
Translate this page into:
Ross syndrome
*For correspondence: pratyusha080@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 35 yr old male† presented with heat intolerance to the outpatient department of Ophthalmology, All India Institute of Medical Sciences, Mangalagiri, India, in July 2019. His vision was 20/20 (Snellen) and N6 (both eyes). There was anisocoria in light with right pupillary diameter of 5 mm (Figure A) and left of 2 mm (Figure B), respectively. There were light-near dissociation and dilatation lag on the right (Video). Eyelids, ocular movements and fundus examinations were normal.
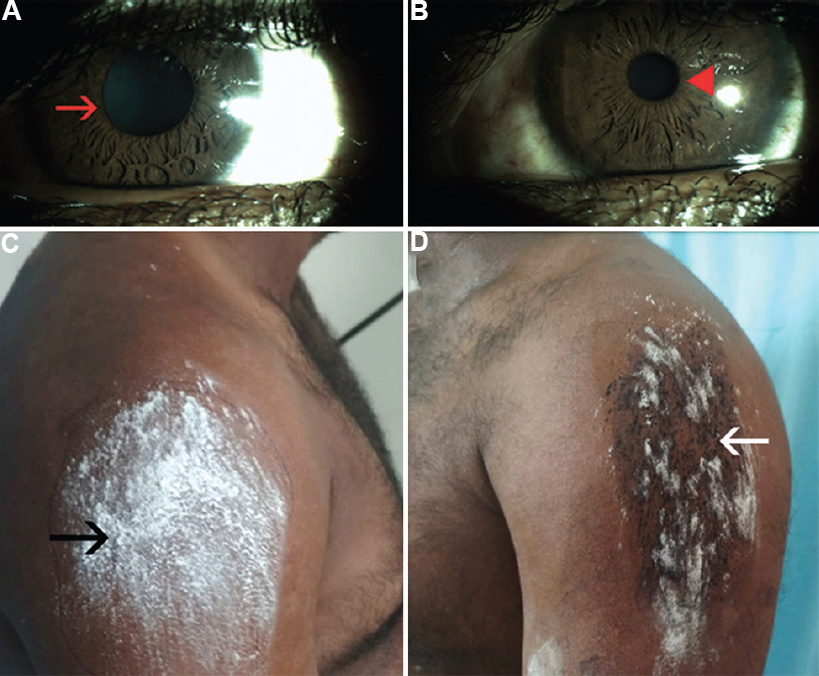
- (A) Clinical photograph showing anisocoria in light: right pupillary diameter of 5 mm (red arrow) and (B) left pupillary diameter of 2 mm (red arrowhead); (C) Iodine-starch test of the upper limb showing absence of staining on the right (black arrow indicating area of anhidrosis); and (D) staining on the left (white arrow indicating area of intact sweating).
Iodine-starch test showed decreased sweating over the right upper limb compared to the left (Figure C and D). Deep tendon reflexes of the upper and lower limbs were absent bilaterally. Complete haemogram, thyroid function tests, blood sugar and magnetic resonance imaging of the brain and spine were normal. The diagnosis of Ross syndrome was made (triad of tonic pupil, anhidrosis and areflexia). The patient was advised simple measures such as avoiding excess heat and wearing wet clothes during strenuous physical activity.
 Video available at ijmr.org.in.
Video available at ijmr.org.in.
Conflicts of Interest: None.




