Translate this page into:
Impact of referral transport system on institutional deliveries in Haryana, India
Reprint requests: Dr Shankar Prinja, Assistant Professor of Health Economics, School of Public Health Postgraduate Institute of Medical Education & Research, Chandigarh 160 012, India e-mail: shankarprinja@gmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Creation of a strong referral transport network across the country is necessary for improving physical access to public sector health facilities. In this study we evaluated the referral transport services in Haryana, i.e. Haryana Swasthya Vaahan Sewa (HSVS), now known as National Ambulance Service (NAS), to assess the extent and pattern of utilization, and to ascertain its effect on public sector institutional deliveries.
Methods:
Secondary data on 116,562 patients transported during April to July 2011 in Haryana state were analysed to assess extent and pattern of NAS utilization. Exit interviews were conducted with 270 consecutively selected users and non- users of referral services respectively in Ambala (High NAS utilization), Hisar (medium utilization) and Narnaul (low utilization) districts. Month-wise data on institutional deliveries in public facilities during 2005-2012 were collected in these three districts, and analysed using interrupted time series analysis to assess the impact of NAS on institutional deliveries.
Results:
Female gender (OR = 77.7), rural place of residence (OR = 5.96) and poor socio-economic status (poorest wealth quintile OR = 2.64) were significantly associated with NAS ambulance service usage. Institutional deliveries in Haryana rose significantly after the introduction of NAS service in Ambala (OR=137.4, 95% CI=22.4-252.4) and Hisar (OR=215, 95% CI=88.5-341.3) districts. No significant increase was observed in Narnaul (OR=4.5, 95% CI= -137.4 to 146.4) district.
Interpretation & conclusions:
The findings of the present study showed a positive effect of referral transport service on increasing institutional deliveries. However, this needs to be backed up with adequate supply of basic and emergency obstetric care at hospitals and health centres.
Keywords
Ambulance
equity
health care utilisation
maternal and child health services
referral transport

India aims to bring down the maternal mortality ratio (MMR) to 109 per 100,000 live births by 20151. Similarly, it aims to reduce the infant and child mortality to 28 and 42 per 1,000 live births respectively1. However, the MMR remains at 178 per 100,000 live births, and it appears, that India will not be able to meet its Millennium Development Goals2.
An analysis of the causes of maternal deaths in India found that nearly half of maternal deaths occurred where institutional care had not been availed at the time of delivery3. The distance from home to health facility was less than 5 km in 49 per cent of institutional deliveries, and as the distance increased number of women having institutional delivery decreased4. Among the reasons for not delivering in health facility, inadequate transport facilities (10.4%) and lack of adequate money (17.9%) featured as important reasons4. According to the District Level Household Survey 3, though 71 per cent of the villages in India had primary health centres within a 10 km distance but only 55.2 per cent had referral services for complicated delivery5. In summary, lack of physical as well as financial access for the natal care services is an important determinant for the use of institutional delivery in rural India.
Various demand-side and supply-side interventions have been initiated in India to improve the access to public sector health facilities for the poor and those living in remote rural areas67. Majority of these interventions aim to reduce barriers to financial access for health care services. But, evidence from National Family Health Survey 3 indicates that utilization of health services is not always a function of financial accessibility of a person7. Physical access and quality of services remain a key concern for improving utilization rates. Augmentation of physical infrastructure is being undertaken for reducing physical access barriers. Simultaneously nearly 20 models of ambulance service delivery have been implemented across the country8.
There is a significant variation in the scale, scope and mode of administration of these ambulance services in different States. While States like Andhra Pradesh and Assam have institutionalized a public private partnership administered Emergency Management and Research Institute (EMRI) at the state level9; Haryana Swasthya Vaahan Sewa (HSVS), now known as National Ambulance Service (NAS) was started in Haryana which is a government managed referral transport system with its administration decentralized to district level10.
We evaluated the referral transport system in Haryana to assess the extent and pattern of NAS utilization and its socio-demographic correlates. Secondly, we assessed whether NAS service has improved the utilization of public sector facilities for institutional deliveries.
Material & Methods
Background of Haryana Referral Transport Scheme (NAS): The NAS is a State wide public sector administered referral transport service in Haryana, India, which has been providing coverage in all 21 districts of the State since 2009. Free transportation services are provided to pregnant women, victims of road side accident, patients belonging to below poverty line households or notified slums, post natal cases in case of emergency till 6 weeks after delivery, neonates in case of emergency till 14 days after birth, freedom fighters and ex- servicemen. For the remaining patients, a user fee of  7/- per km is charged for provision of services. The service is provided for transporting the ill to a public sector health facility, or from a public sector facility to a higher referral centre, or back home after discharge.
