Translate this page into:
Subclinical atherosclerosis in patients with rheumatoid arthritis by utilizing carotid intima-media thickness as a surrogate marker
Reprint requests: Dr Alladi Mohan, Professor & Head, Department of Medicine, Sri Venkateswara Institute of Medical Sciences Tirupati 517 507, India e-mail: alladimohan@svims.gov.in, alladimohan@rediffmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Patients with rheumatoid arthritis (RA) are more prone for accelerated atherosclerosis and Asian Indians as an ethnic group are predisposed to a high risk of premature atherosclerosis. However, sparse data are available regarding the burden of atherosclerosis among asymptomatic adult patients with RA in south India. We studied the burden of asymptomatic atherosclerosis in adult south Indian patients with RA at Tirupati, Andhra Pradesh, India, utilizing carotid intima-media thickness (CIMT) as a surrogate marker.
Methods:
Ultrasound examination of the carotids and CIMT measurement (mm) were carried out in 32 patients with RA, 32 age- and gender-matched normal controls, and 32 patients with atherosclerosis and angiographically proven coronary artery disease. The CIMT values in patients with CAD and normal controls were used to derive the appropriate cut-off value of CIMT for defining atherosclerosis that would be applicable for the ethnic population studied.
Results:
Patients with RA had a higher mean CIMT (mm) compared with normal control subjects (0.598 ± 0.131 vs 0.501 ± 0.081; P = 0.001). Carotid plaque was found more frequently among the cases compared with normal controls [5/32 (15.6%) vs 0/32 (0%), P=0.020]. Using this cut-off value derived by the receiver operator characteristic curve method (≥ 0.57 mm; sensitivity 84.4; specificity 90.6%) and the 75th percentile value among normal controls (≥ 0.55 mm) as surrogate markers, the presence of subclinical atherosclerosis was significantly more among asymptomatic patients with RA compared with normal controls [(59.3 vs 12.5%; P<0.001) and (62.5 vs 25%; P<0.001) respectively].
Interpretation & conclusions:
Based on the present findings CIMT appears to be a useful surrogate marker for detecting subclinical atherosclerosis in adult Indian patients with RA.
Keywords
Atherosclerosis
carotid intima-media thickness
India
rheumatoid arthritis

Rheumatoid arthritis (RA) is a chronic inflammatory disease that results in severe disability and premature mortality1. The systemic and articular inflammatory load drives the destructive progression of the disease, and the extent of inflammation in RA has been linked to an increased risk of cardiovascular mortality resulting from accelerated atherogenesis2. Mortality due to coronary artery disease (CAD) has been found to be 59 per cent higher in patients with RA when compared to general population3. This increase reflects the end-stage of persistence of a long standing immune inflammation and inflammation is considered as a novel risk factor for atherosclerosis4. Studies linking the two conditions have provided data positively correlating RA and atherosclerosis56. Single photon emission computed tomography (SPECT) studies have confirmed that myocardial perfusion abnormalities occur earlier in patients with RA7. The excess CAD is evident in both the genders. There appears to be a vascular involvement especially in seropositive RA with extra-articular features. The local vascular inflammation seems to induce diffuse endothelial dysfunction that initiates accelerated atherosclerosis1.
Carotid intima-media thickness (CIMT) is a simple, reliable, inexpensive, non-invasive marker that is increasingly being used to detect subclinical atherosclerosis and has been recommended by the American Heart Association (AHA), American Society of Echocardiography (ASE) and Society for Vascular Medicine (SVM) as a screening test for heart disease in apparently healthy individuals89. CIMT has been used in several clinical trials as a surrogate end point for evaluating the regression and/or progression of atherosclerotic cardiovascular disease89. At present, several non-invasive imaging techniques offer a unique opportunity to study the relation between surrogate markers and the development of atherosclerosis in patients with RA. The use of these techniques may help identify high risk RA patients who may benefit from active therapy to prevent clinical disease. One of these is the carotid ultrasonography that allows identifying the CIMT and presence of plaques1011. The importance of abnormally high CIMT and plaques as predictors of cardiovascular events in patients with RA has been emphasized1213.
