
Translate this page into:
Susceptibility profile, resistance mechanisms & efficacy ratios of fosfomycin, nitrofurantoin & colistin for carbapenem-resistant Enterobacteriaceae causing urinary tract infections
For correspondence: Dr Rani Diana Sahni, Department of Clinical Microbiology, Christian Medical College, Vellore 632 004, Tamil Nadu, India e-mail: rdsahni@hotmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
The escalation in carbapenem resistance among Enterobacteriaceae has resulted in a lack of effective therapeutic alternatives. Older antimicrobials, fosfomycin, nitrofurantoin and colistin for urinary tract infections (UTIs) caused by carbapenem-resistant Enterobacteriaceae (CRE) may be effective treatment options. The objectives of this study were to evaluate the utility of fosfomycin, nitrofurantoin and colistin in treating UTI caused by CRE and molecular characterization of the plasmid-mediated carbapenem resistance mechanisms.
Methods:
Consecutive, non-duplicate isolates of CR Escherichia coli and Klebsiella spp. from urine cultures were included (n=150). Minimum inhibitory concentrations (MIC) were determined by E-test (fosfomycin and nitrofurantoin) and broth microdilution (colistin). Efficacy ratios were derived by dividing susceptibility breakpoints by observed MIC values of the drugs for the isolates. Isolates were screened for genes coding for carbapenemases using multiplex PCR. Fosfomycin, nitrofurantoin and colistin-resistant isolates were screened for plasmid-borne resistance genes fosA3, oqxAB and mcr-1, respectively using PCR.
Results:
Among E. coli, 98.9, 56 and 95 per cent isolates were susceptible to fosfomycin, nitrofurantoin and colistin, respectively, while 94 and 85 per cent of Klebsiella spp. were susceptible to fosfomycin and colistin, respectively. The efficacy ratios indicated fosfomycin as the drug of choice for UTI caused by CR E. coli and Klebsiella spp., followed by colistin. The blaNDM gene was most common, followed by blaOXA48-like. Plasmid-borne genes encoding resistance to fosfomycin, nitrofurantoin and colistin were absent.
Interpretation & conclusions:
With increasing resistance against the current treatment options, older drugs may emerge as effective options. Molecular screening of resistant isolates is essential to prevent the spread of plasmid-borne resistance against these drugs.
Keywords
Carbapenem-resistant Enterobacteriaceae
colistin
fosfomycin
nitrofurantoin
therapeutic efficacy

Urinary tract infections (UTIs) constitute a major burden of bacterial infections world over1. Carbapenems are the drug of choice for treating UTIs caused by multidrug-resistant Enterobacteriaceae such as Escherichia coli and Klebsiella species. Increasing carbapenem resistance among Enterobacteriaceae has resulted in a lack of effective therapeutic alternatives for UTIs caused by carbapenem-resistant Enterobacteriaceae (CRE). Therefore, revival of older antimicrobial agents such as fosfomycin, nitrofurantoin and colistin for treating these UTIs seems to be a feasible option23. However, plasmid-mediated mechanisms against these older drugs have also been reported45. The spread of these resistance plasmids further complicates the situation. Molecular screening for plasmid-borne isolates has become important in controlling their spread.
The choice of an appropriate agent to treat an infection is generally based on the minimum inhibitory concentrations (MIC) values whenever available. However, deriving the efficacy ratio, which is the ratio of susceptibility breakpoint value by the MIC value obtained, is a better indicator of an agent that should be chosen against a pathogen6. A higher efficacy ratio is indicative of a drug being more effective than those with a lower efficacy ratio.
The aim of this study was to evaluate the role of fosfomycin, nitrofurantoin and colistin in treating UTIs caused by CR E. coli and Klebsiella species. The objectives included to collate and analyze susceptibility profile of the first- and second-line antimicrobials used for UTIs; to determine MIC of fosfomycin, nitrofurantoin and colistin for E. coli and Klebsiella spp.; to calculate the efficacy ratios of these antimicrobials; to perform molecular characterization of CR E. coli and Klebsiella spp. and to screen the fosfomycin, nitrofurantoin and colistin-resistant isolates for carriage of plasmid-borne fosA3, oqxAB genes and mcr-1 genes coding for fosfomycin, nitrofurantoin and colistin resistance, respectively.
