
Translate this page into:
Use of Family CAGE-AID questionnaire to screen the family members for diagnosis of substance dependence
Reprint requests: Dr Debasish Basu, Drug De-addiction & Treatment Centre, Department of Psychiatry, Postgraduate Institute of Medical Education & Research, Chandigarh 160 012, India e-mail: db_sm2002@yahoo.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
CAGE-AID questionnaire is a short, useful screening tool for substance dependence. Assessment of one family member for the screening of substance dependence in the family could be useful in clinical practice and research. In this study, we aimed to assess the validity of the Family CAGE-AID questionnaire for the diagnosis of substance dependence.
Methods:
Cross-sectional assessments using CAGE-AID and Family CAGE-AID questionnaires were conducted both for the study participants (n = 210) and their family members. The participants were recruited from two different treatment settings: a treatment seeking population from a de-addiction centre, and non-treatment seekers for substance use disorders from the psychiatry outpatient department. ICD-10 criteria and subsequent detailed clinical interview by a trained psychiatrist were used for the final diagnosis of substance dependence.
Results:
In the psychiatry outpatient group, the scores on CAGE-AID and Family CAGE-AID questionnaires were significantly correlated with the ICD-10 symptom score (r=0.81 and 0.70, respectively). In the same group, inter-rater agreement of the Family CAGE-AID was good with CAGE-AID and moderate with ICD-10 diagnosis of substance dependence (Cohen's kappa 0.78 and 0.61, respectively). A cut-off score of three on Family CAGE-AID was found to be 95·8 per cent sensitive and 100 per cent specific.
Interpretation & conclusions:
Family CAGE-AID questionnaire is a valid screening instrument for the diagnosis of substance dependence, with acceptable sensitivity and specificity of a cut-off score of three. The simplicity and the brevity of such an instrument can be valuable in the clinical settings of developing countries and also for epidemiological studies.
Keywords
CAGE-AID
family
screening
substance use disorder
validity

Globally, substance use disorders have a high prevalence and constitute an important public health problem. Screening for these disorders is important in clinical practice and epidemiologic research. CAGE questionnaire, a brief and popular screening instrument, is an acronym for four questions: “Have you ever tried to Cut down your drinking; have people Annoyed you about your drinking; have you ever felt Guilty about your drinking; have you ever had a drink first thing in the morning to steady your nerves or to get rid of a hangover (Eye opener)?”1. CAGE has demonstrated high test-retest reliability and adequate correlations with other screening instruments, and is a valid tool for detecting alcohol abuse and dependence23456. It has also been used in other studies to screen for substance use disorders other than alcohol, Adapting the questions to Include other Drugs (CAGE-AID)7. In addition to determining the magnitude of problems due to substance use disorders, detection of misuse through opportunistic screening is important for prevention of related morbidity and mortality8. At an early stage of misuse, a simple intervention, such as a brief counselling session delivered by a primary care physician, has proven to be an effective treatment89.
In general, most patients with substance use disorders do not look like “typical alcoholics” or “drug addicts” unless they are in an advanced stage and are difficult to treat. A clinician must inquire about symptoms and sometimes must press the patient who seems evasive about answering questions about substance abuse. Classic denial is an unconscious mechanism that could underlie the “ever annoyed by criticism of your drinking” question. The drinking problem is often obvious to those around the drinker but may be practically invisible to the drinker1011. Hence assessment of the family members is expected to overcome this lacuna. This conjecture would be more appealing for the collectivist culture in a country like India. In contrast with the West, here most of the patients live with their family, which is almost inseparable from the individual, considering managing patients especially those with mental illness12. Two cross-cultural studies conducted in late nineties based on psychiatrically ill patients have shown that 98.3 per cent of the patients live with their families in India compared to 50 per cent of the patients in the western world1314. In India, there is cooperation and involvement of the family members in the treatment decision, career choice and marriage of patients15.
