
Translate this page into:
The 2015 influenza A (H1N1) pdm09 outbreak in India
* For correspondence: mmurhekar@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
The influenza A(H1N1) pdm09 outbreak in India caused nearly 30,000 laboratory confirmed cases with more than 1700 deaths by March 15, 20151. Most of these cases were reported from the States of Rajasthan, Gujarat, Delhi, Jammu and Kashmir, Maharashtra, Madhya Pradesh, Telangana, Karnataka and Tamil Nadu2. In response to the upsurge of cases, the Central and State health departments initiated a number of activities including strengthening the surveillance; provision of laboratory support in terms of testing, quality assurance, supply of transport medium and diagnostic reagents; dissemination of guidelines for case management of cases and vaccination, making oseltamivir available through the public health system and schedule X chemists and educating the public through regular information, education and communication (IEC) activities3. We present here certain facts about the 2015 influenza A(H1N1) pdm09 outbreak and some lessons learnt for future.
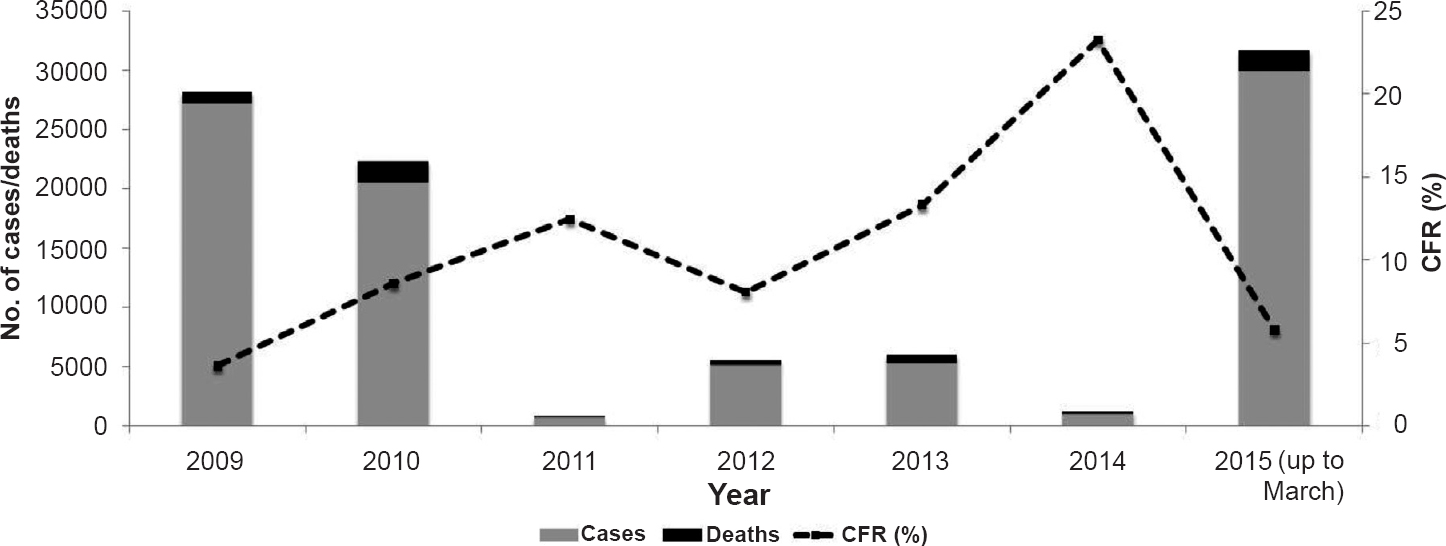
Cases and deaths in post-H1N1 pandemic period: During the 2009 pandemic, India reported 27,236 laboratory confirmed cases of pandemic influenza A (H1N1) with 981 deaths45. While declaring the post-pandemic phase in August 2010, the World Health Organization announced that the pandemic virus will continue as seasonal influenza virus6. Therefore, sporadic H1N1 cases as well as localized outbreaks of varying magnitude are expected in the post-2009 pandemic period.
As per the data from the Ministry of Health and Family Welfare, in the post-pandemic period (since 2010), India has reported more than 62,000 laboratory confirmed influenza A(H1N1)pdm09 cases with nearly 5000 deaths457 (Figure). The cases were reported throughout the year with bi-modal peaks - a major peak in rainy season (July-August), and a minor peak in winter-spring season (December-February)789.
The resurgence of cases could be on account of gaps in population immunity as well as conducive climatic condition such as prolonged cold season in many States in India. A meta-analysis based on sero-surveys conducted in 19 countries including India after 2009 and 2010 waves of pandemic influenza reported that about one third (32%, 95% CI: 26-39) of the population tested was seropositive, indicating that the remaining population was still not exposed to the pandemic virus and hence the post-pandemic cases/outbreaks are expected10.
The Government of India guidelines for case management of influenza A/H1N1 require classification of influenza patients into three categories - Category A includes mild cases where no laboratory testing or antiviral treatment is needed. The category B includes high-risk patients such as children, pregnant women, persons aged ≥ 65 yr and people with chronic disease. These patients need not be laboratory confirmed but should be isolated at their homes and given oseltamivir treatment. Category C patients are severe cases who need hospitalization, laboratory testing and oseltamivir treatment11. The numbers of cases of severe illness and deaths are the most commonly used indicators of severity of influenza outbreak12. Information on severity categorization of cases that occurred during December 2014 and March 2015 has not been routinely collected; hence it is not possible to comment if the virus has recently become more virulent. However, based on the number of reported deaths due to H1N1, the case-fatality ratio (CFR) of 5.8 per cent among the laboratory confirmed cases during January-March 2015 does not appear to be different than earlier years where it ranged between 3.6 and 23.3 per cent (average: 6.9%). The true CFR may be much lower since the reported number of cases (used in the denominator) does not represent true disease burden.