As an ethnic group, Asian Indians are predisposed to a high risk of metabolic syndrome, and premature atherosclerosis14. Thus, Indian patients with RA appear to be at a higher risk for developing atherosclerosis. However, sparse data are available regarding the burden of atherosclerosis among asymptomatic adult patients with RA in south India. Therefore, the present study was designed to determine the presence of asymptomatic atherosclerosis in adult patients with RA in Tirupati, Andhra Pradesh, by utilizing CIMT as a surrogate marker.
Material & Methods
The sample size for the present study was calculated based on the following assumptions. Prevalence of asymptomatic atherosclerosis in adult population in Tirupati = 12.5 per cent15; prevalence of asymptomatic atherosclerosis in RA patients = 50 per cent, which is assumed to be four-fold of that observed in general population3; α = 5 per cent, power of the study (1-β) = 80 per cent. The sample size was calculated to be 46 (23 patients in each of RA and healthy normal control subjects). The study included 32 patients with RA and 32 control subjects. For deriving CIMT cut-off for the ethnic population included in the study, CIMT data obtained in 32 patients with angiographically proven CAD and the 32 healthy control subjects were studied.
Patients with RA (cases): Adult patients (aged 18 years or more) (n=32) diagnosed to have RA as per the revised American Rheumatology Association (ARA) criteria16 attending the Medicine Out-patient Department, Rheumatology clinic, and admitted to the Medicine Wards of the Sri Venkateswara Institute of Medical Sciences (SVIMS) hospital, a tertiary care teaching institute in Tirupati, Andhra Pradesh, India during February 2009 and July 2010 were included in the study. Patients with the following conditions were excluded from the study: (i) age under 18 years; (ii) RA overlap with other rheumatic diseases; (iii) patients with hypertension, diabetes mellitus, and clinically manifest atherosclerosis by way of CAD, peripheral vascular disease (PVD), and cerebrovascular disease; (iv) patients known to have dyslipidaemia of any aetiology and on treatment for the same; (v) history of smoking, alcoholism; and (vii) patients unwilling to participate in the study.
Control subjects: Age and gender matched healthy normal control subjects (n=32) from among the hospital staff and patient attendants were selected. Age- and gender-matched patients with atherosclerosis who had angiographically proven CAD (n=32) were also studied.
Study procedure: The study protocol was cleared by the Institutional Ethical Committee. A written, informed consent was obtained from all the patients and control subjects. In all of them, a detailed history was taken and a thorough physical examination and the following laboratory investigations were carried out: complete haemogram, fasting and post-prandial venous plasma glucose, liver and kidney function tests, serum lipids, urine analysis, rheumatoid factor, electrocardiogram (ECG), chest radiograph, and plain radiographs of the hands and wrists. Severity of RA was assessed using the Disease Activity Score (DAS) 28 score17.
Measurement of CIMT: Ultrasound examination of the carotids was carried out both in cases and controls using Sonoline G40 Diagnostic ultrasound system (Siemens Medical Solutions USA Inc., USA) by the same radiologist who was blinded to the clinical information and all measurements were obtained online. Measurements were made bilaterally at the carotid bulb, distal 1 cm of common carotid artery far wall proximal to the bulb and in the proximal most portion of the internal carotid artery near its origin. The mean of the six readings so obtained was used to calculate the CIMT. Plaque was defined as a focal protrusion of more than 50 per cent of the surrounding wall.
Statistical analysis: Data were recorded on a pre-designed proforma and managed using Microsoft Excel 2007 (Microsoft Corp, Redmond, WA). Descriptive statistics for the categorical variables were performed by computing the frequencies (percentages) in each category. For the quantitative variables, approximate normality of the distribution was assessed. Variables following normal distribution were summarized by mean and standard deviation. The association between two categorical variables was evaluated by Chi-square test or Fisher's exact test as appropriate. Student's ‘t’-test was used to compare the difference in mean values between the two groups for continuous variables that were normally distributed.
Two methods were used to calculate the cut-off of CIMT as a surrogate marker for atherosclerosis. The CIMT measurements in 32 patients with atherosclerosis and angiographically proven CAD and 32 healthy controls were used to derive the appropriate cut-off value of CIMT for defining atherosclerosis. Receiver-operator characteristic curve (ROC curve) for CIMT was plotted with (1-specificity) on the X-axis and sensitivity on the Y-axis using different cut-off levels of CIMT to arrive at the choice of the most appropriate cut-off level. The 75th percentile value of CIMT among the normal control subjects was also used as the optimal cut-off value for defining the presence of asymptomatic atherosclerosis in patients with RA9. The proportion of patients with atherosclerosis among cases and controls detected using these two cut-off values of CIMT as surrogate marker were compared using Chi-square test. The diagnostic yield of both the cut-offs in detecting subclinical atheosclerosis in patients with RA was tested using McNemar's test.