7/- per km is charged for provision of services. The service is provided for transporting the ill to a public sector health facility, or from a public sector facility to a higher referral centre, or back home after discharge.
The service management is decentralized to the district level, with establishment of a call centre at the district hospital. Ambulances are stationed at different health facilities in the district, including district hospital, community health centres and primary health centres. A toll-free number ‘102’ is used by the beneficiaries to call an ambulance for referral and the same is then dispatched from the nearest available station point. Choice of the nearest health facility lies with the call centre operator for the first place of treatment and the attending physician for the referral. Service is limited for transportation to public sector institutions only.
Study area: Haryana State contributes to almost 2 per cent of the total population and 1.37 per cent of total geographical area in India. It had a Human Development Index (HDI) of 0.545 for the year 201111. The State has an infant mortality rate (IMR) of 42 per 1000 and MMR of 146 per 100,000 both of which are closer to or lower than national average of 42, and 178 respectively212. Three districts of Haryana, namely Ambala, Narnaul and Hisar were selected in consultation with the State Government officials, based on call rates per month and other routine performance statistics. Selection was made in a way to have representation of districts having high, medium and low degree of utilization of ambulance services by communities, besides a wider geographic representation within the State. In an analysis of more than 5700 randomly selected women who delivered during the year 2011-2012, it was reported that the proportion of pregnant women who availed HSVS service for delivering in a public sector institution was 47 per cent in Ambala, 39 per cent in Hisar and 25 per cent in Narnaul12. Thus, the three districts of Ambala, Hisar and Narnaul represented high, medium and low utilization districts respectively of NAS for maternal health service utilization. The institutional delivery rate as per DLHS 3 was 56.8 per cent in Narnaul, as compared to 48.6 per cent in Hisar and 55.4 per cent in Ambala5.
Data collection and analysis: To evaluate the NAS services and to assess its impact on utilization, primary as well as secondary data belonging to different time intervals and different sources were collected and analysed (Table I).
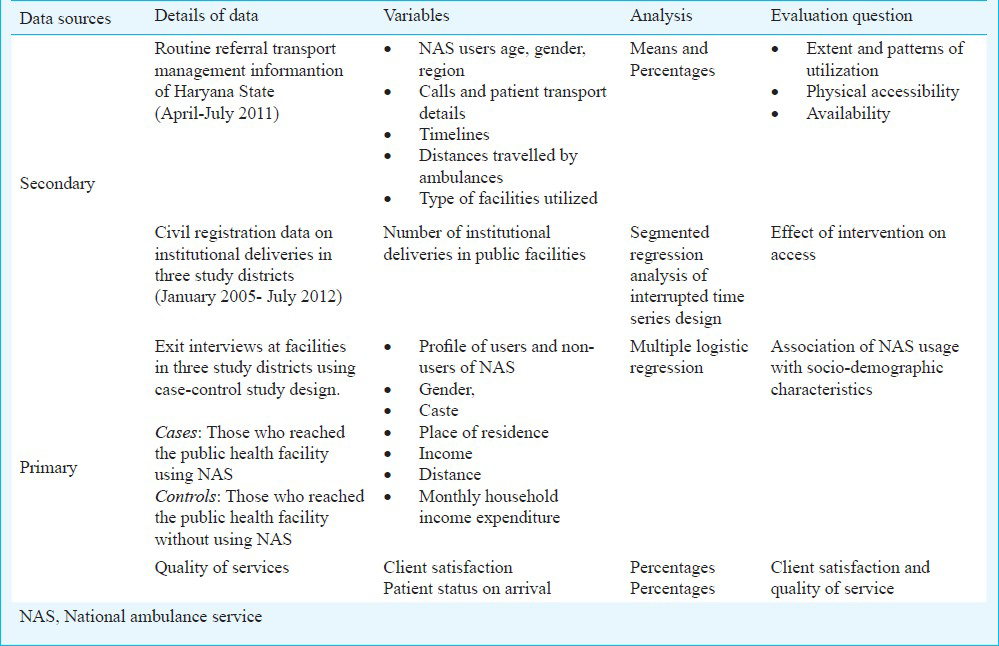
Extent and pattern of service utilization: To assess the extent and pattern of utilization of NAS services, the secondary data on utilization of ambulance services from April to July 2011 were analyzed. This comprised a data on 116,562 utilization episodes from all the 21 districts in Haryana, analysed to ascertain the extent of utilization in different districts which was estimated as the number of patients transported per 100,000 population. Pattern of utilization was assessed according to characteristics of users i.e. age, gender, caste, income and area of residence of the patients; time of the day, type of health facilities used and distance travelled to arrive at the health facility. The secondary data were also used to assess the quality of services in terms of time taken to reach the site of emergency and time taken to transport the patient to hospital.
