Translate this page into:
Risk factor profile for non-communicable diseases among Mishing tribes in Assam, India: Results from a WHO STEPs survey
Reprint requests: Dr K.R. Thankappan, Professor & Head, Achutha Menon Centre for Health Science Studies, Sree Chitra Tirunal Institute for Medical Sciences & Technology, Thiruvananthapuram 695 011, India e-mail: kavumpurathu@yahoo.com/thank@sctimst.ac.in
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
A comprehensive risk factor profile of non-communicable diseases (NCDs) as suggested by the World Health Organization (WHO) has not been reported from tribal population in India. This survey was carried out to assess the prevalence of NCD risk factors among Mishing tribes in Assam using the WHO STEPs approach.
Methods:
A total of 332 individuals of the Mishing tribe (men 54%) aged 25-64 yr were selected from Tinsukia district by multistage cluster sampling. Using the WHO STEPs approach information was collected on demographics, STEP 1 variables (tobacco, alcohol, physical activity, diet) and measured STEP 2 variables (weight, height, waist circumference and blood pressure). Multivariate analysis was used to find the relation between STEP 1 and STEP 2 variables.
Results:
Overall, tobacco use was 84 per cent (men 94%; women 73%, P<0.001) and alcohol use was 67 per cent (men 82%; women 50%, P<0.05); 86 per cent reported vigorous physical activity, (men 91%, women 82%; P < 0.05). Sixty eight per cent reported to consume unhealthy diet (less than five servings of fruits and vegetables/day), 11 per cent had abdominal obesity, 16 per cent were overweight and 26 per cent had hypertension. Non users of tobacco and those who consumed more fruits and vegetables had higher prevalence of overweight (P<0.05). Among the hypertensives, 24 per cent were aware, 17 per cent treated and 2.4 per cent controlled their hypertension. Older individuals had higher hypertension prevalence (P<0.05) compared to younger individuals.
Interpretation & conclusions:
Tobacco use, alcohol use and unhealthy diet habits were high among men and women in this population and were major NCD risk factors. An integrated approach of culturally appropriate population level and high risk strategies are warranted to reduce these risk factors and to enhance adequate control of hypertension.
Keywords
Assam
India
non-communicable disease
risk factor profile
tribes
WHO STEPs

Non-communicable diseases (NCDs) are the major health issue for men and women in most countries, and a major challenge for all health-care systems1. As per the recent estimates, 34.5 million people died from NCDs in 2010, constituting 65 per cent of the 52.8 million deaths worldwide that year2. It has been projected that the deaths due to NCDs will increase to more than 50 million every year by 2030. In the developing countries, NCDs are projected to contribute 80 per cent of the global burden of disease and 70 per cent of deaths by 20203. In India, NCDs caused an estimated 50 per cent of all deaths and 62 per cent of the total disease burden in 20044. NCDs accounted for nearly 40 per cent of all hospital stays and 35 per cent of all outpatient visits in India in 20045.
High blood pressure, tobacco use, alcohol use, unhealthy diet and physical inactivity were identified as the leading risk factors of NCDs globally6. In addition, elevated blood glucose, abnormal serum cholesterol, overweight and obesity caused a substantial burden of NCDs in India4. If these risk factors are addressed adequately, 40-50 per cent of premature deaths due to NCDs in India could be prevented7.
World Health Organization (WHO) has developed the STEPs approach to conduct NCD risk factor surveillance to help member countries to monitor these risk factors and conduct appropriate interventions to reduce them. Seventy nine countries have already published the results of STEPs surveys and some of them conducted repeat surveys8. In India, the Indian Council of Medical Research (ICMR) with the support of the WHO conducted an NCD risk factor survey in five different geographical locations (East, South, North, West, Central India) from April 2003 to March 2005 which provided an estimate of the major NCD risk factors in these locations9. Another survey was conducted limiting to STEP 1 (questionnaire) and STEP 2 (clinical measurements) excluding the STEP 3 (biochemical measurements) in seven States (Andhra Pradesh, Kerala, Madhya Pradesh, Maharashtra, Mizoram, Tamil Nadu and Uttarakhand) in 2007-2008 providing State level estimates10.