In this context, it would be worthwhile to examine whether the Family CAGE questionnaire, adapted from the original CAGE questionnaire1 by Frank et al16 and further adapted by us by amalgamating it with CAGE-AID questionnaire developed by Brown et al17 to include other drugs thus yielding the Family CAGE-AID, can be used to screen the non-substance using family members. Though the validity of Family CAGE instrument regarding family stress, coping and treatment seeking has been examined in non-alcohol using members of the family16, its role in the diagnosis of substance dependence is still to be investigated. Brown18 recommended to examine the validity of Family CAGE questionnaire against a more direct measure like alcohol dependence.
This study was aimed to examine the validity and the predictive characteristics of Family CAGE-AID questionnaire for the diagnosis of alcohol and other substance dependence. Two different subgroups of participants along with their family members were screened to accomplish the objective.
Material & Methods
The study was conducted in the Psychiatry department of Postgraduate Institute of Medical Education and Research, a tertiary-care hospital in Chandigarh, India. Two groups of participants were included. One group consisted of individuals recruited from the patient population attending the Drug De-addiction and Treatment Centre (DDTC) (the DDTC group). The patients attending DDTC primarily seek help for substance use disorders and may or may not have a co-morbid psychiatric diagnosis. They may be self-referred or brought by family members. This group represented the treatment seeking subset and the number of individuals assessed was 109. Another group was drawn from the Psychiatry outpatient services (Psychiatry OPD group). It had patients primarily seeking help for psychiatric problems but might have co-morbid substance use problems. First, they were enquired about their history of substance use. If, the response was positive for substance use they were approached for the purpose of the study. There were 101 participants in this subset of population. Family members of both these treatment groups (one family member per participant) were interviewed. They were required to be in ‘reasonable contact’ with the participant and over 16 yr of age. Reasonable contact was defined as face-to-face contact at least twice per week19. At both the set ups (DDTC and psychiatry OPD) patients and accompanying persons were interviewed. Overall, 210 participants and equal number of their caregivers were examined for the purpose of the study.
Assessment tools: The following instruments were administered for the purpose of the study:
-
Semi-structured forms for socio-demographic and clinical profile: This had emphasis on assessment of family history of substance use and living arrangement of the family.
-
Diagnosis of substance disorder was confirmed on the ICD-10 Checklist- Psychoactive Substance Use Syndromes Module20. This is used to determine a diagnosis of substance dependence based on a cut-off of satisfying at least three or more criteria. But final diagnosis was made on clinical interview by a qualified psychiatrist.
-
CAGE-AID Questionnaire7: The original CAGE questionnaire1 expanded to apply for substances in addition to alcohol (CAGE-Adapted to Include Drugs). It has sufficient criterion validity and has been used in different settings717.
-
Family CAGE-AID Questionnaire: It has the same four questions as the CAGE-AID questionnaire and is administered to family members for screening of alcohol (and other substance) disorders. The Family CAGE questionnaire has strong internal consistency reliability, with Cronbach's alpha coefficients of 0.84 to 0.8916. This questionnaire was modified to include substances in addition to alcohol.
Both the above questionnaires were translated into the local language Hindi and back translated by two different individuals (fluent in Hindi and English) to yield the closest possible meaning.
Procedure: To examine the validity of Family CAGE-AID questionnaire for the diagnosis of substance dependence, participants were recruited from two different sources. Those from the de-addiction centre represented the clinic attending population in whom the diagnosis of substance dependence was established. This group was expected to measure the sensitivity of the instrument. On the contrary, those who were recruited from the psychiatry outpatient were representative of non-clinic attending population and this group in addition to other predictive characteristics was obtained to investigate the validity and the specificity of the instrument. Diagnosis of substance dependence was considered by ICD-10 symptom checklist and substantiated by clinical interview by a qualified psychiatrist. The validity of Family CAGE-AID questionnaire was measured by its concordance with ICD-10 diagnosis of substance dependence and the CAGE-AID questionnaire.