Material & Methods
This prospective study was conducted in the department of Clinical Microbiology, Christian Medical College and Hospital, Vellore, India, between January 2016 and June 2017. The study was approved by the Institutional Review Board (IRB Min No: 9830).
Urine samples received from hospitalized patients for culture were processed using the routine semi-quantitative culture method7. The types of samples included were catheter samples, mid-stream clean catch samples, percutaneous nephrostomy, suprapubic catheter, suprapubic aspirate, ileal conduit and condom catheter. A total of 150 consecutive, non-duplicate isolates of E. coli and Klebsiella spp., satisfying the inclusion criteria (isolates found in probably significant or significant colony counts and resistant to imipenem, meropenem and ertapenem by disc diffusion method) and exclusion criteria (repeat urine culture from patients already included) were included in this study.
Antimicrobial susceptibility testing: Antimicrobial susceptibility testing by disk diffusion was performed as a part of the routine testing and interpretation was done according to the Clinical and Laboratory Standard Institute (CLSI) guidelines8. Isolates were tested for susceptibility to cefpodoxime (10 μg), amoxicillin-clavulanate (20/10 μg), piperacillin-tazobactam (100/10 μg), cefoperazone-sulbactam (75/30 μg), gentamicin (10 μg), amikacin (30 μg), netilmicin (30 μg), ciprofloxacin (5 μg) and trimethoprim-sulphamethoxazole (1.25/23.75 μg) by Kirby-Bauer disk diffusion method9.
The MICs of fosfomycin (n=150) and nitrofurantoin (n=81) were determined using E-test strips (AB Biodisk BioMérieux, France) following manufacturer's protocol. The nitrofurantoin MIC (μg/ml) results were interpreted using CLSI guidelines (≤32 susceptible, 64 intermediate and ≥128 resistant)8. The CLSI guidelines do not provide fosfomycin susceptibility clinical breakpoints for Klebsiella spp. thus, the results were interpreted using breakpoints provided for E. coli. For fosfomycin, the MIC value (μg/ml) interpretation was: ≤64 susceptible, 128 intermediate and ≥256 resistant8.
For colistin susceptibility testing, the isolates (n=150) were subjected to the broth microdilution (BMD) method, with susceptible E. coli ATCC 25922, Pseudomonas aeruginosa ATCC 27853 and mcr-1 positive E. coli NCTC13846 (Courtesy: Dr Olga Perovic, National Institute for Communicable Diseases, Johannesburg, South Africa) as the quality control strains10. The antibiotic pure substance, colistin sulphate powder, was obtained from Sigma-Aldrich, USA. The results were interpreted using the European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines version 8, 2018 (http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/General_documents/Tigecycline_Guidance_document_20181223.pdf) (susceptible ≤2 mg/l and resistant >2 mg/l).
Molecular characterization: Molecular detection of resistance genes coding for carbapenemases: Multiplex PCR was performed for detection of carbapenem resistance genes coding for carbapenemases. Isolates were screened for the production of Class A Klebsiella pneumoniae carbapenemase (KPC)11, Class B carbapenemases active on imipenem (IMP), verona integron-encoded metallo-β-lactamase (VIM) and New Delhi metallo-β-lactamase (NDM)1213 and Class D carbapenemase OXA48-like12. The amplification of genes was performed using Veriti Thermal cycler (Applied Biosystems, USA) using the following cycling condition; initial denaturation at 95°C for 15 min, 30 cycles of 94°C for 30 sec, 59°C for 1.5 min, 72°C for 1.5 min and final extension at 72°C for 10 min followed by hold at 4°C. Amplicons were visualized on two per cent agarose gel using electrophoresis. Control strains were obtained from International Health Management Associates, USA.