Death rates due to NCDs were reported to be higher among people living in poor or marginalized communities11. Tribal population in India is considered the most disadvantaged in terms of health indicators. For example, under five mortality rate was highest among tribes (95.7) compared to schedule caste (88.1), other backward caste (72.8) and forward caste (59.2)12. In order to achieve substantial decrease in the total NCD burden, reduction of NCDs in disadvantaged groups is necessary11. However, data on NCD risk factors among tribal population are limited in India. A few studies reported selected NCD risk factors such as hypertension, tobacco use and alcohol consumption131415. Studies on other NCD risk factors like fruits and vegetables consumption and physical activity and a comprehensive risk factor profile of NCDs as suggested by the WHO have not been reported from tribal population in India. The present study was, therefore, aimed to assess the prevalence of NCD risk factors among Mishing tribes in Assam using the WHO STEPs approach and to estimate the association of behavioural risk factors with socio-demographic correlates and that of clinical risk factors (STEP 2) with behavioural risk factors (STEP 1).
Material & Methods
The present study was conducted among 25-64 yr old people of Mishing tribes living in the riverine islands in Tinsukia district of Assam, India during June to September 2011. Prevalence of hypertension (30%) reported by Hazarika et al13 from a pilot study among Assam tea garden workers, who are mostly tribals, was used to estimate the sample size of 350 with the worst acceptable limit as 25 per cent, a non response rate of 5 per cent and a design effect of 1.5.
Among the 27 administrative districts in Assam there were nine districts with Mishing Tribes16. Of these, one district (Tinsukia) was randomly selected for the study. There were four main human inhabited riverine islands of the river Brahmaputra in the district with only Mishing population (Erahuti, Miri chapori, Laika and Amarpur). All the four islands were selected for the study. In the next stage, villages were selected from these islands. Two of these islands Erahuti and Miri chapori had only one village each and both were selected. Two of the three villages from Laika and 10 of the 38 villages from Amarpur were also selected randomly (Figure). Each of the 14 villages was considered as a cluster. From each village 25 participants were selected to get a total sample of 350. All eligible individuals from the household who agreed to sign the consent form were included. All consecutive households were surveyed till the sample size of 25 from each village was achieved. In a few villages, this number exceeded 25 because all eligible adults in the last house visited were included.