Statistical softwares PASW Statistics 18, Release 18.0.0, (IBM SPSS Statistics, Somers NY, USA); Systat 12, Version 12.00.08 (Systat Software, Inc, Chicago IL, USA); and MedCalc Version 11.3.0 for Windows 2000/XP/Vista/7 (MedCalc Software bvba, Belgium) were used for statistical analysis.
Results
During the study period, 48 patients with RA who had given consent to undergo evaluation were screened. Of these, 16 (33.3%) were excluded and 32 patients were included in the study as ‘cases’. The causes of exclusion were type 2 diabetes mellitus (n=7); dyslipidaemia (n=5), unwillingness to undergo further diagnostic testing (n=3); and tobacco smoking (n=1).
Demographic characteristics of patients with RA, age-, gender- and body mass index (kg/m2)-matched normal controls; and patients with atherosclerosis and angiographically proven CAD are shown in Table I. Majority of patients with RA were in their fifth decade of life; females (n=27) outnumbered males (n=5).

The median symptom duration among patients with RA (n=32) was 45.5 months [inter quartile range (IQR) 19.5 - 65 months]. The mean DAS28 score at presentation in these patients was 4.9 ± 2.1. Almost 50 per cent of the patients with RA (47%) had severe disease (DAS28 score ≥ 5.1); 41 per cent had mild to moderately severe disease. Only four patients (12%) were in remission.
Of the 32 patients with RA, 14 (43.8%) were treatment naïve and were receiving symptomatic treatment with non-steroidal anti-inflammatory drugs. Depending on disease severity as assessed by the DAS28 score, the remaining 18 (56.2%) patients were receiving a combination of disease modifying antirheumatic drugs (DMARDs) such as oral hydroxy chloroquine (n=17), weekly oral methotrexate (n=14) or injectable methotrexate (n= 2); daily oral prednisolone (n=7), oral leflunomide (n=4) and salazopyrine (n=3).
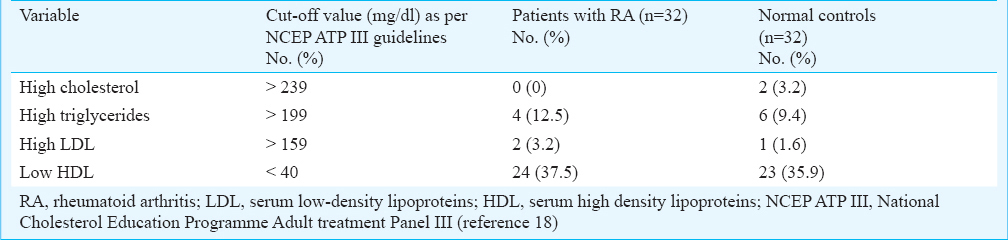
Comparison of serum lipid profile among patients with RA and normal controls is shown in Fig. 1. There was no significant difference in the mean serum cholesterol; triglycerides; LDL; and HDL levels between the two groups. The prevalence of dyslipidaemia defined as per the National Cholesterol Education Programme Adult treatment Panel III (NCEP ATP III) criteria18 in patients with RA and normal controls is shown in Table II. The percentage of patients with lipid abnormalities such as, a high serum cholesterol, triglycerides, LDL and low serum HDL were comparable between the two groups.

- Comparison of mean serum lipid levels (mg/dl) between cases and controls. Chol, serum cholesterol; LDL, serum low-density lipoproteins; TG, serum triglycerides; HDL, serum high density lipoproteins; VLDL, very low-density lipoproteins; RA, rheumatoid arthritis.
Majority of the patients with angiographically proven CAD had single vessel disease (n=15); while the others had triple-vessel disease (n=10) and two-vessel disease (n=7). The mean intima-media thickness (IMT) at various points of measurement and the mean of the six-readings, CIMT is shown in Fig. 2. The coefficient of variation for the mean of the six CIMT readings that was taken as CIMT measure in normal control subjects, patients with RA was calculated to be 16.1 and 21.8 per cent, respectively. Patients with RA had a higher mean CIMT compared with normal control subjects (0.598 ± 0.131 vs 0.501 ± 0.081 mm; P = 0.001). Carotid plaque was found more frequently among the cases compared with normal controls [5/32 (15.6%) vs 0/32 (0%), P=0.020].