Molecular detection of plasmid-borne oqxAB genes coding for nitrofurantoin resistance: The nitrofurantoin resistant E. coli were screened for carriage of plasmid-borne resistance genes oqxAB using a modified version of the PCR protocol described earlier14. Briefly, amplification of genes was performed using Veriti Thermal cycler with the following cycling condition; initial denaturation at 95°C for 5 min, 35 cycles of 94°C for 30 sec, 52°C for 60 sec, 72°C for 60 sec and final extension at 72°C for 7 min followed by hold at 4°C. Amplicons were visualized on two per cent agarose gel using electrophoresis.
Molecular detection of plasmid-borne colistin resistance gene mcr-1: The colistin-resistant isolates were screened for plasmid-borne resistance gene mcr-1 using a modified version of the PCR protocol described earlier5. Briefly, amplification of genes was performed using Veriti Thermal cycler using the following cycling condition; initial denaturation at 95°C for 10 min, 25 cycles of 95°C for 60 sec, 58°C for 30 sec, 68°C for 60 sec and final extension at 72°C for 10 min followed by hold at 4°C. Amplicons were visualized on two per cent agarose gel using electrophoresis.
Calculation of efficacy ratio: The efficacy ratio of the drugs was derived by dividing the susceptible breakpoint MIC as per CLSI guidelines8 by the MIC result obtained by E-test (fosfomycin and nitrofurantoin) or broth microdilution (BMD, colistin)6. The efficacy ratios were compared to predict the most effective agent for UTI caused by E. coli and Klebsiella species. Since nitrofurantoin MIC by E-test was determined only for E. coli, the nitrofurantoin efficacy ratio for Klebsiella spp. could not be calculated.
Results
On routine antimicrobial susceptibility testing of the CR E. coli, 98.8 per cent were found to be resistant tocefpodoxime, amoxicillin-clavulanate, cefoperazone-sulbactam each and 96.3 per cent were resistant to piperacillin-tazobactam. The resistance rates of the aminoglycosides were as follows: netilmicin - 77.8 per cent, amikacin - 76.5 per cent and gentamicin 86.4 per cent, while 88.9 per cent were resistant to trimethoprim/sulphamethoxazole and 95.1 per cent to ciprofloxacin. Among the CR Klebsiella spp., all the isolates (100%) were resistant to cefpodoxime, cefoperazone-sulbactam and piperacillin-tazobactam, and 99 per cent of them were resistant to amoxicillin-clavulanate. Resistance to aminoglycosides was 87 per cent for gentamicin and amikacin, and 96 per cent for netilmicin, while 80 and 93 per cent of the isolates were resistant to trimethoprim/sulphamethoxazole and ciprofloxacin, respectively.
The MICs of fosfomycin and colistin for all 150 isolates and of nitrofurantoin for E. coli isolates are summarized in Table I. The susceptibility profile of the isolates is shown in Table II. The efficacy ratios calculated for fosfomycin, colistin and nitrofurantoin are shown in Figs 1 and 2. The fosfomycin efficacy ratio for E. coli was ≥4 for majority of the isolates (96%, n=78), while, the fosfomycin efficacy ratio for Klebsiella spp. was ≥4 for 74 per cent of isolates (n=51). Fosfomycin was more active against E. coli than Klebsiella spp. Similarly, the number of isolates with high colistin efficacy ratio was more for E. coli than Klebsiella spp., making colistin a better agent for CR E. coli than CR Klebsiella species. However, for nitrofurantoin, the number of E. coli isolates with nitrofurantoin efficacy ratio of one or less than one was 62 per cent (n=50). Thus, among the three agents tested for CR E. coli, the order of preference was fosfomycin, followed by colistin and nitrofurantoin; while for CR Klebsiella spp., fosfomycin was preferred over colistin.