The data collection period was from April 1 to June 30, 2013. The participants were included in the study by convenience sampling. After obtaining written informed consent, assessment on semi-structured forms and questionnaires was carried out. Assessment on CAGE-AID questionnaire for the participants and Family CAGE-AID questionnaire for the family member was carried out separately. The questionnaires were on separate pages of the main form to prevent undue influence of one rater on to others while answering. Sometimes family members do not want to divulge information regarding substance user in the family mostly due to fear of violence or a possibility of disturbance in the equilibrium in the family. Likewise sometimes the substance user himself is not comfortable with the idea of his family discussing about his substance use problem with others. In our study, we took into account both the factors and had excluded subjects with even minimal reluctance. All questionnaires were administered by trained psychiatrists in a single sitting. Ethical Clearance of the study protocol was obtained from the Institute Ethics Committee.
Statistical analysis: Analysis was done separately for the two study subgroups. Frequency, mean and standard deviation were used to depict the socio-demographic characteristics of the study participants. Similar statistical analysis was done for the relevant clinical variables. Pearson's correlation was applied to find out the association between the score in the Family CAGE-AID questionnaire with the CAGE-AID questionnaire and total score of the ICD-10 symptom checklist for substance dependence. The inter-rater agreement amongst Family CAGE-AID, CAGE-AID and diagnosis of substance dependence as per ICD-10 was calculated by Cohen's kappa. The predictive characteristics of the Family CAGE-AID for the diagnosis of substance dependence were derived from the analysis of sensitivity, specificity, positive and negative predictive values of the instrument. The predictive power of individual questions in the Family CAGE-AID questionnaire was measured by logistic regression.
Results
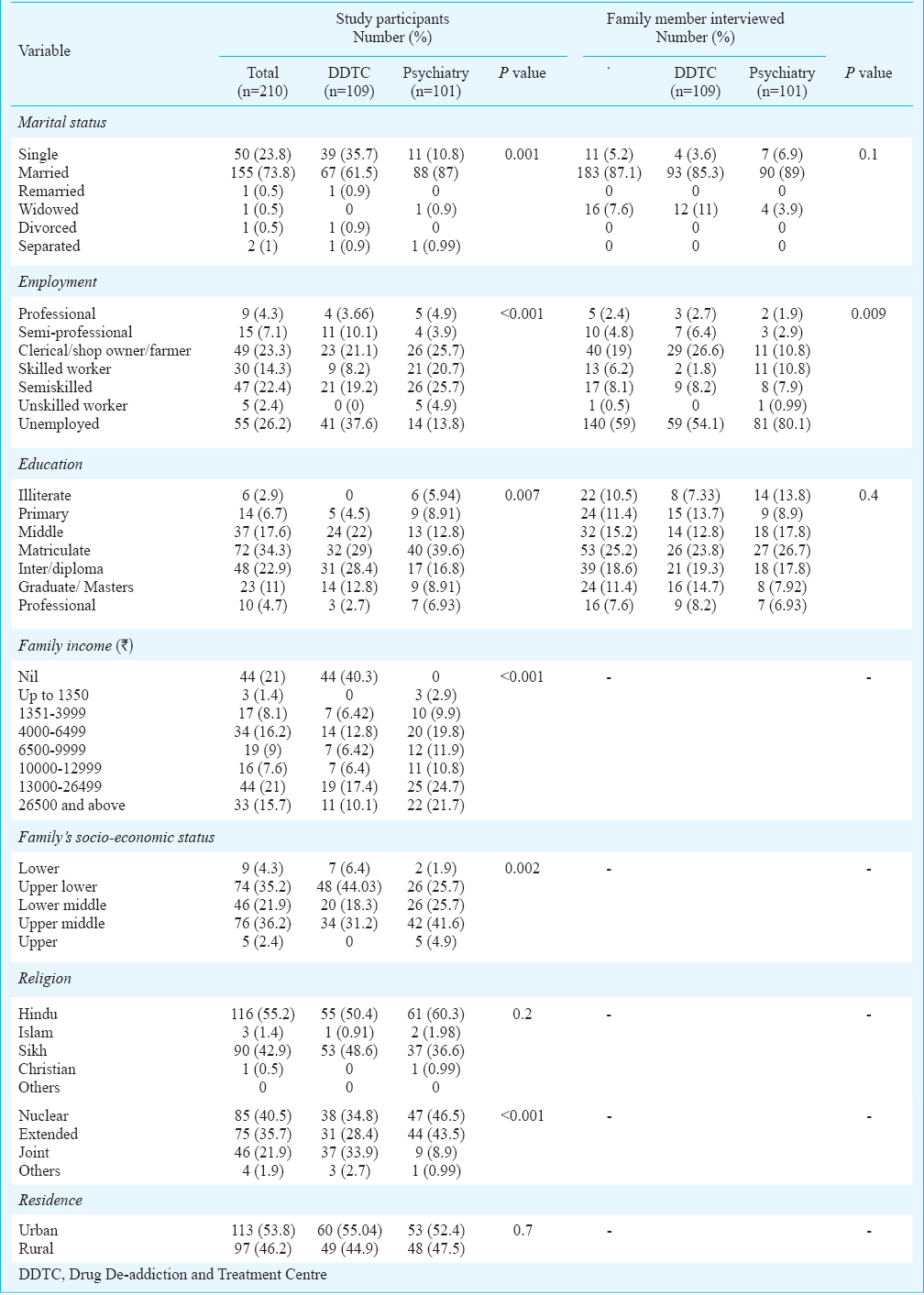
Socio-demographic and clinical variables: A total of two hundred ten substance users and their family members were examined. All of them were male. The mean age of the DDTC groups participants was 38.1 ± 13 yr. Most of them were married (73.8%) and about one fourth were unemployed. Around one third of them were educated up to high school. When compared both the groups were found to be significantly different with respect to their marital status, level of education, socio-economic status, type of family and occupation. The details are given in Table I.
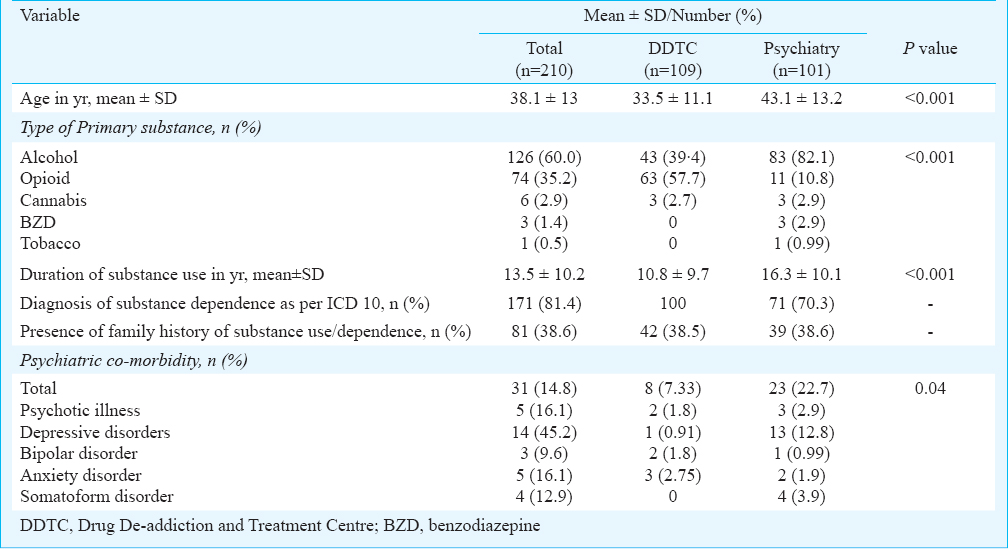
In the overall sample, 60 per cent were alcohol users and 35.2 per cent were opioid users. Opioid was over-represented (57.7%) in the DDTC group as opposed to the psychiatry OPD group where alcohol (82.1%) was the predominantly used substance. Mean duration of substance use was 13.5 ± 10.2 yr. Comparison of clinical variables also displayed significant difference in age, type of primary substance use, duration of use and occurrence of psychiatric disorders between the de-addiction and the psychiatry outpatient groups. (Table II).
