
Translate this page into:
Sarcoidosis mimicking as liver & splenic abscess
*For correspondence: dr.aruntiwari@live.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 56 yr old man† presented to the department of Clinical Immunology and Rheumatology, Amrita Institute of Medical Sciences, Kochi, India, in June 2019, with recurrent pyrexial illness, papulopustular skin lesions (Fig. 1), constitutional symptoms and raised inflammatory markers for the last three years. Computed tomography of the abdomen revealed multiple hepatic and splenic lesions, suggestive of abscesses (Fig. 2). There was no growth documented on cultures, and tuberculosis workup was also negative. Biopsies taken from skin, liver and bone marrow were inconclusive. However, his positron-emission tomography (PET)-magnetic resonance (MR) showed inflammatory uptakes in the liver, spleen and abdominal lymph nodes (Fig. 3). Based on the above clinical, biochemical and radiological findings, a diagnosis of granulomatous disease was considered and the patient was subjected to repeat skin biopsy which revealed granulomas (Fig. 4). He was diagnosed with sarcoidosis and started on steroids and azathioprine. He was in remission at six months of follow up.

- Papulopustular skin lesions over trunk at the time of pyrexial illness.
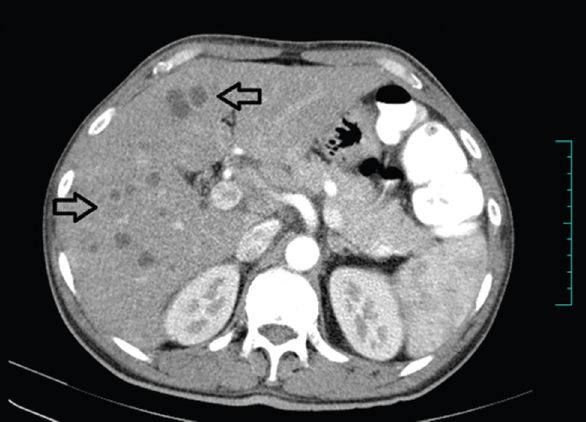
- Computed tomography abdomen image with liver showing multiple hypodense (marked with hollow arrows) lesion with subtle peripheral enhancement and splenomegaly.
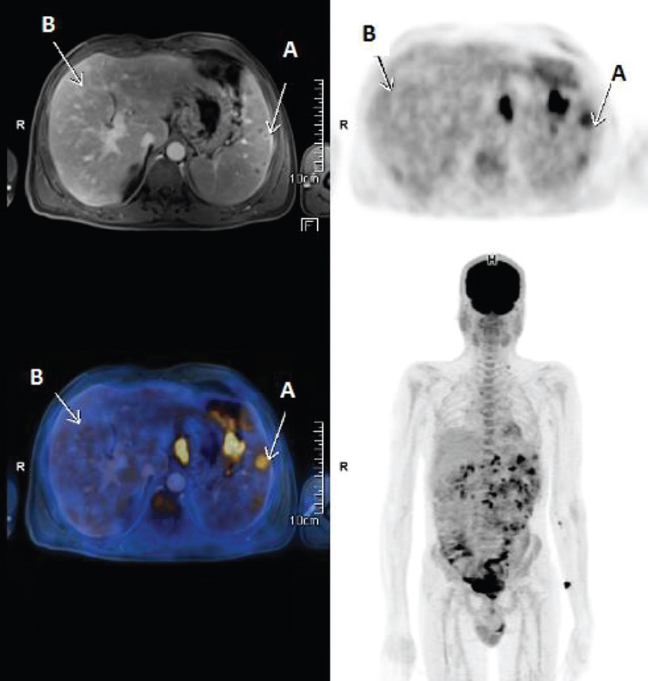
- Positron-emission tomography-magnetic resonance image showing FDG avid multiple mediastinal and intra-abdominal lymph nodes, FDG avid and non-avid T2 hyperintense lesions in the spleen (arrows noted A in image) and FDG non-avid T2 hyperintense lesions in the liver (arrows noted B in image).
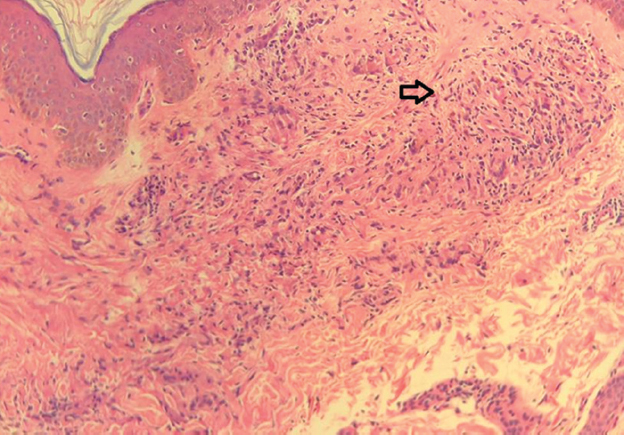
- Histopathology image: Skin biopsy, from papulopustular lesion over the upper back. Image showing ill-to-well-formed granulomas (hollow arrow) with giant cells, interstitial giant cells and histiocytes in the upper dermis (H and E, ×10).
Sarcoidosis has varied clinical manifestations, and in this case, it was a close mimic to liver, splenic abscess and skin pustulosis. Key points in this case that led to the diagnosis were multisystem involvement, abdominal lymph nodes uptake on PET, raised inflammatory markers and granulomas on skin biopsy.
Acknowledgment:
Authors acknowledge Dr Malini Eapen, Department of Pathology, AIMS, Kochi, for carrying out the histopathological analysis of the skin biopsy and providing the respective image.
Conflicts of Interest: None.