| Organism | Fosfomycin MIC (n=150) (µg/ml) | Nitrofurantoin MIC (n=81) (µg/ml) | Colistin MIC (n=150) (µg/ml) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MIC range | MIC50 | MIC90 | Mean MIC | MIC range | MIC50 | MIC90 | Mean MIC | MIC range | MIC50 | MIC90 | Mean MIC | |
| Escherichia coli (n=81) | 0.25-96 | 0.75 | 8 | 9.8 | 2->128 | 32 | >128 | 34 | 0.12-16 | 0.5 | 2 | 1.6 |
| Klebsiella spp. (n=69) | 0.25->256 | 16 | 48 | 12.5 | NA | NA | NA | NA | 0.25-32 | 1 | 8 | 2.1 |
NA, not available
| Isolate | Non-susceptible (%) | ||
|---|---|---|---|
| Fosfomycin | Nitrofurantoin | Colistin | |
| Escherichia coli (n=81) | 1.2 (n=1) | 44 (n=36) | 5 (n=4) |
| Klebsiella spp. (n=69) | 6 (n=4) | NA | 15 (n=10) |
NA, not available
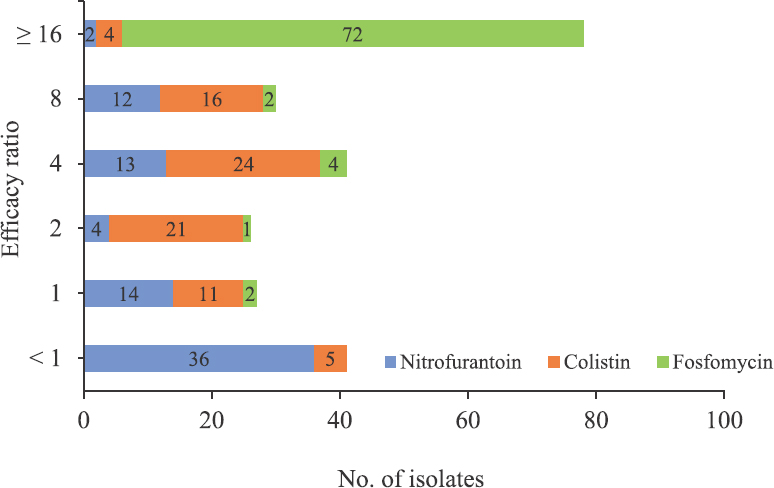
- Comparison of efficacy ratio of fosfomycin, nitrofurantoin and colistin for E.coli.
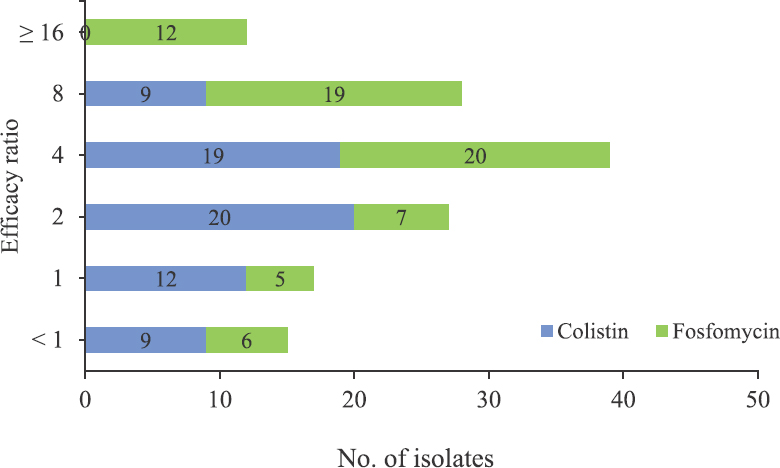
- Comparison of the efficacy ratio of fosfomycin and colistin for Klebsiella spp.
The results of the PCR for detection of genes encoding carbapenemase enzymes blaIMP, blaVIM, blaNDM, blaKPC and blaOXA48-like are summarized in Table III. Among E. coli isolates, the most common gene detected was blaNDM followed by blaOXA48-like, whereas in Klebsiella spp., blaOXA48-like was more common than blaNDM. Co-carriage of more than one carbapenemase genes was also detected in 16 isolates. Plasmid-borne fosfomycin resistance gene fosA3 was absent in E. coli (n=1) isolate that showed intermediate susceptibility to fosfomycin. There was no co-carriage of plasmid-borne nitrofurantoin resistance gene oqxAB in the nitrofurantoin resistant E. coli. Co-carriage of plasmid-borne colistin resistance gene mcr-1 was absent in the colistin resistant E. coli or Klebsiella species.