Association of ambulance service usage with individual socio-demographic characteristics: To explore the association of utilization of NAS service with indivisual socio-demographic characteristics, case control design was used. Primary data were collected from one district hospital, one randomly selected community health centre (CHC) and one randomly selected primary health centre (PHC) in each of the three study districts in September 2011. All the patients admitted in the emergency department and maternity ward during the period of data collection were consecutively recruited and interviewed. Overall, 270 patients who had utilized the ambulance service and 270 patients who had not utilized the state run NAS service for travelling to the same health facility were interviewed. The sample of patients recruited from different institutions, i.e. PHC, CHC and district hospital was estimated using probability proportional to size, with number of patients being recruited in proportion to the patients treated in respective category of institutions in the district. Hence our sample was representative of the patients being treated in public sector institutions in these districts. In order to address selection bias at interviewer level consecutive sampling was used, wherein every emergency admission in health facility was contacted. Multiple logistic regression analysis was used to jointly examine the influence different independent variables (i.e. gender, caste, place of residence, income and distance) had on NAS service usage.
Effect of referral transport on utilization of public health facilities for institutional deliveries: For conducting this analysis, month-wise longitudinal data from 2005 till July 2012 were collected for institutional deliveries in public facilities in the three study districts. Monthly data were collected to avoid any secular trends. This allowed us to adopt a quasi-experimental design comparing institutional deliveries in districts with different degrees of NAS service utilization. To assess improvement in utilization of public health facilities for institutional deliveries, interrupted time series analysis was conducted using segmented linear regression13. First-order autocorrelation was tested statistically by using the Durbin-Watson statistic, and higher-order autocorrelations were investigated by using the autocorrelation and partial autocorrelation functions14. The best-fitting pre- and post-intervention lines were estimated by using linear regression. The coefficients and 95 per cent CI for ‘intervention’ represented the impact of NAS on institutional deliveries, while the pre- and post- represented trend of institutional deliveries in pre- and post-intervention periods respectively. Difference in the pre and post-slope represented the rate of change.
The study protocol was approved by the Institute Ethics Committee of Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh. Written informed consent were obtained both for secondary data collection (from authorities concerned) and for primary data collection (from the patients or their attendants for the interviews).
Results
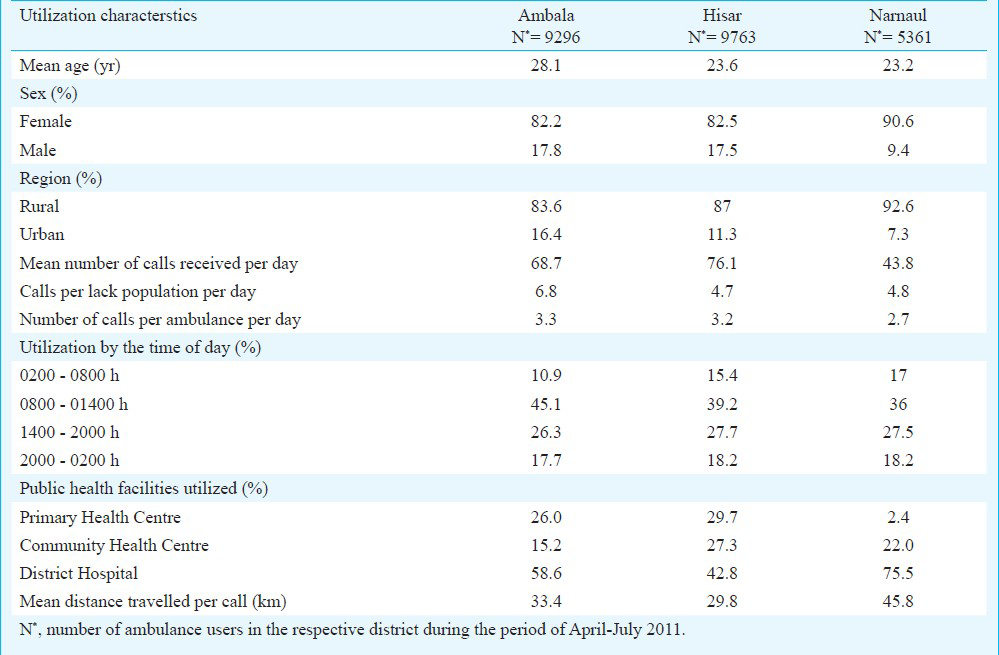
Extent of utilization: During April-July 2011, average number of calls received per day was highest in Hisar (76.1) followed by Ambala (68.7) and Narnaul (43.8) (Table II). It was found that since the time a call was made, the NAS ambulance took 18.8 min to reach the site of emergency and 21.7 min to transport the patient to the hospital from site of emergency. In nearly 90 per cent of the cases, NAS ambulance reached the site of emergency within 30 min of call while in 80 per cent of the cases the patient reached hospital within 1 hour of call (Fig. 1).
