Translate this page into:
Seroprevalence of human immunodeficiency virus & hepatitis B virus co-infection in Belgaum, southern India
+For correspondence: mvparande@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Infection due to the human immunodeficiency virus (HIV) is a major public health issue globally, particularly in developing and populous countries. India also faces the menace of high prevalence of hepatitis B, which shares the same route and mode of transmission as HIV. The situation becomes more challenging with the occurrence of hepatitis B virus (HBV) co-infections in HIV positive persons, as people at high risk for HIV infection may be at increased risk for other pathogens including HBV1. Such HIV and HBV co-infection has been associated with reduced survival with an increased risk of progression to severe liver disease and hepatotoxicity, associated with antiretroviral therapy2. An estimated one third of deaths in HIV patients are directly or indirectly related to liver disease2. In order to devise prevention and intervention strategies, it is, therefore, important to understand the magnitude of such co-infections and dynamics of their transmission which may vary culturally and geographically.
The city of Belgaum is located in North-West Karnataka, India, and shares its borders with the States of Maharashtra and Goa and is, therefore, a multicultural region. Because of its strategic location and availability of several tertiary care hospitals, Belgaum caters to the health care needs of the region in North-West Karnataka as well as the neighbouring areas of Maharashtra and Goa. The present study was undertaken to understand the magnitude of HBV and HIV co-infections in Belgaum and gather demographic information that could be used for devising prevention and treatment strategies.
A total of 4026 serum samples of confirmed HIV positive cases which were received in the department of Microbiology from the Antiretroviral Therapy (ART) center of Belgaum Institute of Medical Sciences (BIMS) & District Civil Hospital, Belgaum, during a three year period from June 2007 to May 2010 were screened with a commercially available ELISA kits (ERBA lisa Hepatitis B, Transasia biomedicals, India and Microscreen HBsAg, Span Diagnostics Limited, India). The test was done according to manufacturer's instructions. Since samples from general population were not readily available, and population under consideration was predominantly adults, plasma from blood donors was likely to give an idea of baseline infections. Hence, 4030 consecutive blood samples from donors attending our hospital blood bank from June 2007 were screened for HBV infection using the same kit to provide baseline seroprevalence data in general population.
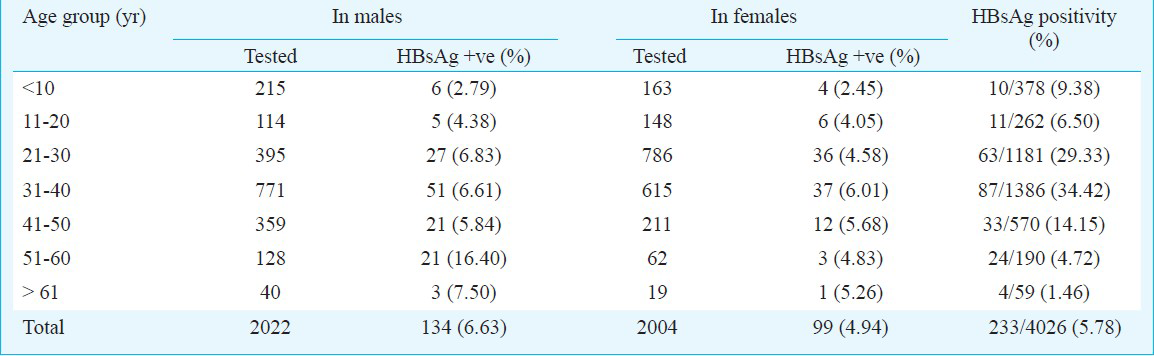
A total of 233 (5.78%) HIV infected individuals were found to be coinfected with HBV (Table), which was significantly higher (P<0.001) than that in apparently healthy donors 48 (1.19%). The HIV and HBV co-infection in males was slightly higher (134 of 2022, 6.63%) than that of the females (99 of 2004, 4.94%). Mohammadi et al2 also reported significantly higher HIV and HBV co-infection in males (51.5%) than in females (11.20 %). HBsAg positivity (P<0.05) varied significantly in different age groups. The mean age for the 4026 HIV positive individuals was 30.74 ± 12.96 yr (32.86 for males; 29.62 for females). In a study conducted in northern India the prevalence of co-infection was 9.9 per cent and mean age was 28.4 yr1. Our study showed that the HBV-HIV co-infection was highest among individuals of the age group of 31-40 yr followed by 21-30 yr which was similar to an earlier study3. Increase in the prevalence in this age group could be due to increased exposure to the risk factors. In our study the numbers of males and females were almost equal which was not the case in other studies where males were predominant134.
The implications of HIV and HBV co-infection is of serious concern in developing countries because of limited spectrum of readily available antiretroviral drugs. This has assumed more importance in some patients since the institution of highly active antiretroviral therapy (HAART) has prolonged the life of HIV positive patients but they need to be managed for the co-infection. A recent WHO report5 recommends, screening for HBV before initiation of ART and using ART containing tenofovir and either lamivudine or emtricitabine in HIV and HBV co-infected patients5. The present study underscores the importance of estimating the co-infections that may vary geographically as well as gender-wise in the process of mobilizing resources and implementation of prevention, control and ART programmes.
References
- Seroprevalance of hepatitis viruses in patients infected with human immunodeficiency virus. Indian J Pathol Microbiol. 2009;52:17-9.
- [Google Scholar]
- Survey of both hepatitis B virus (HBsAg) and hepatitis C virus (HCV Ab) coinfection among HIV positive patients. Virol J. 2009;6:202-9.
- [Google Scholar]
- Seroprevalence of hepatitis B surface antigen, antibodies to hepatitis C virus and Human immunodeficiency virus in a hospital based population in Jaipur Rajasthan. Indian J Community Med. 2010;35:165-9.
- [Google Scholar]
- HIV infection rates among persons attending an ICTC of a Delhi hospital. Indian J Sex Transm Dis AIDS. 2009;30:121-2.
- [Google Scholar]
- Antiretroviral therapy for HIV infection in adults and adolescents. Recommendations for public health approach - 2010 revision. Available from: http://whqlibdoc.who.int/publications/2010/9789241599764_eng.pdf
- [Google Scholar]




