Translate this page into:
Spontaneous pneumothorax in ataxia telangectasia
*For correspondence: sudheerpgi@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 20 yr old male presented to Neurology Outpatient department, Postgraduate Institute of Medical Education and Research (PGIMER), in November 2012 with progressive cerebellar ataxia since the age of eight. The patient complained about a sudden onset shortness of breath for the past five days. Clinical examination revealed conjunctival and nail telangectasia (Figs. A and B). Chest roentgenogram showed right sided pneumothorax (Fig. C) that was managed with high flow oxygen and intercoastal drain insertion (Fig. D) following which the patient had symptomatic relief. CT of chest (Fig. E) and cranial MRI (Fig. F) revealed findings as described. A diagnosis of ataxia telangectesia was made based on clinical and laboratory findings (elevated serum AFP and reduced serum IgA and IgE levels). The patient had no complaints of dyspnoea, and pulmonary function tests done six months later were normal.
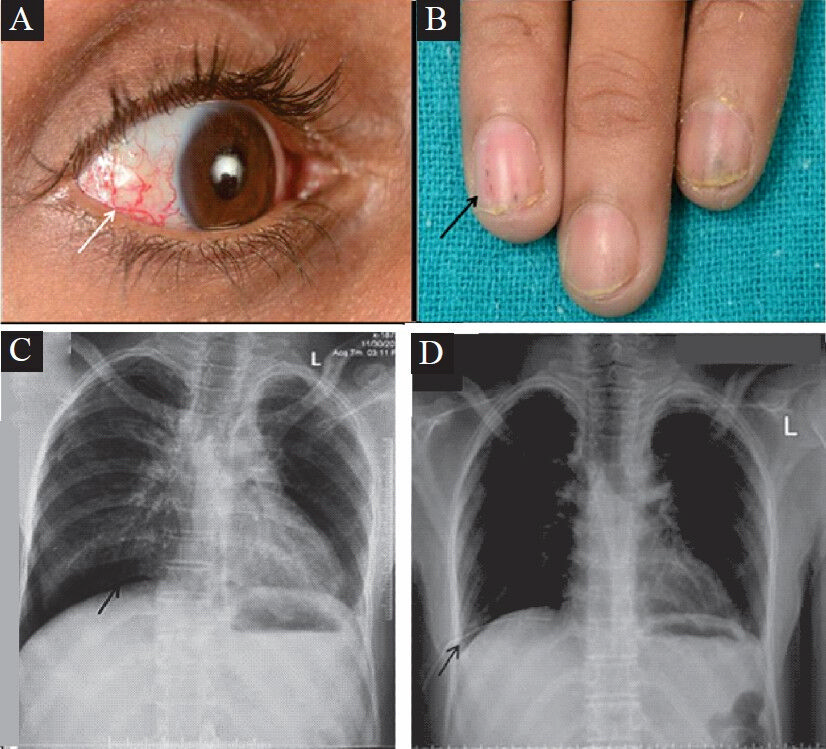
- Clinical photograph showing (A) ocular and (B) nail telangiectasia (arrows). Baseline X-ray chest posteroanterior (P/A) view (C) displayed right epidiaphragmatic and apical hyperlucencies (arrows) suggestive of pneumothorax with subsequent resolution of pneumothorax following insertion of intercostal tube (D) (arrow).
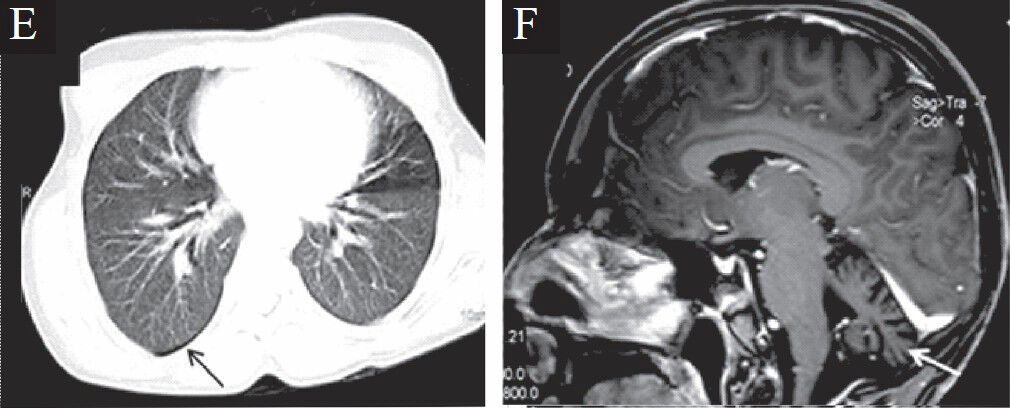
- Computerized tomograph of the chest (E) revealed presence of pneumothorax (arrow) with no parenchymal changes. Cranial MRI (F) depicted cerebellar atrophy (white arrow) without cerebral cortical parenchymal changes.