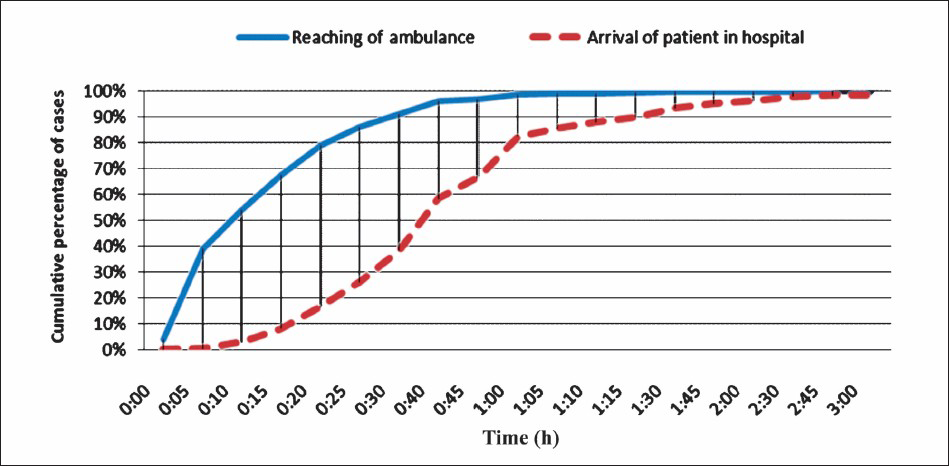
- Timeliness of NAS service in Haryana State, April- July, 2011.
Pattern of utilization: Most of NAS users were in the age group of 15-59 yr (94%), women (88.3%) and residents of rural areas (86.2%). No differences were observed in demographic characteristics of users among the three districts. The ambulance service was being used mostly during the morning hours between 0800 - 1400 h (45%) and by pregnant women (75.9%) (Table II).
District hospitals received maximum number of NAS users (53%). Mean distance travelled by ambulances per call in the State was 35.0 km with highest distances being covered in Narnaul district (Table II). Among the 270 NAS users interviewed, 63 per cent felt ‘satisfied’ from the services provided, 35.9 per cent were ‘very satisfied’ while only 1.1 per cent reported to be ‘somewhat satisfied’ with the services being provided.
