Translate this page into:
Testicular seminoma with early carcinomatous differentiation
*For correspondence: Bahçelievler Mah. Çamlik Cad. No: 2, ÇORUM, Turkey dr.selahattin@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 25 year old male patient presented to the Urology Clinic, department of Urology, Haydarpasa Numune Training and Research Hospital, Istanbul, Turkey, in March 2013, with painless testicular mass for the last three months. Physical examination revealed a 20x15 cm sized right testicular mass (Fig. 1). Computerized tomography showed 10x9 cm sized mass in the retroperitoneal area (Fig. 2). Serum tumour markers were measured. Serum alpha foeto protein (AFP), beta human chorionic gonadotropin (ß-hCG) and lactate dehydrogenase (LDH) levels were 1.59 U/l, 16.34 IU/l and 955 U/l, respectively. The patient underwent inguinal surgical orchiectomy for definitive diagnosis and treatment. Macroscopically, this right testicular mass was 19x13x6 cm in size, that consisted of focal necrosis and haemorrhage. Infiltration of tunica albuginea with tumour cells was seen. Microscopically, extensive necrosis, lymphovascular invasion, infiltration of rete testis, epididymis, tunica vaginalis and albuginea suggested the high mitotic activitiy of atypical seminoma. Immunohistochemically, the tumour cells were diffusely positive for podoplanin and focal positive for CD 30 (Fig. 3), but were negative for placental alkaline phosphatase (PLAP), c-kit CD117, CK(cytokeratin) 8/18, CK 19, high molecular weight cytokeratin (HMWCK) and pan-cytokeratin (PANCK). After pathological examination, the patient was treated with four cycles of bleomycin, etoposide and cisplatin chemotherapy and radiotheraphy for para-aortic regimen with 3600 cGy. After this treatment, second line chemotherapy including paclitaxel, ifosfamide and cisplatin was performed. The patient was followed up for one year without recurrence and metastasis.
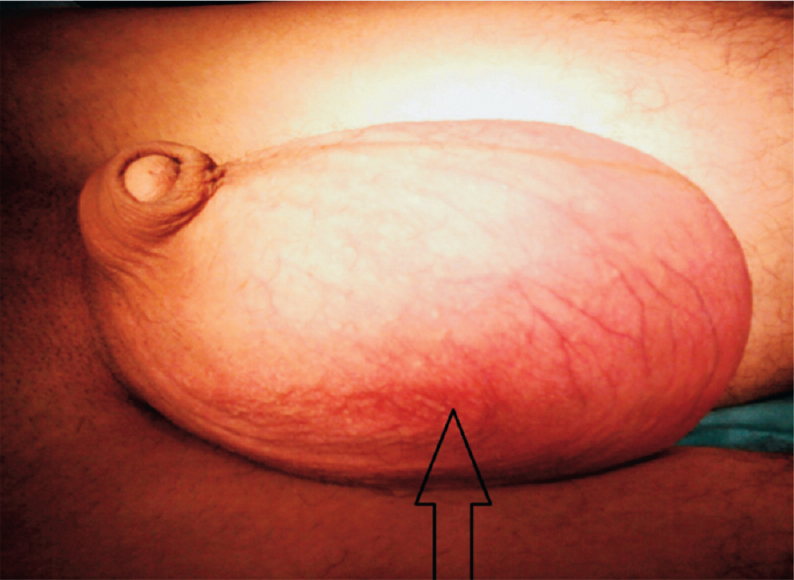
- Giant testicular mass on phsycial examination (arrow).