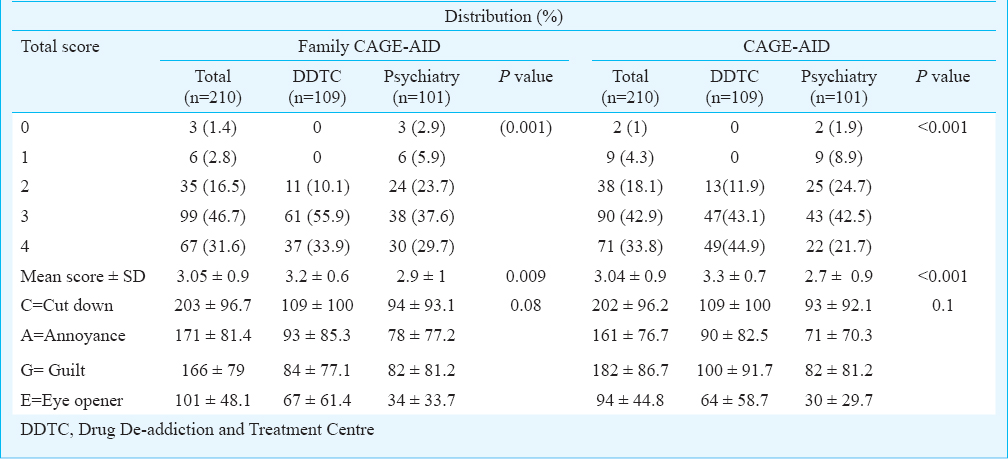
The Family CAGE-AID questionnaire: Most of the participants (78.3%) scored three or more in the Family CAGE-AID questionnaire. “Cut down on substance use” was the commonest (96.7%) agreed upon item followed by “Annoyed by complaints about substance use” (81.4%), “Guilty about substance use” (79%) and “Eye opener” (48.1%). The mean score of Family CAGE-AID questionnaire was 3.05 ± 0.9. Most of the participants in the de-addiction subgroup had scored three (55.9%) which was more than that of psychiatry outpatient (37.6%). With respect to the individual questions, both the subgroups had demonstrated a similar trend as mentioned in the overall sample. But the question on “Eye opener” received a substantially more positive response in the de-addiction subgroup (61.4 vs 33.7%). When the de-addiction and the psychiatric outpatient groups were compared, they were found to be significantly different with regard to the mean scores in both Family CAGE-AID and CAGE-AID questionnaire (Table III).
Significant correlation was observed between the scores of Family CAGE-AID questionnaire and number of criteria satisfied as per ICD-10 symptom score (r=0.70; P<0.0001) in the psychiatry sample. In the same group of subjects the total scores of CAGE-AID and the Family CAGE-AID were also significantly correlated (r=0.81; P<0.0001). Amongst the participants of the de-addiction subgroup, the correlation of the total scores of the Family-CAGE-AID questionnaire with the CAGE-AID questionnaire and the ICD-10 symptom score were 0.27 (P=0.004) and 0.02 (P=0.79), respectively.
