
Translate this page into:
Years of potential life lost due to cancer in Kamrup Urban District of Assam, northeast India
*For correspondence: manojkalita5354@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Despite sophistication in diagnosis and advances in treatment, cancer continues to be a major public health problem as well as a major cause of premature death across worldwide12. In 2012, there were an estimated 8.2 million deaths from cancer in the world: 4.7 million (57%) in males and 3.5 million (43%) in females. The world age-standardized mortality rate shows that there are 126 cancer deaths for every 100,000 men in the world and 83 deaths every 100,000 females3. However, an estimated 600,000-700,000 deaths in India were caused by cancer in 20124. In India, the highest incidence and mortality rate of cancer were seen in the north-eastern part of the country5. Some of the specific types of cancer have the highest incidence and mortality in these regions as compared to the national (India) and global scenario, particularly cancers of the gall bladder, stomach cancer, oesophageal cancers, mouth cancer and hypopharyngeal cancer56. Aizwal district of North-east India had the highest rate of mortality in India in men (140.6/100,000) and women (83.2/100,000)7. In Kamrup urban district, 70/100,000 men and 41.2/100,000 women died due to cancer7.
The number and rates of deaths alone do not reflect the complete burden imposed on the society, as some cancers harm younger people more than others. The number of years of life lost (YLL) therefore, depends on the age at death and the number of deaths at each age, and may resolve some of the mismatches of disease impact derived from death numbers alone. YLL data may be more useful in resource allocation and design of prevention programmes8910.
Data from the Population Based Guwahati (Kamrup Urban District) Cancer Registry57 for the 5-year period 2010 to 2014 were used to calculate YLL. Simple percentage mortality expressed the number of deaths from an individual tumour type divided by the total number of deaths from cancer as a percentage. The aim of the study was to quantify the total and YLL due to cancer in Kamrup urban district between 2010 and 2014.
Estimates of the YLL due to cancer are generated by comparing the life expectancy at five years of age interval with the number of deaths from cancer that occurred at that age group. The projected level of the expectation of life at birth for 2010-2015 for Assam State was calculated as 63.6 yr for males and 64.8 yr for females11. In Kamrup urban district, a total of 2259 deaths (males=1474, females=785) had occurred due to cancer in the last five years (2010-2014). On an average, about 452 deaths due to cancer were recorded per year, of which 295 were male deaths and 157 were female deaths. The age distribution of deaths among men and women is shown in the Figure. The probability of death increased with advancing age and was higher among older age group. Nearly 82.6 per cent (1218/1474) and 70.6 per cent (554/785) of deaths among men and women, respectively, occurred in the population in the age group of 50 yr and above.
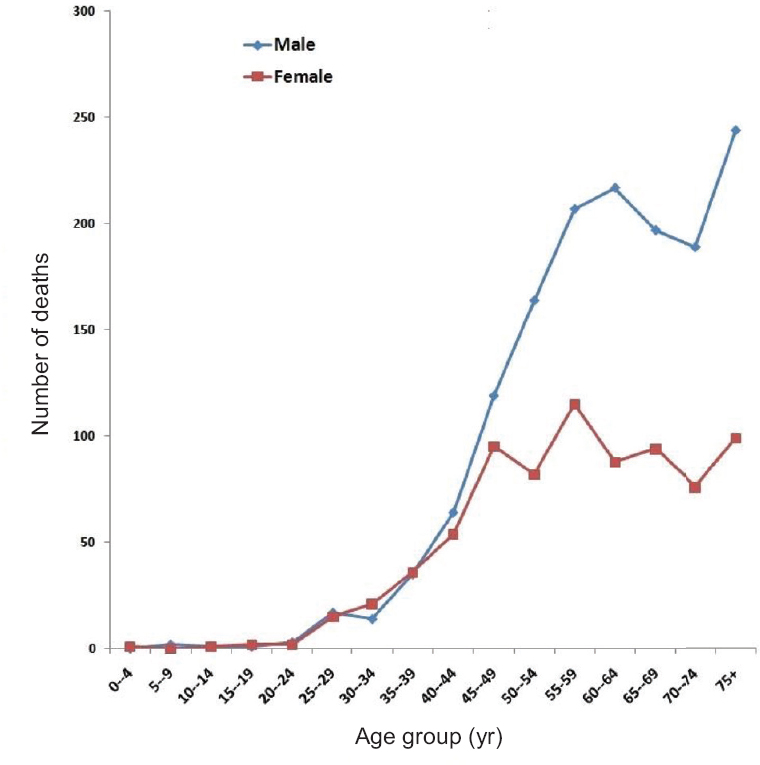
- Total number of cancer-caused deaths in Kamrup urban district in 2010-2014 according to age group.