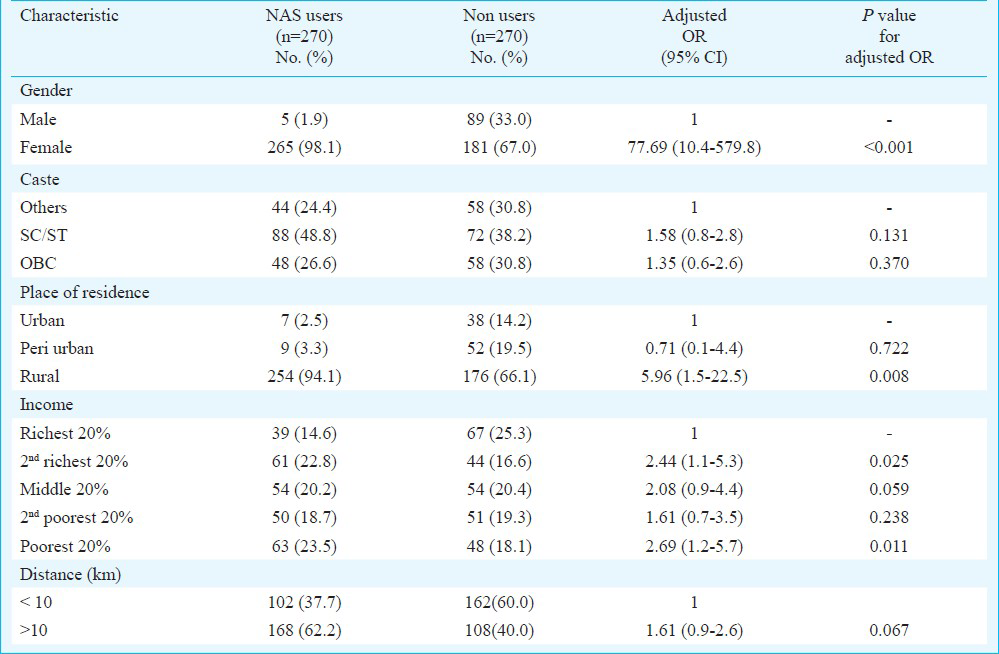
Association of NAS usage with socio-demographic characteristics: Female gender (OR = 77.7), rural place of residence (OR = 5.96) and income (poorest wealth quintile OR = 2.6) were significantly associated with NAS ambulance service usage (Table III). Among the hospitalized patients who used NAS, those belonging to poorest quintile were 1.6 times higher than richest quintile. On the contrary, among those who reached the hospital using non-HSVS modes of transport, richest quintile patients were 1.4 times higher than the poorest 20 per cent.
Impact of NAS on public sector institutional deliveries: There was an increase in the number of institutional deliveries in public sector institutions in districts Ambala and Hisar after implementation of NAS in November 2009, while the increase was not as characteristic in Narnaul. While Janani Suraksha Yojna (JSY) and Delivery Hut schemes in Haryana were started in May and September 2005, respectively, a more marked increase in number of deliveries in public sector institutions happened only after introduction of NAS referral transport in 2009. Janani Shishu Suraksha Karyakram (JSSK), a scheme for free institutional delivery, was introduced in July 2011. This could have supplemented the effect of NAS in later period.
In our interrupted time series analysis, it was found that institutional deliveries in Haryana rose significantly after the introduction of HSVS service in Ambala (OR=137, 95% CI=22.4-252.4) and Hisar (OR=215, 95% CI=88.5-341.3) districts (Table IV). No significant increase was observed in Narnaul (OR=4.5, 95% CI= -137.4 to 146.4) district. Pre slope, which is representative of pre-HSVS period, showed increasing trend in monthly institutional deliveries in Ambala (OR=4.1), Hisar (OR=8.7) and Narnaul (OR=5.8). However, in the post-intervention period, while institutional deliveries increased (post-slope) further in districts Ambala (OR=7.7) and Hisar (OR=9.7) there was no significant change in Narnaul (OR= 3.9) (Table IV, Fig. 2).