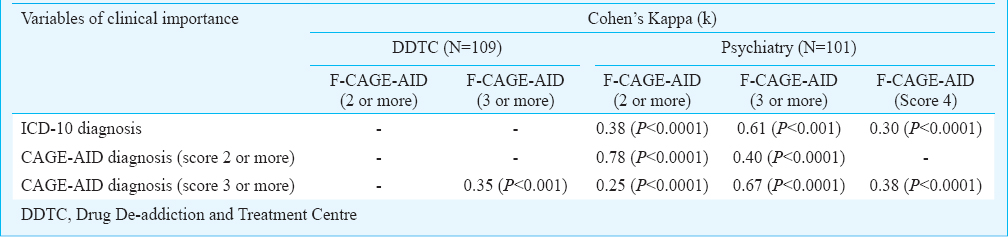
For the sample from psychiatry outpatient, Family CAGE-AID questionnaire was found to have a substantial inter-rater agreement with that of the same score of CAGE-AID questionnaire (Cohen's kappa 0.78 and 0.67 for cut-off two and three, respectively). In the same group, the inter-rater reliability of Family CAGE-AID questionnaire with ICD-10 diagnosis of substance dependence was found to be moderate (Cohen's kappa=0.61) when the cut-off of Family CAGE-AID was determined as three. As all the participants recruited from the DDTC group were substance dependent, inter-rater agreement could not be calculated. (Table IV).
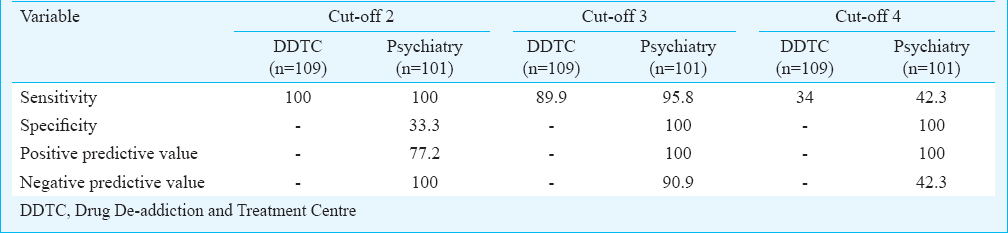
For the psychiatry OPD group, when the cut-off was kept as two, the sensitivity and specificity of Family CAGE-AID questionnaire were observed to be 100 and 33.3 per cent, respectively. On the other hand, a cut-off of three increased the specificity to 100 per cent but lowered the sensitivity to 95.8 per cent. As all the participants from de-addiction outpatient were substance dependent, only sensitivity could be measured which was found to be 100 and 89.9 per cent for Family CAGE-AID cut-off score of two and three, respectively. Thus, a cut-off score of three generated the best balance between sensitivity and specificity (Table V).
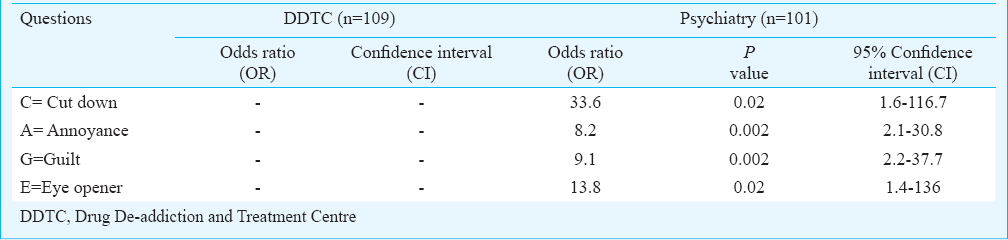
Logistic regression was run to find out whether the individual questions of Family CAGE-AID questionnaire could predict the diagnosis of substance dependence. This model of prediction was observed to be viable (Chi-square=76.8; P<0.001) and accounted for the 55 per cent (Nagelkerke R2=0.55) of overall variance. Amongst the four questions of the Family CAGE-AID questionnaire, the first one (“Cut down on substance use”) had the strongest association (OR=33.6; P=0.02) with the diagnosis of substance dependence. The association of the other three questions was also observed to be significant (Table VI).
