
Translate this page into:
Serum prolactin levels in patients with psoriasis: Results of a pilot study
* For correspondence: vkm1@rediffmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Prolactin possibly plays a pathogenetic role in psoriasis by stimulating keratinocyte proliferation, T-lymphocyte interferon gamma production and promoting angiogenesis1. The inhibition of the T-suppressor cell functions by prolactin may serve to promote psoriatic plaque development2. It has been postulated that retinoids decrease the prolactin secretion from pituitary gland and add to their antipsoriatic effect3. Bromocriptine, an antiprolactin drug has been found useful in the treatment of psoriasis and psoriatic arthritis45. There are studies demonstrating serum prolactin levels varying with severity, duration and treatment of psoriasis5678. However, not many studies are available from India.
Fifty five male patients aged 22-66 years (mean ± SD 42.30±12.72 yr) having chronic plaque psoriasis for at least six months and presenting at the Dermatology, Venereology and Leprosy outpatient department, of Dr R.P. Government Medical College, Kangra (Tanda), Himachal Pradesh, India, during January to December 2012, were included in this study. Only those patients who gave written informed consent were included. Except for topical emollients and oral anti-histaminics, all topical and systemic treatments were stopped for two and four wk respectively before blood sampling. Patients with palmoplantar psoriasis, psoriatic arthritis, on medications or who had consumed foods (during the last one week) affecting prolactin levels (phenothiazines, metoclopramide, calcium channel blockers, methyldopa, cimetidine, alcohol, coffee and animal proteins) were excluded from the study. Patients with cardiovascular disease, peripheral vascular disease, systemic lupus erythematosus or having abnormal haemogram, fasting blood glucose, hepatorenal function tests or thyroid functions tests were also excluded. The study was approved by the institutional ethics committee.
Demographic profile, clinical details and baseline body surface area (BSA) involvement and psoriasis area-and-severity index (PASI) score9 were recorded and severity of psoriasis was graded as mild, moderate or severe (Table I). The 55 age-matched male patients (45.52 ±11.77 yr, range 20-65 yr) with or without minor dermatoses (dermatophytosis, scabies) and having no personal or family history of psoriasis, were included as controls. Blood samples (5 ml) were collected after overnight fasting between 0800 and 1000 h by antecubital venepuncture. Quantitative estimation for serum prolactin was performed by standard chemiluminescent immunoassay method and as per manufacturer protocol using Immulite® ready to use in vitro kits (Siemens Healthcare, Diagnostic Products Ltd., UK). Magnetic resonance imaging (MRI) of brain was performed to exclude prolactinoma in case serum prolactin levels exceeded 100 ng/dl.
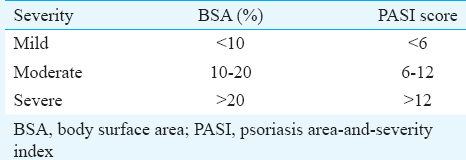
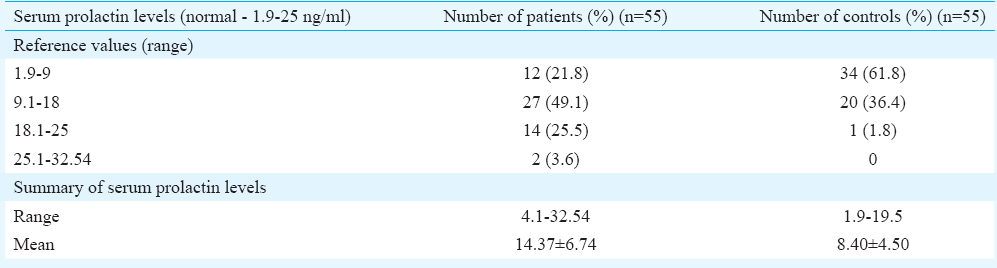
Of the 55 patients, 25 (45.5%) were aged between 22 and 40 yr, 23 (41.8%) were between 41 and 60 yr and seven (12.7%) patients were >60 yr of age. The duration of psoriasis varied between six months and 20 yr. Thirty five (63.6%) patients had the disease for less than five years while in 20 (36.4%) patients it was present for more than five years. BSA involvement was <10 per cent in 38 (69%), 10-20 per cent in 10 (18.2%) and >20 per cent in 7 (12.8%) patients, respectively. PASI score of <6 was seen in 41 (74.5%), 10 (18.2%) patients had PASI score of 6-12 and it was >12 in four (7.3%) patients. Serum prolactin levels (Table II) in 53 (96.4%) patients were though within normal range (1.9-25 ng/ml) but on higher side and varied between 4.1 and 24.68 ng/ml (14.37±6.74 ng/ml). The remaining two (3.6%) patients had serum prolactin levels above normal (26.50 ng/ml and 32.54 ng/ml). The controls had serum prolactin levels within normal range (8.40±4.50 ng/ml).