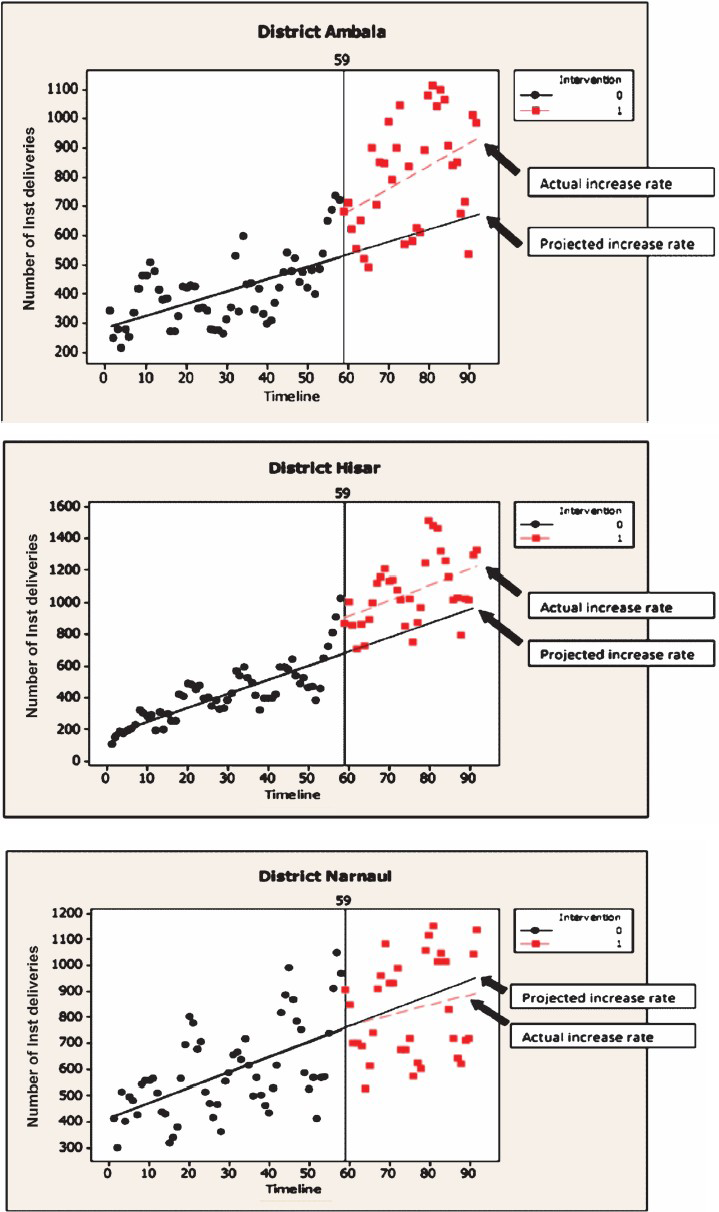
- Impact of referral transport service on public sector institutional deliveries in Haryana, 2005-2012. On X-axis numbers 0-90 indicate number of months from January 2005 onwards. 0, pre-intervention period; 1, post-intervention period.
Discussion
Overall, our study findings indicated that the districts where the NAS services were well utilized (i.e. Ambala and Hisar) a significant increase in institutional deliveries was associated with NAS introduction. Our results on impact of NAS on institutional deliveries could have been confounded by the presence of JSSK or other interventions aimed at promoting institutional deliveries. There are a number of design aspects of an interrupted-time series which can be incorporated to decide whether such confounding may be a possible explanation of an apparent intervention effect. One important design strategy to assess the plausibility of time dependent effects is to include a “no intervention” control series. In our study, it was not possible to include a no intervention scenario as the intervention was implemented in the entire State.
Hence, a quasi-experimental design was used. Ambala, Hisar and Narnaul represented high, medium and low utilization districts for NAS in regard to maternal health care. Our analysis showed that the NAS had a significant positive impact at increasing institutional deliveries in Ambala and Hisar, while there was statistically insignificant change in Narnaul. This dose-response relationship builds a stronger argument in favour of the role of referral transport in increasing institutional deliveries in Haryana. Further, the temporality of the increase in institutional deliveries also favours argument of positive effect of NAS on institutional deliveries
The reason why institutional deliveries did not increase in Narnaul after introduction of referral transport could be manifold. It could be that the referral transport was not adequately utilized or that the obstetric services were not adequately available or accessible in public health facilities or both. Another report, also showed that the utilization of referral transport was least in Narnaul among the three districts12. This survey also reported that the awareness of the 102 ambulance was low in Narnaul. There is also on evidence which points towards lesser number of gynaecologists per 1000 population in Narnaul (Phogat A, personnel communication, 2013).
Average number of trips per ambulance per day was found to be 8.1 in Andhra Pradesh, 4.31 in Gujarat, 1.14 in Rajasthan as against 2.8 in Haryana. However, pregnancy related cases as percentage total patients transported to institutions constituted 36 per cent in Haryana state as against 21 per cent in Andhra Pradesh, 33.7 per cent in Gujarat and 20.1 per cent in Rajasthan9. EMRI operational in different States across India, is providing services under public private partnership claims to reach site of emergency within 15 min and the patient is reached to professional medical help within an average of 35 min as compared to 18.9 and 21.7 min respectively taken by NAS service15. The cost of operating EMRI is quite high and variable ( 19-189)9 whereas the net cost of operating NAS service has been reported to range from 12.4 to 15.3 per km17. This study reported that the average technical efficiency of the NAS model of referral transport services was 76.8 per cent, with about 91 per cent ambulances operating at an efficiency level of more than 60 per cent, while 39 per cent operated at a level of more than 80 per cent efficiency.