Discussion
Majority of the study population were either alcohol or opioid users. This result was in accordance with the data obtained from the Drug abuse monitoring system (DAMS)21. In our sample, most of the individuals were brought to the de-addiction centre by their family members. This coincides with the usual trend and emphasizes the salience of the family members in the treatment of substance use22. The Family CAGE-AID questionnaire was correlated with the ICD-10 symptom score and with the traditional CAGE-AID questionnaire. There was a substantial inter-rater agreement between the Family CAGE-AID and the CAGE-AID questionnaire. The Family CAGE-AID questionnaire was also found to have a moderate inter-rater reliability with that of the ICD-10 diagnosis of substance dependence. These results demonstrated the validity of Family CAGE-AID questionnaire. The questionnaire with a cut-off criterion of two was also found to be 100 per cent sensitive for the diagnosis of substance dependence. When the cut-off was adjusted at three, the specificity and the positive predictive value (PPV) for the diagnosis reached 100 per cent though the sensitivity dropped to 95.8 per cent. All four questions of Family CAGE-AID predicted substance dependence, but the first question, “Tried to Cut down on substance use” was found to have the strongest association. This question reflects a scenario in which the amount of consumption has reached beyond such a level that the substance user himself or the families have exercised control.
Construct validity of the Family CAGE-AID questionnaire in alcohol problems was studied by Frank et al16. In that study, the Family CAGE-AID was strongly correlated with global assessment of family alcohol-related problems and predicting help-seeking behaviour. The Family CAGE-AID was also significantly correlated with a higher sick visit rate, more medications prescribed and lifetime history of major depression. But the concurrent validity of the questionnaire was not investigated. We measured and established the concurrent validity of the Family CAGE-AID questionnaire across the various substance use. With a lower threshold (cut-off 2) Family CAGE-AID was found to be highly sensitive and with higher threshold (cut-off 3) it was 100 per cent specific for the diagnosis of substance dependence. A study conducted in an adolescent mental health care centre has also demonstrated excellent diagnostic accuracy of CAGE-AID in predicting substance use disorders22. Our study has replicated similar findings in the adult population, extending the generalizability of the previous result. However, our figures were higher when compared to CAGE-AID questionnaire in which sensitivity and specificity ranged from 43 to 94 per cent and 70 to 97 per cent, respectively in primary care population17. In another meta-analysis, when compared to the Diagnostic and Statistical Manual IV (DSM IV) criteria the pooled sensitivity of CAGE-AID was found to be 87 per cent for inpatients, 71 per cent for the primary care patients and 60 per cent for the ambulatory patients5. So more severe is the substance abuse, more is the possibility of a positive screening in CAGE-AID questionnaire. As more than half of our study participants were recruited from a tertiary care de-addiction centre, they represented the more severe forms of substance use. This might explain the high predictive characteristics of the family CAGE-AID questionnaire. The high figures could well be explained by the source of information in the Family CAGE-AID thus averting the ‘denying’ and ‘evasive’ substance user.
Family CAGE-AID questionnaire was found to be a valid instrument for the diagnosis and screening of substance dependence. It could overcome the substance user related problems which could question the reliability of the responses of a direct questionnaire like CAGE-AID. Apart from diagnosis, screening for substance abuse could be followed by brief intervention which has a reasonable evidence especially for the primary care population. Such an instrument can also identify the non-attending family members and incorporate them in the treatment23. Numerous clinical trials have demonstrated the efficacy (and often superiority) of couple and family treatments for alcoholism and drug abuse and emphasized on a greater awareness of family members’ crucial roles in the aetiology, maintenance, and long-term course of substance use and addictive behaviour24.
The findings of the study are limited by its lack of generalizability. Though an attempt was made to include various spectrum of severity of substance dependence, the number of milder, non-treatment seeking subset was relatively less. Moreover, majority of our participants were either alcohol or opioid users resulting in questionable generalizability of this instrument across various other substances. The reliability of the translated version of Family CAGE-AID was not established a priori. Despite all efforts to make it absolutely sure to include only those individuals and their family members who were really willing to participate in the study, the possibility of denial or over-reporting could not be obviated completely. We have not assessed and excluded relatives with psychiatric co-morbidity, which might have influenced the response in the Family CAGE questionnaire. Finally, it can be argued that the 95% CI ranges were large for the predictive power of individual CAGE items. However, none of the lower bound of the CI values was less than 1, indicating that one can place confidence in the results of these estimates, though the standard error is large.