Elevated serum prolactin levels in patients with psoriasis have been considered to play a role in keratinocyte hyperproliferation and inflammation through enhanced production of chemokine CXC ligand (CXCL) 9, CXCL10, CXCL11610. Several workers have postulated significance of hyperprolactinaemia in the pathogenesis of psoriasis56710. El-Khateeb et al7 after studying elevated prolactin levels in the serum and blister fluid of psoriatic lesional skin of 15 psoriasis patients and healthy controls proposed that it was perhaps locally produced prolactin involved in the pathogenesis of psoriasis. Giasuddin et al6 observed significantly higher mean serum prolactin levels in psoriasis (25.8±16.1 ng/ml) as compared to that in atopic dermatitis (9.1±4.7 ng/ml) and healthy controls (10.3±5.3 ng/ml). Dilmé-Carreras et al5 observed significantly increased serum prolactin levels in psoriasis patients (21.4±16.7 ng/ml) as compared to healthy controls (8.4±5.2 ng/ml). The levels reduced significantly six weeks after treatment with tacalcitol ointment suggesting an association of elevated serum prolactin and disease activity5. The mean serum prolactin levels in most of our patients (96.4%) were on higher side of the normal as compared to that in controls. However, there was no variation of serum prolactin levels with reference to the PASI score. Gorpelioglu et al11 also reported similar findings in their study of 39 psoriasis patients and 36 controls. However, they did not consider increased prolactin levels in their nine patients and five controls significant as these were below 100 ng/ml, the minimum limit for the diagnosis of prolactinoma. Azizzadeh et al12 noted that serum prolactin levels varied with severity of disease in patients but observed no significant difference in mean serum prolactin levels between patients and controls. Keen and Hassan13 observed serum prolactin levels varying with severity of psoriasis and correlating with duration and treatment. Whether prolactin plays any significant role in the pathogenesis of psoriasis, its high serum levels are biological markers of disease activity or bromocriptine becomes a useful therapeutic option need confirmation after well-designed studies. Small number of patients/controls and no therapeutic follow up were major limitations of our study.
Conflicts of Interest: None.
References
- Prolactin stimulates proliferation of cultured human keratinocytes. J Invest Dermatol. 1993;101:275-9.
- [Google Scholar]
- Prolactin and the skin: A dermatological perspective on an ancient pleiotropic peptide hormone. J Invest Dermatol. 2009;129:1071-87.
- [Google Scholar]
- Effects of chronic retinoid administration on pituitary function. J Endocrinol Invest. 2005;28:961-4.
- [Google Scholar]
- Serum prolactin levels in psoriasis and correlation with cutaneous disease activity. Clin Exp Dermatol. 2011;36:29-32.
- [Google Scholar]
- Prolactin: Does it have a role in the pathogenesis of psoriasis? Dermatology. 1998;197:119-22.
- [Google Scholar]
- Prolactin level is significantly elevated in lesional skin of patients with psoriasis. Int J Dermatol. 2011;50:693-6.
- [Google Scholar]
- Correlation of serum prolactin levels and disease activity in systematic lupus erythematosus. Rheumatol Int. 2013;33:511-6.
- [Google Scholar]
- Prolactin enhances interferon-gamma-induced production of CXC ligand 9 (CXCL9), CXCL10, and CXCL11 in human keratinocytes. Endocrinology. 2007;148:2317-25.
- [Google Scholar]
- Is prolactin involved in etiopathogenesis of psoriasis? J Eur Acad Dermatol Venereol. 2008;22:1135-6.
- [Google Scholar]
- Serum prolactin levels in psoriasis and its association with disease activity: A case-control study. Indian J Dermatol. 2014;59:562-6.
- [Google Scholar]




