
Translate this page into:
Superior vena cava syndrome
* For correspondence: menonara@yahoo.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 76 year old male presented as an outpatient to the department of Medicine, Command Hospital, Lucknow, India, in February 2014 with dyspnoea, dysphagia, hypophonia and significant weight loss. He had erythema, oedema of face, dilated veins over neck, anterior aspect of chest and abdomen with craniocaudal flow (Fig. 1). The patient was diagnosed to have superior vena cava (SVC) syndrome. Contrast enhanced computed tomography (CECT) of the chest showed a homogenous mass occupying the superior mediastinum occluding the SVC and displacing the trachea (Fig. 2). Trucut biopsy of the lesion revealed non-Hodgkin lymphoma (high grade). The patient was started on injection dexamethasone and chemotherapy with cyclophosphamide, hydroxydaunorubicin, vincristine and prednisolone. He however, succumbed to a cardiac event just before he was due for the second cycle of chemotherapy.
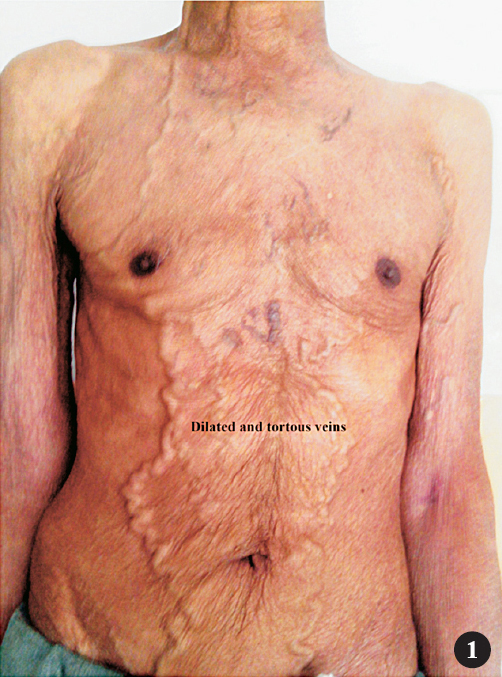
- Dilated and tortuous veins on chest and abdomen.

- CECT chest shows heterogenous mass encasing the superior vena cava (white arrow) and displacing the trachea (black arrow).