Oesophageal cancer was the leading cause of cancer death in both sexes; 15.6 per cent of cancer deaths in men and 11.6 per cent in women during 2010-2014. Lung cancer was the second leading cause of death among men (11.5% of all cancers) of Kamrup urban district and, among women, gallbladder cancer was the second leading cause of death comprising 11.5 per cent of the total deaths due to cancer. Deaths from oesophageal, stomach, lung, gallbladder, breast and ovary cancers combined contributed almost half of all deaths from cancer during this period.
Oesophageal cancer was the sixth leading cause of cancer death worldwide12. A substantial number of years of life were lost or affected by oesophageal cancer worldwide, with the burden resting disproportionately on less developed countries. Geographically, the greatest burden is in the eastern part of Asia13. Oesophageal cancer was the top most killer among men in Kamrup urban district in terms of total YLL and mortality percentage. A total of 1567.4 and 581.2 life years were lost due to oesophageal cancer death among men and women, respectively, in 2010-2014.
The YLL for an individual cancer site can be expressed as a percentage of the total YLL from all cancers, so it can be directly compared with percentage mortality. Based on the total number of deaths at each age level, multiplied by the expected remaining years of life on each level, a total of 9305.4 YLL was estimated for men and 7668.6 for women who died from cancer between 2010 and 2014 (Table). The greatest percentage of YLL in men was due to oesophageal cancer, contributing a total of 16.8 per cent followed by hypopharyngeal cancer (7.8%) and lung cancer (7.4%). Among women, the greatest percentage of YLL was from breast cancer, comprising a total of 12.1 per cent followed by ovarian cancer (11.3%) (Table).
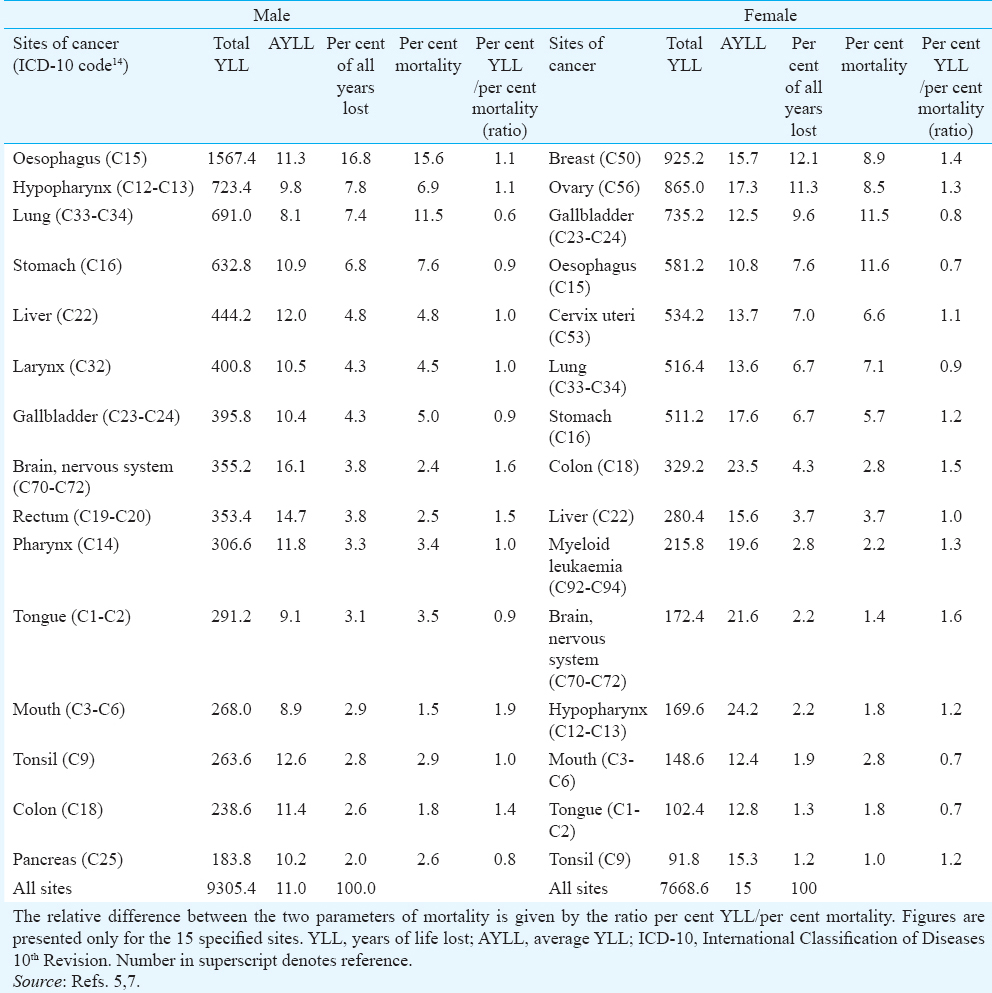
The average YLL (AYLL) is simply an average derived by dividing YLL by the actual number of deaths for each cancer site, over the defined time period. Effectively it shows, on an average, how much a patient's life is likely to be shortened by his/her cancer. The variation in cancer burden per affected patient varied dramatically according to tumour type. The mean AYLL amounted to 11.0 yr in men and 15.0 in women, indicating the numerical average of the life shortening from cancer (Table). Deaths among female-specific cancers such as cervical, breast, ovarian and uterine cancers occurred in lower ages than the male-specific or predominant cancers such as prostate, bladder and oesophageal cancers, contributing to a higher AYLL in females than in males. Among the top 10 sites, brain and central nervous system (CNS) cancers in males had the highest average number of AYLL per death (16.1 yr) followed by rectum (14.7 yr). Among females, the highest AYLL was due to hypopharyngeal cancer (24.2 yr) followed by carcinoma of colon (23.5 yr).