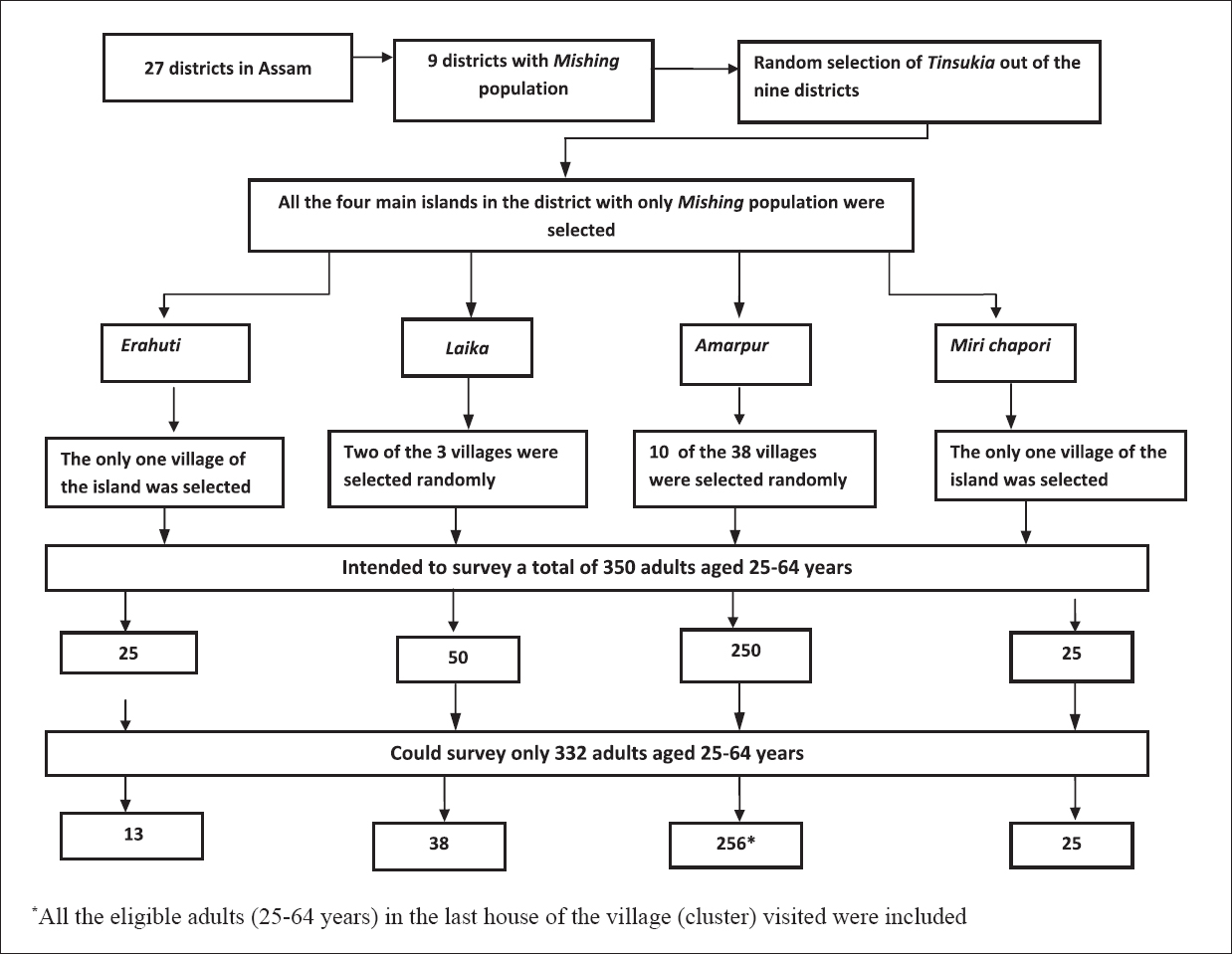
- Flowchart showing sample selection process.
A modified version of WHO STEPs questionnaire was used for NCD risk factor surveillance17. The English questionnaire was translated into Assamese (local language) and back translated to English by independent translators. Although this tribal population used a different language, majority of them could speak Assamese language. Due to limited resources, biochemical analysis (STEP 3) was not conducted. STEP 1 included information on age, sex, education, marital status, tobacco use, alcohol consumption, consumption of fruits and vegetables and physical activity. The common alcoholic beverage used by this tribal population was home made “Apong” which was reported to be closer to beer18. In STEP 2 height, weight, waist circumference and blood pressure were measured. SECA (Germany) weighing machine, constant tension tape and stadiometer were used to measure weight, waist circumference and height, respectively. Blood pressure was measured using Omron digital automatic blood pressure monitor three times (OMRON -4, Omron Corporation, Kyoto, Japan) for all participants in sitting position with the right arm at heart level. The average of the last two readings was taken as the final reading for that participant. All the measurements were taken according to the STEPs protocol17. Re-calibration of equipment was done at regular device-dependent intervals.
There was a high level of non-response reported from Laika island due to the erosion from floods prior to the survey. Most people of the Erahuti village left due to loss of house and property. Thus finally 13 tribals from Erahuti, 38 from Laika, 256 from Amarpur and 25 from Miri chapori islands were surveyed providing a total of 332 participants (Figure).
All participants were interviewed at their households during June to September 2011 by one of the authors (PJM) who had previous experience in working with this community. He was trained in survey research methods including the WHO STEPs. Bed ridden patients with debilitating illness were excluded.
Ethical clearance for the study was obtained from the institute ethics committee of the Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, Kerala, India. All participants gave written informed consent.
