf, accessed on January 26, 2008
- District Administration, Nicobar District, Andaman and Nicobar Islands, Location/climate, General information. Available from: http://nicobar.nic.in/island_wise_info.htm, accessed on March 20, 2009
- On the anthrophilic indices of some Anopheles found in east central India. Indian J Malariol. 1947;1:111-22.
- [Google Scholar]
- Report of an enquiry into malaria conditions in the Andamans. Delhi: Government of India Press; 1927.
- Science and Technology Project Report on integrated vector control of malaria, filaria and other vector borne diseases; - Annual Report. Delhi: Malaria Research Centre; 1989. p. :374-7.
- Inundation of sea water in Andaman and Nicobar Islands and parts of Tamil Nadu coast during 2004 Sumatra tsunami. Curr Sci. 2005;88:1736-40.
- [Google Scholar]
- National Institute of Public Finance and Policy, New Delhi. State Development Report of Andaman & Nicobar Islands. June. 2006. p. :142. Available from: www.nipfp.org.in/State%20 Development%20Report%20of%A&-Final%20(June%20 06).pdf, accessed on January 26, 2008
- El Nino and associated outbreaks of severe malaria in highland populations in Irian Jaya, Indonesia: a review and epidemiological perspective. Southeast Asian J Trop Med Public Health. 1999;30:608-19.
- [Google Scholar]
- World Health Organization. Communicable diseases following natural disasters: risk assessment and priority interventions 2006
- [Google Scholar]
- Malaria prevalence in Nias District, North Sumatra Province, Indonesia. Malar J. 2007;6:116-23.
- [Google Scholar]
- World Health Organization. In: Malaria risk and malaria control in Asian countries affected by the tsunami disaster, Roll Back Malaria Department, WHO/HQ. Technical note: Geneva, Switzerland: WHO; 2005.
- [Google Scholar]
- Malaria in Car Nicobar Island in the aftermath of tsunami: Some observations. Natl Med J India. 2009;22:217-8.
- [Google Scholar]
- Population movement and malaria persistence in Rameswaram Island. ICMR Bull. 1984;14:125-33.
- [Google Scholar]
- Ecology, economics and political will: the vicissitudes of malaria strategies in Asia. Parasitologia. 1998;40:39-46.
- [Google Scholar]
- Endemic coastal malaria in the Thousand Islands District, near Jakarta, Indonesia. Trop Med Int Health. 2005;10:489-96.
- [Google Scholar]
- Population movement, socio-economic behaviour and the transmission of malaria in Northern Thailand. Southeast Asian J Trop Med Public Health. 1986;17:396-405.
- [Google Scholar]
- World Health Organization. In: Malaria control in complex emergencies: an inter-agency field handbook. Geneva, Switzerland: WHO; 2005.
- [Google Scholar]
- State Malaria Control Society, Gujarat. Enhanced malaria control project, Gujarat State. Malariology course for medical officers of primary health centres, 2002-03. Gandhingar (Gujarat, India): State Malaria Control Society, Gujarat; 2002-03. Available from: gujhealth.gov.in/health_programmes/malaria/pdf/moohc_module.pdf, accessed on March 20, 2009
- National Vector Borne Disease Control Programme. Malaria Surveillance (Document). Available from: http://nvbdcp. gov.in/Doc/Director&20Desk/Malaria&20Surveillance&20 -&203.doc, accessed on March 20, 2009
- Altered environment and risk of malaria outbreak in South Andaman, Andaman & Nicobar Islands, India affected by tsunami disaster. Malar J. 2005;4:32-40.
- [Google Scholar]
- Global Malaria Programme. Guidelines for the treatment of malaria. In: Guidelines for the treatment of malaria. Geneva, Switzerland: WHO; 2006.
- [Google Scholar]
- WHO DPR Korea. World Health Day 2007. Towards the elimination of malaria in the Korean peninsula. Available from: http://www.dprk.searo.who.int/EN/Section1_25.htm, accessed on March 20, 2009
- Effect of permethrin impregnated bed nets in reducing population of malaria vector Anopheles culicifacies in a tribal village of Orissa state (India) Indian J Med Res. 1989;93:371-8.
- [Google Scholar]
- Lambdacyhalothrin treated bed nets as an alternative method of malaria control in tribal villages of Koraput District, Orissa State, India. South East Asian J Trop Med Public Health. 1993;24:513-21.
- [Google Scholar]
- Deltamethrin impregnated bednets against Anopheles minimus transmitted malaria in Assam, India. J Trop Med Hyg. 1995;98:73-83.
- [Google Scholar]
- Evaluation of lambdacyhalothrin-impregnated bednets in a malaria endemic area of India. Part 3. Effects on malaria incidence and clinical measures. J Am Mosq Control Assoc. 1998;14:444-50.
- [Google Scholar]
- Impact of alphacypermethrin treated bed nets on malaria in villages of Malkangiri district, Orissa, India. Acta Trop. 2003;89:55-66.
- [Google Scholar]