In Kamrup urban district, the female population had a lower YLL, but lost more years on average (higher AYLL) by cancer type, largely because of the age at onset of particular type of cancer and longer life expectancy of women. Breast and cervical cancers were important contributors to female cancer mortality. A sustainable portion of these deaths can be prevented only by improving early detection and treatment methods of breast and cervical cancer.
Among men highest AYLL was due to brain and nervous system cancer (16.1 yr); this was probably due to CNS cancer occurring at early years of life. Among women on average 24.2 life years were lost due to hypopharyngeal cancer. Kamrup urban district recorded a significantly increasing trend of prostate cancer incidence rates over time from 2003 onwards and it was the sixth leading site among men in Kamrup urban district13. Despite a high prostate cancer incidence in Kamrup urban district, the AYLL due to prostate cancer were relatively low compared to other cancer types; this could be attributed to the advanced age at diagnosis.
Cancer is a major and increasing cause of premature deaths, and YLL may be a more accurate measure than number of deaths. AYLL measures the burden to individual patients and may be helpful where individuals’ needs are relevant, such as palliative care. The high AYLL illustrate the poor prognosis. Primary prevention, early detection, adequate and timely treatment are needed to change this situation, particularly in Kamrup urban district, Assam.
Acknowledgment
Authors thank Dr P. Mathur and his team for providing guidance and valuable information for this manuscript and acknowledge the cooperation from all the sources of registration and oncologists of Dr. B. Borooah Cancer Institute, Guwahati, India.
Financial support & sponsorship: Authors sincerely acknowledge the National Cancer Registry Programme (NCRP), National Centre of Disease Informatics and Research (NCDIR), Indian Council of Medical Research (ICMR), and Department of Health Research, Government of India, for funding Population Based Cancer Registry-Guwahati, vide letter No. NCDIR/COU/NE/433/2009.
Conflicts of Interest: None.
References
- Years of life lost (YLL) from cancer is an important measure of population burden - And should be considered when allocating research funds. Br J Cancer. 2005;92:241-5.
- [Google Scholar]
- Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893-917.
- [Google Scholar]
- GLOBOCAN 2012 v10. 2013. Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11. Lyon: International Agency for Research on Cancer; Available from: http//www.globocan.iarc.fr
- [Google Scholar]
- The growing burden of cancer in India: Epidemiology and social context. Lancet Oncol. 2014;15:e205-12.
- [Google Scholar]
- Three Year Report of the Population Based Cancer Registries: 2009-2011. 2013. Available from: http://www.ncrpindia.org
- [Google Scholar]
- A way forward to address the cancer burden in North-East India. Int J Health Allied Sci. 2016;5:61-2.
- [Google Scholar]
- Three Year Report of the Population Based Cancer Registries: 2012-2014. 2016. Available from: http://www.ncrpindia.org
- [Google Scholar]
- The global burden of cancer: Priorities for prevention. Carcinogenesis. 2010;31:100-10.
- [Google Scholar]
- A comparison of cancer burden and research spending reveals discrepancies in the distribution of research funding. BMC Public Health. 2012;12:526.
- [Google Scholar]
- Population Projections for India and States 2001-2026, Report of the Technical Group on Population Projections Constituted by the National Commission on Population; May 2006. New Delhi: Office of Registrar General and Census Commissioner, India; 2001.
- [Google Scholar]
- High Resolution Microendoscopy for Early Detection of Esophageal Cancer in Low-Resource Settings (Conference Presentation) In: Suter MJ, Lam S, Brenner M, Tearney GJ, Wang TD, eds. Endoscopic Microscopy XI; and Optical Techniques in Pulmonary Medicine III. SPIE Bios 2016: Proceedings Volume 9691; 2016 February 13-18; San Francisco, USA. San Francisco: The International Society for Optics and Photonics; 2016.
- [Google Scholar]
- The global burden of esophageal cancer: A disability-adjusted life-year approach. World J Surg. 2016;40:395-401.
- [Google Scholar]
- ICD-10 Version:2016. Available from: http://apps.who.int/classifications/icd10/browse/2016/en
- [Google Scholar]