Data were coded and analysed according to the WHO guidelines17. Hours of physical activity of low, moderate and vigorous intensities were calculated by Metabolic Equivalent (MET) values using WHO guidelines. Current tobacco users were defined as individuals who used any form of tobacco during the last one month. Current alcohol users were those who consumed an alcoholic drink within the past 30 days. Binge drinking was defined as ≥5 standard drinks for men and ≥4 standard drinks for women in one day. Physical activity was captured in three domains; at work, during travel and during leisure time. Physical activity was classified according to MET minutes per week into three groups viz., low (<600), moderate (600-2999) and vigorous (≥3000). Unhealthy diet was defined as consumption of less than five servings of fruits and vegetables per day. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Individuals were grouped as overweight or obese if they had a BMI of ≥25 kg/m2. Abdominal obesity was defined as waist circumference of ≥ 90 cm for men and ≥ 80 cm for women. Hypertension was defined as systolic blood pressure of ≥140 mm of Hg and/or diastolic blood pressure of ≥ 90 mm of Hg or on medication for hypertension.
Analysis was performed using SPSS version 17.0 (SPSS Inc, Chicago, IL). Analysis on the NCD risk factors was done using WHO STEPs approach17. The mean values of continuous variables were compared between men and women using student ‘t’ test. Multiple logistic regression analysis was performed for finding out the predictors of STEP 1 and STEP 2 variables.
Results
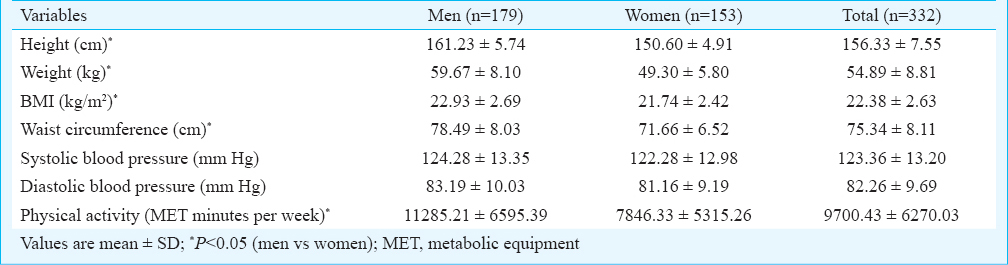
Mean age of the sample population was 38±9.6 yr. The basic demographic and behavioural risk factors for men and women are presented in Table I. The main occupation of the people belonging to the Mishing community was cultivation related activity throughout the year. They travel usually by walking or cycling and the leisure time physical activity included outdoor games like football, volleyball, etc. Women were also involved in cultivation, cycling and some outdoor games although to a lesser extend compared to men. Ever use of tobacco was 88.0 per cent (95% CI 83.9-91.1) (men 97.2%; women 77.1%) and current use was 84.3 per cent (95% CI 80.0-87.9). Average age at initiation of smoking for men was 19 yr (range 8-35 yr). On an average men were using four (range 1-20) sticks (cigarettes/beedies) per day. Mean value of NCD risk factors by sex are presented in Table II.