| Isolate | Genes detected | blaIMP | blaVIM | blaNDM | blaKPC | blaOXA48-like | Co-producers |
|---|---|---|---|---|---|---|---|
| Escherichia coli (n=81) | Carbapenemases | - | Positive 1.2% (n=1) | Positive 43% (n=35) | - | Positive 14% (n=11) | Positive 6% (n=5) |
| Co-occurrence of mcr-1 gene (n=4) or oqxAB genes (n=36) or fosA3 (n=1) | - | Negative | Negative | - | Negative | Negative | |
| Klebsiella spp. (n=69) | Carbapenemases | - | Positive 1.4% (n=1) | Positive 23% (n=16) | - | Positive 35% (n=24) | Positive 17% (n=12) |
| Co-occurrence of mcr-1 gene (n=10) | - | Negative | Negative | - | Negative | Negative |
Discussion
On routine antimicrobial susceptibility testing, amikacin resistance was found to be lower than most other drugs. Hu et al15 reported 87 per cent amikacin resistance in CRE, whereas Moemen and Masallat16 reported 52.4 per cent amikacin resistance which was much lower as compared to resistance against other drugs. Piperacillin-tazobactam resistance was; 96.3 per cent for E. coli and 100 per cent for Klebsiella species. Other groups1516 reported 98.7 and 97.6 per cent piperacillin-tazobactam resistance for CRE, respectively. When tested against cefoperazone-sulbactam, 98.8 per cent E. coli and 100 per cent Klebsiella spp. were found to be resistant. Hu et al15 reported 88.3 per cent cefoperazone-sulbactam resistance.
The susceptibility testing for fosfomycin showed good in vitro activity with 98.8 and 94 per cent susceptibility among E. coli and Klebsiella spp., respectively. Livermore et al17 reported fosfomycin susceptibility of 100 per cent in CR E. coli but only 48.1 per cent in CR Klebsiella species. Falagas et al18 reported 95 per cent susceptibility among carbapenemase-producing Enterobacteriaceae. In India, Sahni et al19 reported susceptibility rate of 83 per cent among the E. coli (n=2416) isolated from urine between 2009-2010 whereas Rajenderan et al20 found that fosfomycin inhibited 90 per cent of E. coli and Klebsiella spp. from various samples, including urine. The efficacy ratio of fosfomycin for CR E. coli and CR Klebsiella spp. also indicated good activity of this agent.
Nitrofurantoin MIC was determined only for the E. coli isolates. Only 56 per cent of the isolates were susceptible to nitrofurantoin. Shanmugam et al21 reported 51 per cent susceptibility to nitrofurantoin among CR E. coli. Although studies specific to nitrofurantoin susceptibility in CRE are limited, various studies done on multidrug resistance (MDR) or extended-spectrum beta-lactamases producing E. coli from urine samples, report the considerable difference in susceptibility to nitrofurantoin2223. The efficacy ratios of nitrofurantoin for E. coli were not as promising as those for fosfomycin or colistin. The colistin susceptibility rates for E. coli and Klebsiella spp. were 95 and 85 per cent respectively. Overall, 90.7 per cent of the isolates were susceptible to colistin. Süzük et al24 from Turkey reported 96.8 per cent colistin susceptibility among CRE, while a study from Pakistan25 found 84.1 per cent colistin susceptibility among CRE.
From the efficacy ratios of the three drugs calculated, fosfomycin appeared to be a good treatment option in the management of CR E. coli followed by colistin and nitrofurantoin. For CR Klebsiella spp., fosfomycin followed by colistin appeared to be good therapeutic options.
The most common carbapenemase gene detected was blaNDM in 37 per cent followed by blaOXA48-like in 23 per cent isolates, with a predominance of blaNDM in E. coli (68.5) and of blaOXA48-like in Klebsiella spp. (42.6%). A study from Bangladesh reported blaNDM (50%) followed by blaOXA48-like (20%) on CR uropathogens26. Sharma et al27 reported blaNDM (32%) and blaOXA48-like (32%) in septicaemia cases. Co-carriage of more than one gene was detected in 14 per cent isolates, with 75 per cent of them co-carrying blaNDM and blaOXA48-like. Similar findings were reported by other investigators2628.
