
Translate this page into:
Tuberous sclerosis with bilateral giant renal angiomyolipomas
* For correspondence: sureshsingla08@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 27 yr old female presented to the Urology department, Institute of Institute of Kidney Disease and Research Centre, Ahmedabad, Gujarat, in April, 2014 with bilateral dull aching flank pain, more on left side, early satiety, incapacitating her day-to-day activities for the last two months. She was on antiepileptic drugs for her convulsive episodes since early childhood. Examination revealed protuberant abdomen with multinodular, smooth, firm swellings and multiple adenoma sebaceum on her face (Fig. 1). Her biochemical investigations were within normal range, with serum creatinine-0.8 mg/dl. Contrast enhanced CT-abdomen revealed huge heterogeneously enhancing mass lesions with fat density (negative Hounsfield units) in both the kidneys, left kidney measuring 26x19x10.5cm, with barely visible renal parenchyma. Magnetic resonance imaging (MRI) brain showed cortical tubers in cerebrum and subependymal nodules in foramen of monro (Fig. 2). The patient underwent retroperitoneal laparoscopic control of renal artery followed by left open nephrectomy via flank retroperitoneal incision. Grossly, left kidney was totally distorted and replaced by multilobulated mass with no visible parenchyma and light microscopy on hematoxylin and eosin (H&E) staining revealed combination of mature adipose tissue, bundles of smooth muscle and abnormal blood vessels, suggestive of angiomyolipoma (Fig. 3). Presently, she is asymptomatic and her nadir serum creatinine was 1.1 mg/dl at six month follow up.
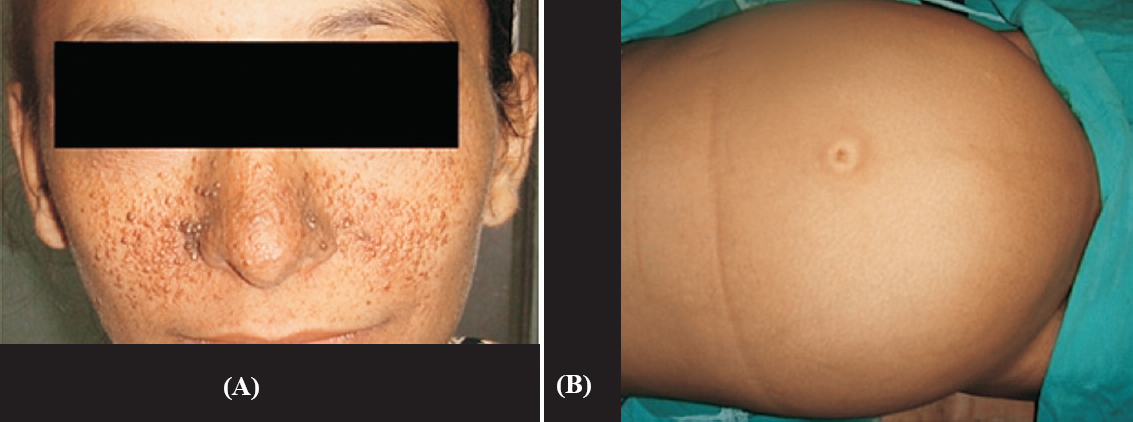
- Clinical photograph showing multiple adenoma sebaceum around nose and bilateral malar regions (A) and protuberant abdomen (B).
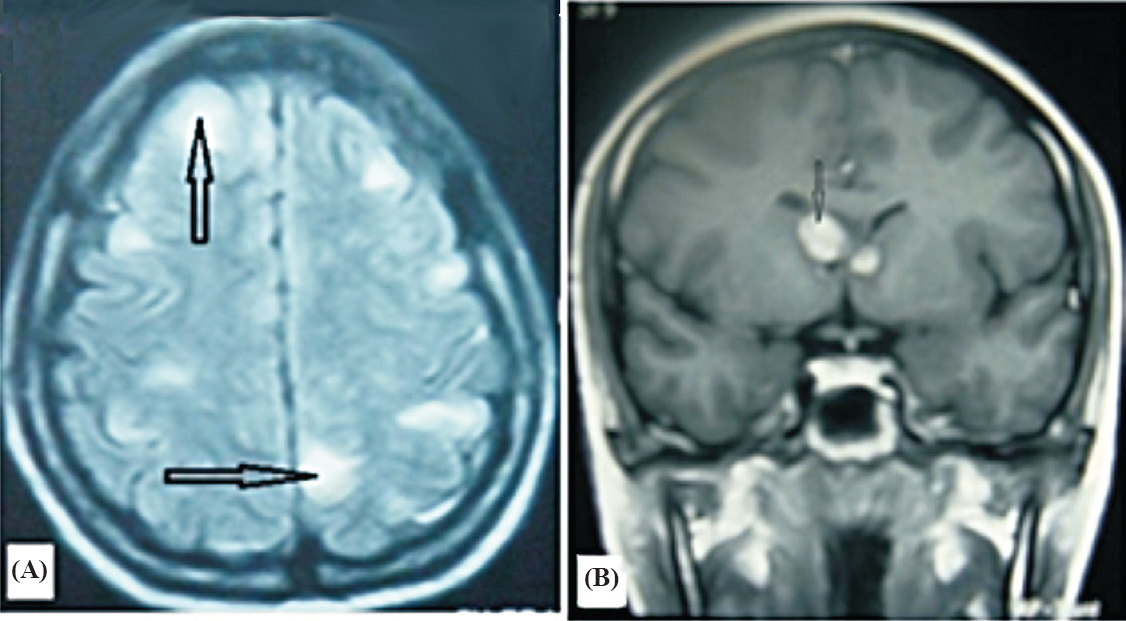
- Magnetic resonance imaging (MRI)-brain. (A) Multiple cortical tubers in cerebrum (black arrows). (B) Multiple subependymal nodules, largest at right side of foramen of Monro (black arrow).
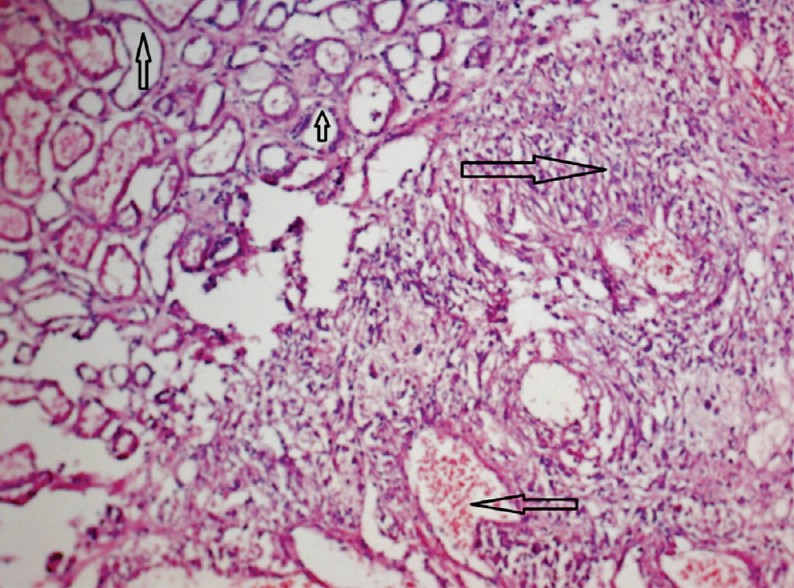
- Light microscopy (H&E, 100X) revealed combination of fat cells (upward arrows), smooth muscle component (right hand arrow) and blood vessels (left hand arrow).