- Box-whisker plot of mean intima-media thickness at six sites of measurement (mm) and the mean CIMT value (mm) in patients with RA (n=32) and normal control subjects (n=32). The circles and squares represent outlier values. LT_CCA, distal 1 cm of common carotid artery far wall proximal to the bulb on the left side; LT_BULB, left carotid bulb; LT_ICA, proximal most portion of the left internal carotid artery near its origin; RT_CCA, distal 1 cm of common carotid artery far wall proximal to the bulb on the right side; RT_BULB, right carotid bulb; RT_ICA, proximal most portion of the right internal carotid artery near its origin, carotid bulb, distal 1 cm of common carotid artery far wall proximal to the bulb and in the proximal most portion of the internal carotid artery near its origin; RA, rheumatoid arthritis.
Calculation of cut-off value of CIMT for the detection of atherosclerosis: The ROC-curve for calculating the optimal cut-off value of CIMT for detection of atherosclerosis is shown in Fig. 3. At a cut-off value of CIMT greater than or equal to 0.57, the sensitivity and specificity were 84.4 [95% confidence intervals (CI), 67.2 - 94.7] and 90.6 (95% CI, 75.0 - 98.0), respectively. The 75th percentile value of CIMT in normal control subjects was found to be 0.55 mm.

- ROC-Curve (thick line) along with 95% confidence bounds (interrupted lines) for calculating the cut-off value for CIMT as a surrogate marker of atherosclerosis. The area under the ROC curve (AUC) = 0.919; standard error = 0.0367; 95% Confidence Intervals = 0.824 to 0.973; Z-statistic = 11.427; significance level P (Area=0.5) = 0.000. CIMT, carotid intima-media thickness.
Presence of atherosclerosis among patients with RA and normal controls: Using the ROC-curve cut-off value (≥ 0.57 mm) as the surrogate marker, the proportion of patients with atherosclerosis was significantly higher among patients with RA compared with normal controls (59.3 vs. 12.5%; P<0.001). Using the 75th percentile value among normal controls (≥ 0.55 mm) as the surrogate marker, the proportion of patients with atherosclerosis was significantly higher among patients with RA compared with normal controls (62.5 vs. 25%; P<0.001) (Table III).

On comparing the proportion of patients with subclinical atherosclerosis among patients with RA identified with the ROC cut-off (19 of the 32) and the 75th percentile cut-off (20 of the 32) using McNemar's test, there was no significant difference between the diagnostic yield of both the methods.
Discussion
The prevalence of obesity and the incidence of metabolic syndrome is rapidly increasing in India and other south Asian countries, leading to increased morbidity and mortality due to type 2 diabetes mellitus and cardiovascular disease14. This increase has been observed not only in Indian adults and children but also in economically disadvantaged people residing in urban slums and rural areas. Given the unique susceptibility of Asian Indians to metabolic syndrome14 and the increased susceptibility and accelerated progression of atherosclerosis observed in RA, Indian patients with RA appear to be at a higher risk for developing atherosclerosis and related complications.
In the present study, majority of the patients with RA were females (n=27). Since RA predominantly affects women, and is also an independent risk factor, a search for asymptomatic atherosclerosis especially among women with RA using CIMT appears warranted. No significant difference in the lipid profile and presence of dyslipidaemia was found between the patients with RA and normal control subjects. Therefore, the presence of atherosclerosis among patients with RA assessed using CIMT as a surrogate marker appears to be a reflection of asymptomatic (subclinical) atherosclerosis. Significantly higher CIMT and more frequent finding of carotid plaques have been described in RA patients from Southern Europe with no classic cardiovascular risk factors or clinically evident cardiovascular disease19. The CIMT has been associated with the inflammatory burden and the chronicity of the inflammatory response. Long-standing RA patients with mean C-reactive protein (CRP) levels greater than 15 mg/dl had higher CIMT values than those with lower CRP levels20.