In conclusion, Family CAGE-AID questionnaire may be a utilitarian instrument for its potential in detecting substance dependence in community or epidemiological studies where the primary user may be unavailable or non-cooperative, or in clinical settings utilizing family members attending other facilities and services, especially in the socio-cultural context of our country. Future research is warranted to substantiate its validity in the general population.
Conflicts of Interest: None.
References
- The value of the CAGE in screening for alcohol abuse and alcohol dependence in general clinical populations: A diagnostic meta-analysis. J Clin Epidemiol. 2004;57:30-9.
- [Google Scholar]
- The Value of CAGE, CUGE, and AUDIT in screening for alcohol abuse and dependence among college freshmen. Alcohol Clin Exp Res. 2000;24:53-7.
- [Google Scholar]
- The CAGE Questionnaire: Validation of a new alcoholism screening instrument. Am J Psychiatry. 1974;131:1121-3.
- [Google Scholar]
- The CAGE questionnaire for alcohol misuse: a review of reliability and validity studies. Clin Invest Med. 2007;30:33-41.
- [Google Scholar]
- The prevalence and detection of substance use disorder among inpatients ages 18 to 49: an opportunity for prevention. Prev Med. 1998;27:101-10.
- [Google Scholar]
- Brief intervention in primary care settings. A primary treatment method for at-risk, problem, and dependent drinkers. Alcohol Res Health. 1999;23:129-7.
- [Google Scholar]
- Hazardous and harmful alcohol consumption in primary care. Arch Intern Med. 1999;159:1681-9.
- [Google Scholar]
- Preserve and strengthen family to promote mental health. Indian J Psychiatry. 2010;52:113-26.
- [Google Scholar]
- Characteristics of patients with schizophrenia in two cities in the US and India. Psychiatr Serv. 1996;47:300-1.
- [Google Scholar]
- Comparison of people with schizophrenia from Liverpool, England and Sakalwara, Bangalore, India. Int J Soc Psychiatry. 1998;44:225-30.
- [Google Scholar]
- Heitzman J, Worden RL, eds. India: A country study (2nd ed). Washington: Library of Congress; Washington DC Federal Research Div; 1995.
- Use of the Family CAGE in screening for alcohol problems in primary care. Arch Fam Med. 1992;1:209-16.
- [Google Scholar]
- Conjoint screening questionnaires for alcohol and other drug abuse: criterion validity in a primary care practice. Wis Med J. 1995;94:135-40.
- [Google Scholar]
- Family alcoholism screening- progress, pitfall, and promise. Arch Fam Med. 1992;1:219-21.
- [Google Scholar]
- Needs for care among the relatives of long-term users of day care. Psychol Med. 1989;19:725-36.
- [Google Scholar]
- World Health Organization (WHO). International statistical classification of diseases and related health problems, 10th Revision (ICD-10). Geneva: WHO; 1992.
- The extent, pattern and trends of drug abuse in India: National survey. New Delhi: United Nations Office on Drugs and Crime (UNODC) and Ministry of Social Justice and Empowerment, Government of India; 2004.
- Screening for substance abuse among adolescents: validity of the CAGE-AID in youth mental health care. Subst Use Misuse. 2009;44:823-34.
- [Google Scholar]
- Screening in brief intervention trials targeting excessive drinkers in general practice: systematic review and meta-analysis. BMJ. 2003;327:536-42.
- [Google Scholar]
- Can screening and brief intervention lead to population-level reductions in alcohol-related harm? Addict Sci Clin Pract. 2012;28:15-8.
- [Google Scholar]