A limitation of the present study was routinely recorded secondary data for analyzing the system performance, which has often been found to have problem of incompleteness and inaccuracy17. However, the variables analyzed were found to have been recorded in the database for more than 90 per cent of utilization episodes (age, gender, region, time lines, mean distance travelled per call). Data were relatively more incomplete for variables such as Kilometres as per Geographical Positioning System, which was not studied using the secondary data.
Another limitation of our study was the selection of cases and controls from health facilities. A community based survey would have been ideal for determining the rates of utilization of hospital services among the population sub-groups, based on income, caste, gender and area of residence. However, in view of limited resources, we selected our cases and controls from the health facilities. While it has the risk of missing the number of individuals who did not utilize health service at all, we believe that any distributional differences in hospital service utilization among population sub-groups between the cases (NAS users) and controls (non-users of NAS) can be interpreted in terms of being associated with the use of referral transport.
To conclude, our findings suggested a positive effect of referral transport service on utilization of institutional deliveries. This lends support to the argument that bridging the gaps in physical access through provision of a referral transport system can lead to positive outcomes in health system.
Acknowledgment
Authors acknowledge National Health Systems Resource Centre (NHSRC), New Delhi, India for funding the study, and thank Drs Rakesh Gupta, and T. Sundararaman for contributing to study design, Drs. Amit Phogat, Satish Aggarwal, J.S. Grewal and Yadav for assistance in collection of data.
References
- Maternal & child mortality and total fertility rates: Sample Registration System (SRS) New Delhi: Office of Registrar General, India; 2011.
- [Google Scholar]
- Special Bulletin on Maternal mortality in India 2010-12. New Delhi: Office of Registrar General, India, Ministry of Home Affairs, Goverment of India; 2013.
- [Google Scholar]
- Maternal and perinatal death inquiry and response project implementation review in India. J Obstet Gynecol India. 2013;63:101-7.
- [Google Scholar]
- UNICEF. Coverage evaluation survey. In: National fact sheet. New Delhi: UNICEF; 2009.
- [Google Scholar]
- District level household and facility survey. (DLHS-3), 2007-2008, India. Mumbai: IIPS and ORC Macro; 2010.
- [Google Scholar]
- High Level Expert Group Report on Universal Health Coverage for India. New Delhi: Planning Commission of India; 2011.
- [Google Scholar]
- Demand side financing in Health: How far can it address the issue of low utilization in developing countries? Health systems financing: the path to universal coverage. In: World Health Report 2010. In: Background Paper No. 27. Geneva: World Health Organization; 2010.
- [Google Scholar]
- Directory of innovations implemented in the health sector: December 2008 (first draft) New Delhi: MoHFW and Department for International Development; 2009.
- [Google Scholar]
- NHSRC. Study of emergency response service - EMRI model. New Delhi: National Health Systems Resource Centre; 2009. p. :47.
- [Google Scholar]
- Neonatal, postneonatal, childhood, and under-5 mortality for 187 countries, 1970-2010: a systematic analysis of progress towards Millennium Development Goal 4. Lancet. 2010;375:1988-2008.
- [Google Scholar]
- Inequality-adjusted Human Development Index for India's States: 2011. New Delhi: United Nations Development Programme; 2011.
- [Google Scholar]
- Concurrent evaluation of National Rural Health Mission, Haryana. In: 1st Biennial Report. Chandigarh: School of Public Health, Postgraduate Institute of Medical Education and Research (PGIMER); 2013.
- [Google Scholar]
- How to do (or not to do) … Assessing the impact of a policy change with routine longitudinal data. Health Policy Plan. 2012;27:76-83.
- [Google Scholar]
- Detecting autocorrelation. In: Basic econometrics (4th ed). New york: McGraw-Hill; 2003. p. :462-74.
- [Google Scholar]
- Transforming Government – eGovernment initiatives in India. Hyderabad: The ICFAI University Press; 2009.
- [Google Scholar]
- Cost & efficiency evaluation of a publicly financed and publicly delivered referral transport service model in three districts of Haryana state, India. Indian J Med Res. 2013;138:1003-11.
- [Google Scholar]
- A framework for evaluation of secondary data sources for epidemiological research. Int J Epidemiol. 1996;25:435-42.
- [Google Scholar]