CIMT has been recommended to screen for heart disease in apparently healthy individuals and has been endorsed as a surrogate end-point for evaluating the regression and/or progression of atherosclerotic cardiovascular disease and as a predictor of the presence of coronary atherosclerosis and its clinical sequelae821. Other surrogate markers of cardiovascular disease such as flow-mediated dilatation have been also been found to be abnormal in RA. However, CIMT seems to be the more appropriate tool for establishing structural atherosclerotic disease. It has been observed that correlation between flow-mediated dilatation and CIMT may not be evident in recent onset RA and a disease duration longer than seven years was required to establish correlation between flow-mediated dilatation and morphological abnormalities expressed by carotid ultrasound22. CIMT also offers the advantage of low cost, wide availability in developing countries like India, relative comfort and convenience for the patient as it is a non-invasive investigation.
The mean CIMT value among patients with RA was significantly higher than that observed among normal control subjects in the present study. Similar observations were reported in other studies from India232425 and from other parts of the world2627. Patients with other factors that influence atherosclerosis such as hypertension, diabetes mellitus, hyperlipidaemia, among others were not excluded in some studies2428. Care was taken in the present study to exclude patients with other conditions that may contribute to atherosclerosis. Further, we also obtained six measurements to derive the CIMT including the proximal internal carotid bulb, where a higher prevalence and severity of atherosclerosis have been described29. However, a major limitation of CIMT as a marker for atherosclerosis is that there is no clear “threshold” for demarcating ‘normal’ and ‘abnormal’ values30. The consensus statement from the American Society of Echocardiography9 suggested that a value greater than 75th percentile for the patient's age, sex and race/ethnicity should be considered high and indicative of increased vascular risk. Normative values of CIMT for adult South Indian patients are not available in the published literature. In the present study an attempt was made to define the appropriate “cut-off” value for defining atherosclerosis. For this two methods, namely, construction of ROC-curve; and defining the 75th percentile value from normal control subject data were used.
In some Indian studies, arbitrary cut-offs, such as, 1 standard deviations (SD)23 or 2 SD25 above the mean value obtained for control subjects have been used; or, without defining a cut-off, comparison of mean CIMT values between cases and controls24 have been used to explain the significance of CIMT measurements. However, these methods do not appear to be the ideal methods for defining the cut-off value. In the present study, CIMT measurements obtained from patients with angiographically proven CAD and age- and gender-matched normal control subjects were used to construct an ROC curve and a cut-off value of 0.57 was derived. Patients with RA were categorized as having atherosclerosis if their CIMT value was greater than or equal to 0.57 mm. The performance of this cut-off value in detecting asymptomatic atherosclerosis among patients with RA was very similar to the 75th percentile value of CIMT in normal control subjects. Thus, these cut-off values of CIMT appeared to be appropriate for screening for asymptomatic (subclinical) athero-sclerosis among adult patients with RA.
Presence of carotid plaque is indicative of increased risk of atherosclerosis and cardiovascular disease and may signify the need for more aggressive risk-reduction interventions. In the present study, carotid plaque was found more frequently among the cases compared with normal controls. Further, frequent observation of asymptomatic atherosclerosis and carotid plaque among patients with RA assumes greater significance when interpreted in context of the mean age and proportion of female patients. In this study, women, a group conveniently thought to have lesser burden of atherosclerotic cardiovascular disease as compared to men, constituted 84 per cent of the patients and their mean age was only 47.4 ± 10.2 yr. The present study revealed that subclinical atherosclerosis, detected by CIMT as a surrogate marker and the presence of carotid plaques, is common in patients with RA. CIMT measurement was found to be a safe, inexpensive, reproducible, and repeatable strategy for detecting subclinical atherosclerosis. The cost- effectiveness of screening strategies for atherosclerosis like carotid ultrasound and the effect of interventional therapeutic strategies in risk reduction needs to be evaluated in longitudinal studies with a large sample size.
The present study was a cross-sectional study. Further longitudinal follow up these patients over a period of time to look for clinical events that reflect the consequences of atherosclerosis would provide valuable corroboration of the observations from the present study. The number of male participants was small in out study, so the upper limit as defined would perhaps be largely applicable to women.
Acknowledgment
The authors acknowledge the Sri Balaji Arogya Vara Prasadini scheme of Sri Venkateswara Institute of Medical Sciences and the Tirumala Tirupati Devasthanams, Tirupati for financial assistance.
References
- Rheumatoid arthritis: a disease associated with accelerated atherogenesis. Semin arthritis Rheum. 2005;35:8-17.