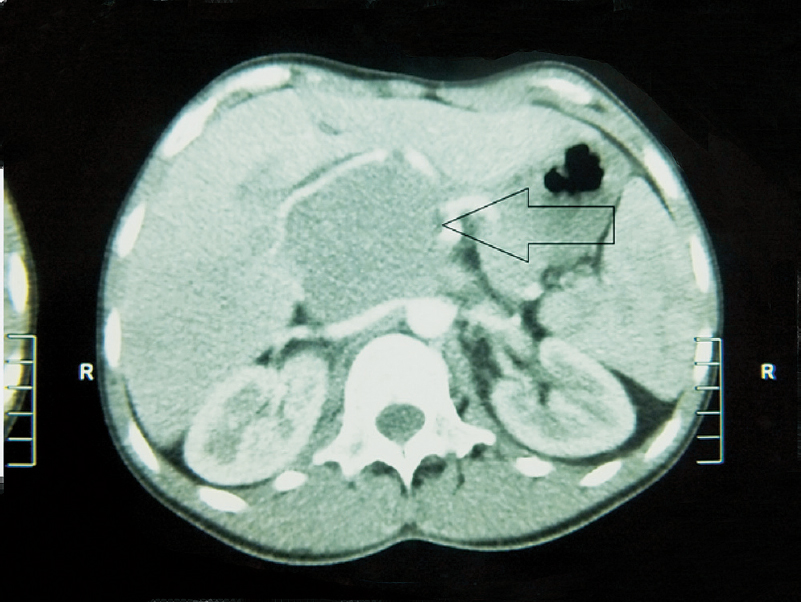
- Computerized tomography of retroperitoneal lymphadenopathy. Arrow shows 10 ×9 cm mass.
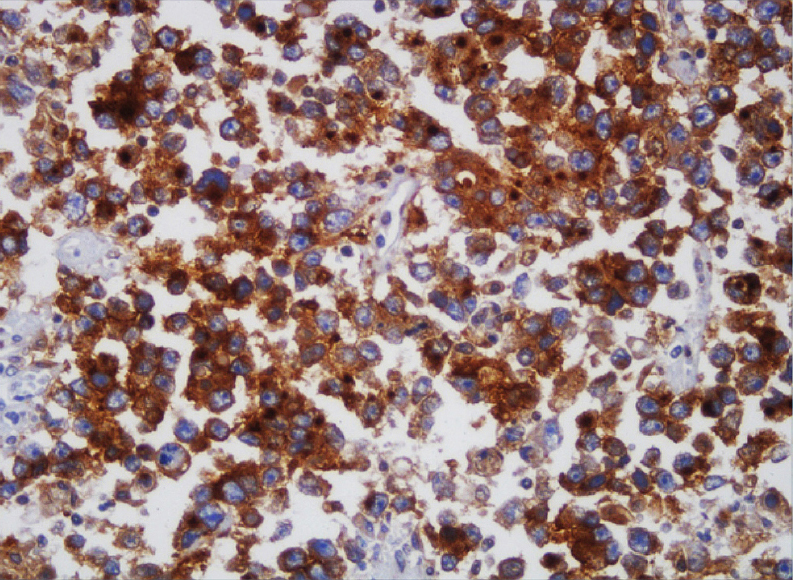
- The tumour cells with cytoplasmic and perinuclear “dot-like” staining with podoplanin (×40).
Atypical seminoma was defined as an intermediate neoplasm between embryonal carcinoma and classical seminoma1. Tumour cells showing moderate or marked nuclear pleomorphism, nuclear overlapping, lack or paucity of cytoplasmic clarity were considered as atypical seminomas2. All seminomas are not the same, rare cases may grow in a more agressive manner than expected. Positive CD30 may be showing early carcinomatous differantiation of some seminomas3. Early carcinomatotus differentiation is an infrequent phenomenon, which can progress to advanced disease2.
References
- Fine-needle aspiration cytology of unusual germ cell tumors of the mediastinum: Atpical seminoma and parietal yolk sac tumor. Diagn Cytopathol. 2002;27:69-74.
- [Google Scholar]
- Testicular seminoma: A clinicopathologic and immunohistochemical study of 105 cases with special reference to seminomas with atypical features. Int J Surg Pathol. 2002;10:23-32.
- [Google Scholar]
- The ultrastructure and histogenesis of male germ cell neoplasia with emphasis on seminoma with early carcinomatous features. Ultrastruct Pathol. 1988;12:67-86.
- [Google Scholar]