Nitrofurantoin resistance in E. coli may be chromosomal or plasmid-mediated. The mutations in chromosomal genes nfsA and nfsB (encoding oxygen-insensitive nitroreductases) and the deletion in ribE (encoding lumazine synthase involved in biosynthesis of flavin mononucleotide) contribute to nitrofurantoin resistance2930 whereas the plasmid-borne resistance genes oqxAB encode an efflux pump active for nitrofurantoin4. None of the isolates was positive for oqxAB genes. The resistance in these isolates could be chromosome-mediated. For fosfomycin, chromosomal mutations can affect the function of the transport systems, involved in its uptake by the bacteria. Fosfomycin inactivating enzymes (metalloenzymes and kinases) produced by bacteria also lead to resistance. In E. coli, fosA3 gene coding for fosfomycin inactivating enzyme was reported to be co-carried on the same plasmid as oqxAB3132.
Colistin resistance is mainly due to alteration in the lipopolysaccharide of bacterial outer membrane. Mutations in genes involved in lipid A modifications, such as mutations in mgrB gene are known to cause colistin resistance. Plasmid (mcr-1, mcr-2, mcr-, mcr-3, mcr-4 and mcr-5) mediated resistance has been reported among E. coli and Klebsiella spp.5. The mcr-1 gene codes for phosphoethanolamine transferase that modifies the pEtN moiety of lipid A, conferring resistance to colistin33. The colistin-resistant isolates in this study were not found to carry mcr-1 gene. This could be due to chromosome-mediated mechanisms or presence of other variants of mcr gene not evaluated in this study.
Currently, in the midst of widespread plasmid-mediated resistance, the absence of plasmid-mediated fosfomycin, nitrofurantoin and colistin resistance is a relief. However, continuous screening and surveillance of isolates to prevent the rapid spread of plasmid-borne resistance are essential.
Financial support & sponsorship: The study was funded by the Fluid Research Grant from Christian Medical College, Vellore.
Conflicts of Interest: None.
References
- Urinary tract infections: Disease panorama and challenges. J Infect Dis. 2001;183(Suppl 1):S1-4.
- [Google Scholar]
- A new strategy to fight antimicrobial resistance: The revival of old antibiotics. Front Microbiol. 2014;5:551.
- [Google Scholar]
- Plasmid-mediated oqxAB is an important mechanism for nitrofurantoin resistance in Escherichia coli. Antimicrob Agents Chemother. 2016;60:537-43.
- [Google Scholar]
- Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: A microbiological and molecular biological study. Lancet Infect Dis. 2016;16:161-8.
- [Google Scholar]
- Use of Antimicrobial Susceptibility Data to Guide Therapy. Available from: https://www.animalhealth.msu.edu/sections/bacteriology/WEBCD.BACT.REF.013.pdf
- Cumitech 2c: Laboratory diagnosis of urinary tract infections. American Society Mic Series. Washington, DC: ASM Press; 2009.
- [Google Scholar]
- Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. USA: CLSI; 2017.
- [Google Scholar]
- Jorgensen JH, Pfaller MA, Carroll KC, Funke G, Landry ML, Richter SS, eds. Manual of clinical microbiology (11th ed). Washington, DC: American Society of Microbiology; 2015.
- European Committee on Antimicrobial Susceptibility Testing (EUCAST) warnings concerning antimicrobial susceptibility testing products or procedures. Available from: http://www.eucast.org/ast_of_bacteria/warnings/
- Novel carbapenem-hydrolyzing beta-lactamase, KPC-1, from a carbapenem-resistant strain of Klebsiella pneumoniae. Antimicrob Agents Chemother. 2001;45:1151-61.
- [Google Scholar]
- Multiplex PCR for detection of acquired carbapenemase genes. Diagn Microbiol Infect Dis. 2011;70:119-23.
- [Google Scholar]
- Development of a set of multiplex PCR assays for the detection of genes encoding important beta-lactamases in Enterobacteriaceae. J Antimicrob Chemother. 2010;65:490-5.
