
Translate this page into:
Uncommon presentation of a less common tumour
* For correspondence: savita2081@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 44 yr old male, presented to the department of Dermatology, Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, in January 2012 with a large 25x15cm nodulo-ulcerative growth over the right chest wall destroying the nipple-areolar complex. The lesion showed central puckering with infiltrative margins, was hard in consistency, and fixed on the chest wall (Fig. 1). Contrast enhanced computed tomography showed small shadows in bilateral lung parenchyma, suggestive of lung metastasis (Fig 2a and b). Skin punch biopsy showed clusters of tumour cells infiltrating dermis with desmoplasia and lymphovascular emboli (Fig. 3a). These cells were positive for oestrogen and progesterone receptors (Fig. 3b, c). A diagnosis of stage IV adenocarcinoma breast with cutaneous metastasis was made and palliative radiotherapy was administered. The patient died due to disease progression after four months.

- Multiple nodular and nodulo-ulcerative lesions exclusively involving the right chest wall and abdomen with destruction of the nipple-areola complex. The largest lesion on the chest shows central puckering.
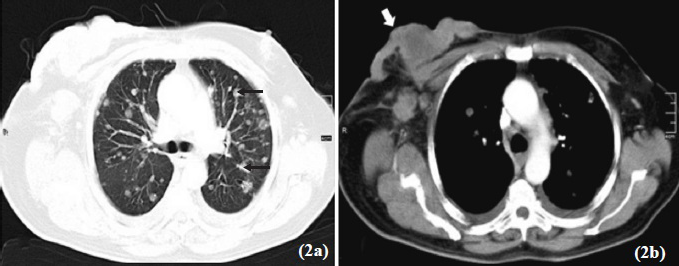
- Lung window of CECT chest showing multiple, rounded, nodular lesions (arrows) suggestive of metastases (b). Mediastinal window of CECT chest showing heterogenous attenuation soft tissue mass lesion involving right breast (arrow).
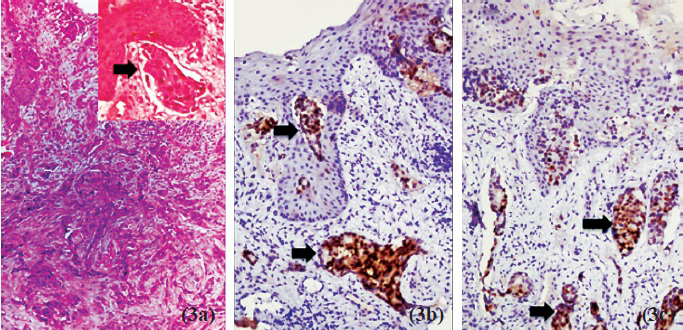
- Microphotograph of skin biopsy showing tumour infiltrating the dermis with desmoplasia and lymphovascular emboli (inset, arrow) (a, H&E x 10x, 40x). The tumour cells showed uniform positive staining for oestrogen (b), and progesterone (c) receptor (arrow) (DAB-Brown x 20x).
Male breast cancer is uncommon and direct extension into skin and surrounding structure can occur early but extensive and distant skin metastasis is rare. Increased awareness of cutaneous metastasis is necessary for early diagnosis and treatment.
Acknowledgment
The authors acknowledge the contribution of Dr Uma Nahar Saikia, Professor, Department of Histopathology, PGIMER in histopathological diagnosis of the patient.