In India, where routine influenza vaccination programme does not exist, identifying risk factors for adverse outcomes and targeting high risk groups for early hospital admission and tamiflu treatment could also be useful public health strategies, besides the emphasis on case-categorization based treatment algorithms.
Has the virus mutated since 2009?: Influenza virus frequently mutates and such drifts are known to affect the transmissibility as well as virulence of the virus12. A large number of deaths reported in the 2015 outbreak raised such a concern. A recent report indicates that the 2014 Indian H1N1 strain has undergone mutations thereby increasing its virulence13. A complete genome analysis conducted by National Institute of Virology, Pune, on six virus strains from the 2015 outbreak indicates that the virus has not undergone any genetic changes that could have affected H1N1 virulence or resistance to oseltamivir14.
Influenza vaccination is most effective when circulating viruses are well matched with vaccine viruses. In India, as the risk groups are not clearly identified, only healthcare workers working in close proximity to influenza patients have been recommended to receive the H1N1 vaccine during the 2015 outbreak15.
What have we learnt from the 2015 H1N1 outbreak?: Besides making people aware about the ways to minimize the transmission, and ensuring appropriate management of cases including the use of tamiflu only for category B and C patients, health authorities also need to focus on better documentation of the outbreak in terms of descriptive epidemiology, clinical details and severity category of cases in order to identify risk factors for adverse outcomes. These data will also be useful in identifying additional high-risk groups, which could be considered for vaccination.
In the 2015 influenza outbreak, clinical and epidemiological information from laboratory confirmed cases and deaths was collected by the State Integrated Disease Surveillance Programmes and only the information about number of laboratory confirmed cases and deaths was sent to the national authorities on a daily basis. It might be useful if thoughtfully developed uniform data collection tools are used by all the States to collect clinical, epidemiological and treatment related data from laboratory confirmed cases and analyzed in a timely manner. Additionally, periodic and frequent release of communications about the evolving epidemic to the public and the public health authorities making full use of available data will also help in mitigating rumors and misinterpretation.
In conclusion, the key lessons learnt from the 2015 H1N1 outbreak include: (i) in the post-pandemic period, cases of H1N1 influenza and related deaths are expected to continue to occur; (ii) it is important to adhere to the guidelines released by the government for management of H1N1 influenza patients and milder patients need not be treated with oseltamivir and may not require hospitalization; (iii) there is no evidence to suspect significant genetic change in virus affecting its virulence in the recent time; (iv) better documentation of the burden of H1N1 cases, associated risk factors and adverse outcomes is critically important.
Conflicts of Interest: None.
References
- The New Indian Express. Available from: http://www.newindianexpress.com/nation/People-in-30-45-Age-Group-Worst-Affected-by-Swine-Flu/2015/03/18/article2719779.ece
- Press Trust of India. Available from: http://pib.nic.in/newsite/erelease.aspx
- Ministry of Health and Family Welfare, Government of India. Seasonal Influenza A H1N1. Actions taken by Ministry of Health and Family Welfare. Available from: http://mohfw.gov.in/showfile.php?lid=3080
- 2009. Central Bureau of Health Intelligence. National Health Profile of India. Available from: http://cbhidghs.nic.in/writereaddata/linkimages/8%20Health%20Status%20Indicators4950277739.pdf
- Press Information Bureau, Government of India, Ministry of Health and Family. Preventive measures on swine flu. Available from: http://pib.nic.in/newsite/PrintRelease.aspx?relid=115710
- WHO. Global Alert and Response. What is post pandemic? 10 August 2010. Available from: http://www.who.int/csr/disease/swineflu/frequently_asked_questions/post_pandemic/en/
- 2010. Central Bureau of Health Intelligence. National Health Profile of India. Available from: http://cbhidghs.nic.in/writereaddata/mainlinkFile/File1012.pdf
- Emergence of pandemic 2009 influenza A H1N1, India. Indian J Med Res. 2012;135:534-7.
- [Google Scholar]
- Dynamic patterns of circulating seasonal and pandemic A(H1N1)pdm09 influenza viruses from 2007-2010 in and around Delhi, India. PLoS One. 2012;7:e29129.
- [Google Scholar]
- Estimating age-specific cumulative incidence for the 2009 influenza pandemic: a meta-analysis of A(H1N1)pdm09 serological studies from 19 countries. Influenza Other Respir Viruses. 2013;7:872-86.
- [Google Scholar]
- Ministry of Health and Family Welfare, Government of India. Guidelines on categorization of Influenza A H1N1 cases during screening for home isolation, testing treatment, and hospitalization (Revised on 11.02.2015). Available from: http://mohfw.gov.in/showfile.php?lid=3071
- WHO. Global Alert and Response (GAR). Assessing the severity of an influenza pandemic. 11 May 2009. Available from: http://www.who.int/csr/disease/swineflu/assess/disease_swineflu_assess_20090511/en/
- Influenza surveillance: 2014-2015 H1N1 “Swine”- derived influenza viruses from India. Cell Host Microbe. 2015;17:279-82.
- [Google Scholar]
- Press Information Bureau, Government of India. Press Note from National Institute of Virology Pune. 12 March 2015. Available from: http://pib.nic.in/newsite/PrintRelease.aspx?relid=116939
- Directorate General of Health Services, Ministry of Health and Family Welfare (Emergency Medical Relief) Seasonal Influenza A (H1N1): Guidelines for Vaccination of Health Care Workers (Updated on 14 February 2015). Available from: http://mohfw.gov.in/showfile.php?lid=3073