- [Google Scholar]
- Independent emergence of colistin-resistant Enterobacteriaceae clinical isolates without colistin treatment. J Clin Microbiol. 2011;49:4022-3.
- [Google Scholar]
- Emergence of carbapenem-resistant clinical Enterobacteriaceae isolates from a teaching hospital in Shanghai, China. J Med Microbiol. 2012;61:132-6.
- [Google Scholar]
- Prevalence and characterization of carbapenem-resistant Klebsiella pneumoniae isolated from Intensive Care Units of Mansoura University hospitals. Egypt J Basic Appl Sci. 2017;4:37-41.
- [Google Scholar]
- What remains against carbapenem-resistant Enterobacteriaceae? E valuation of chloramphenicol, ciprofloxacin, colistin, fosfomycin, minocycline, nitrofurantoin, temocillin and tigecycline. Int J Antimicrob Agents. 2011;37:415-9.
- [Google Scholar]
- Antimicrobial susceptibility of multidrug-resistant (MDR) and extensively drug-resistant (XDR) Enterobacteriaceae isolates to fosfomycin. Int J Antimicrob Agents. 2010;35:240-3.
- [Google Scholar]
- Evaluation of fosfomycin activity against uropathogens in a fosfomycin-naive population in South India: A prospective study. Future Microbiol. 2013;8:675-80.
- [Google Scholar]
- Determination of MIC distribution of Arbekacin, Cefminox, Fosfomycin, Biapenem and other antibiotics against gram-negative clinical isolates in South India: A prospective study. PLoS One. 2014;9:e103253.
- [Google Scholar]
- Molecular characterisation of nfsA gene in nitrofurantoin resistant uropathogens. J Clin Diagn Res. 2016;10:DC05-9.
- [Google Scholar]
- Susceptibility of multidrug-resistant gram-negative urine isolates to oral antibiotics. Antimicrob Agents Chemother. 2016;60:3138-40.
- [Google Scholar]
- In vitro activity of fosfomycin against Escherichia coli isolated from patients with urinary tract infections in Canada as part of the CANWARD surveillance study. Antimicrob Agents Chemother. 2014;58:1252-6.
- [Google Scholar]
- Determination of MIC distribution of colistin, fosfomycin, and tigecyclin antibiotics against carbapenem resistant Enterobacteriaceae. Biomed Res 2017:28.
- [Google Scholar]
- Frequency of colistin and fosfomycin resistance in carbapenem-resistant Enterobacteriaceae from a tertiary care hospital in Karachi. Infect Drug Resist. 2017;10:231-6.
- [Google Scholar]
- Emergence of carbapenemase-producing urinary isolates at a tertiary care hospital in Dhaka, Bangladesh. Ci Ji Yi Xue Za Zhi. 2016;28:94-8.
- [Google Scholar]
- Mechanisms of carbapenem resistance in K. pneumoniae and E. coli from bloodstream infections in India. Infect Dis Ther. 2016;4:293.
- [Google Scholar]
- Emergence of Escherichia coli, co-producing NDM-1 and OXA-48 carbapenemases, in urinary isolates, at a tertiary care centre at central India. J Clin Diagn Res. 2014;8:DC01-4.
- [Google Scholar]
- Nitrofurantoin resistance mechanism and fitness cost in Escherichia coli. J Antimicrob Chemother. 2008;62:495-503.
- [Google Scholar]
- An in vitro deletion in ribE encoding lumazine synthase contributes to nitrofurantoin resistance in Escherichia coli. Antimicrob Agents Chemother. 2014;58:7225-33.
- [Google Scholar]
- Characterization of plasmids carrying oqxAB in bla(CTX-M)-negative Escherichia coli isolates from food-producing animals. Microb Drug Resist. 2014;20:641-50.
- [Google Scholar]
- Complete sequence of the FII plasmid p42-2, carrying blaCTX-M-55, oqxAB, fosA3, and floR from Escherichia coli. Antimicrob Agents Chemother. 2016;60:4336-8.
- [Google Scholar]
- Dissemination and mechanism for the MCR-1 colistin resistance. PLoS Pathog. 2016;12:e1005957.
- [Google Scholar]