- [Google Scholar]
- Risk of cardiovascular mortality in patients with rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum. 2008;59:1690-7.
- [Google Scholar]
- Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;353:429-30.
- [Google Scholar]
- How early is the atherosclerotic risk in rheumatoid arthritis? Autoimmun Rev. 2010;9:701-7.
- [Google Scholar]
- An update on the relationships between rheumatoid arthritis and atherosclerosis. Atherosclerosis. 2010;212:377-82.
- [Google Scholar]
- Tackling ischaemic heart disease in rheumatoid arthritis. Rheumatology. 2003;42:607-13.
- [Google Scholar]
- 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2010;122:e584-636.
- [Google Scholar]
- American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr. 2008;21:93-111.
- [Google Scholar]
- Endothelial dysfunction, carotid intima-media thickness, and accelerated atherosclerosis in rheumatoid arthritis. Semin Arthritis Rheum. 2008;38:67-70.
- [Google Scholar]
- Validated methods for assessment of subclinical atherosclerosis in rheumatology. Nat Rev Rheumatol. 2012;8:224-34.
- [Google Scholar]
- Carotid intima-media thickness predicts the development of cardiovascular events in patients with rheumatoid arthritis. Semin Arthritis Rheum. 2009;38:366-71.
- [Google Scholar]
- Carotid atherosclerosis predicts incident acute coronary syndromes in rheumatoid arthritis. Arthritis Rheum. 2011;63:1211-20.
- [Google Scholar]
- The metabolic syndrome in South Asians: epidemiology, determinants, and prevention. Metab Syndr Relat Disord. 2009;7:497-514.
- [Google Scholar]
- Prevalence of coronary artery disease and coronary risk factors in an urban population of Tirupati. Indian Heart J. 2007;59:157-64.
- [Google Scholar]
- The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31:315-24.
- [Google Scholar]
- Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995;38:44-8.
- [Google Scholar]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III) JAMA. 2001;285:2486-97.
- [Google Scholar]
- Increased prevalence of severe subclinical atherosclerotic findings in long-term treated rheumatoid arthritis patients without clinically evident atherosclerotic disease. Medicine (Baltimore). 2003;82:407-13.
- [Google Scholar]
- High-grade C-reactive protein elevation correlates with accelerated atherogenesis in patients with rheumatoid arthritis. J Rheumatol. 2005;32:1219-23.
- [Google Scholar]
- Society of Atherosclerosis Imaging and Prevention Developed in collaboration with the International Atherosclerosis Society. Appropriate use criteria for carotid intima media thickness testing. Atherosclerosis. 2011;214:43-6.
- [Google Scholar]
- Correlation between endothelial function and carotid atherosclerosis in rheumatoid arthritis patients with long-standing disease. Arthritis Res Ther. 2011;13:R101.
- [Google Scholar]
- Subclinical atherosclerosis and endothelial dysfunction in patients with early rheumatoid arthritis as evidenced by measurement of carotid intima-media thickness and flow-mediated vasodilatation: an observational study. Semin Arthritis Rheum. 2012;41:669-75.
- [Google Scholar]
- Assessment of atherosclerosis by carotid intimomedial thickness in patients with rheumatoid arthritis. J Assoc Physicians India. 2008;56:587-90.
- [Google Scholar]
- Subclinical atherosclerosis in rheumatoid arthritis in India. J Rheumatol. 2006;33:244-7.
- [Google Scholar]
- Rheumatoid arthritis is an independent risk factor for increased carotid intima-media thickness: impact of anti-inflammatory treatment. Rheumatology (Oxford). 2010;49:1076-81.
- [Google Scholar]
- Common carotid intima-media thickness and von Willebrand factor serum levels in rheumatoid arthritis female patients without cardiovascular risk factors. Clin Rheumatol. 2007;26:533-7.
- [Google Scholar]
- Early atherosclerosis in rheumatoid arthritis: effects of smoking on thickness of the carotid artery intima media. Ann N Y Acad Sci. 2005;1051:281-90.
- [Google Scholar]
- Increased prevalence of carotid artery atherosclerosis in rheumatoid arthritis is artery-specific. J Rheumatol. 2010;37:730-9.
- [Google Scholar]
- Carotid intima-media thickness and coronary atherosclerosis: weak or strong relations? Eur Heart J. 2007;28:398-406.
- [Google Scholar]