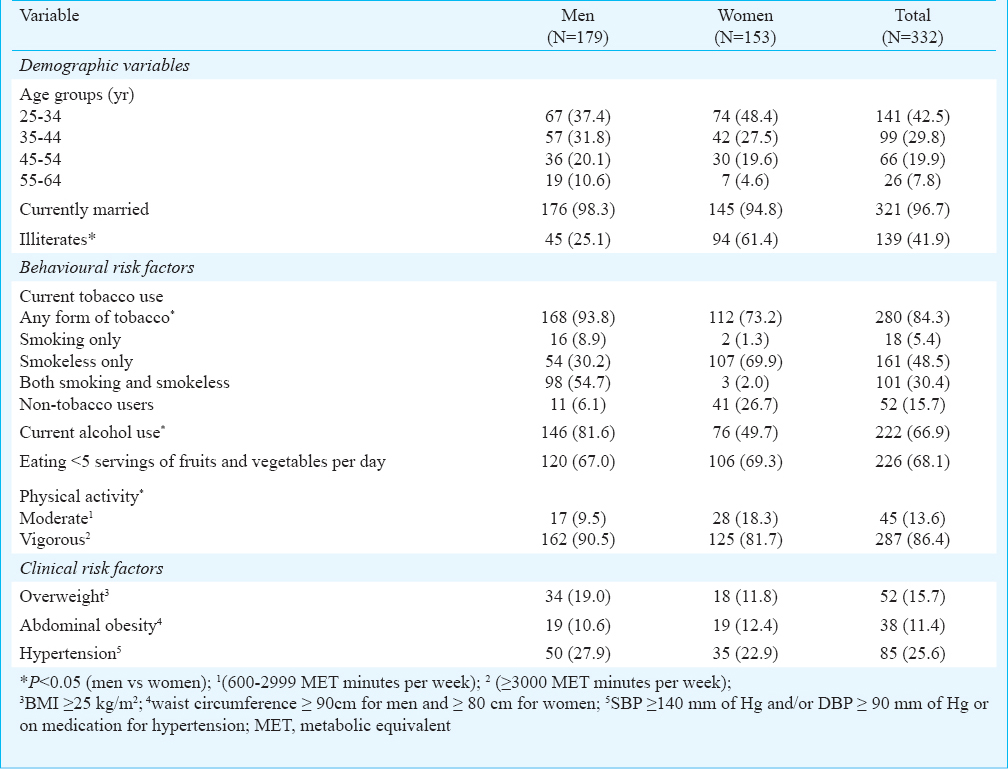
Ever use of alcohol was reported by 290 (87.3%) (95% CI 83.3-90.5) (men: 97.8%; women 75.2%) and current use by 222 (66.9%) (95% CI 61.6-71.7). Among the current alcohol users, 17.5 per cent of men and 9.6 per cent women reported binge drinking. Majority of the participants (n=299) (90.1%) were using either alcohol or tobacco. There was a significant association between alcohol and tobacco use (P<0.001). Among alcohol users 91.4 per cent used tobacco. Among 280 tobacco users, 203 (72.5%) used alcohol. Overall 61.1 per cent used both alcohol and tobacco.
Low level of physical activity was not reported by any of the study participants. Vigorous activity was reported by 287 (86.4%) (95% CI 82.3-89.7). Consumption of less than five servings of fruits and vegetables per day was reported by 226 (68.1%) (95% CI 62.9-72.9) participants. Overweight was seen in 52 (15.7%) (95% CI 12.1-19.9) and abdominal obesity in 38 (11.4%) (95% CI 8.4-15.4) of the participants. Hypertension was found in 85 (25.6%) (95% CI 21.2-30.6).
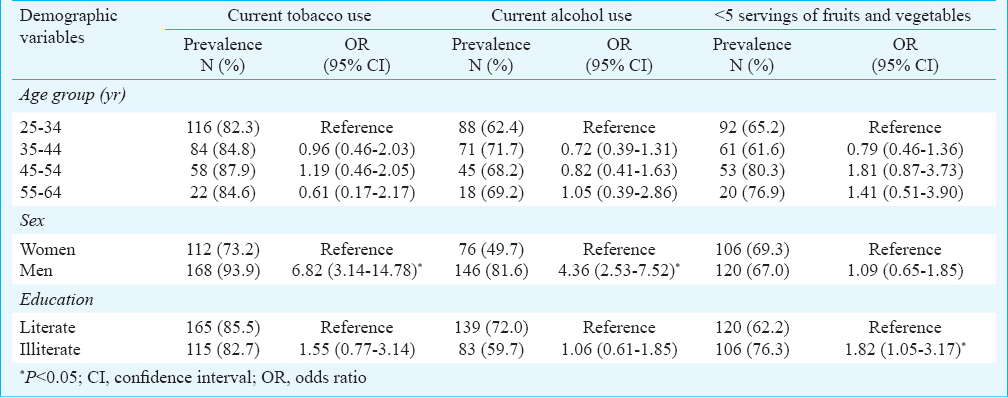
Only seven participants had checked their blood sugar prior to the survey and no one was reported to have diabetes. Results of multivariate logistic regression analysis on the demographic predictors performed separately for behavioural risk factors of tobacco use, alcohol use and unhealthy diet habits are presented in Table III. Since physical inactivity was not reported by any of the study participants, multivariate analysis was not performed on the predictors of physical inactivity. Men were seven times more likely to use tobacco (OR 6.82, 95% CI 3.14-14.78) and four times more likely to consume alcohol (OR 4.36, 95% CI 2.53-7.52) compared to women. Illiterates were more likely to have low fruits and vegetables intake (OR 1.82, 95% CI 1.05-3.17) compared to literates (Table III).
One hundred and twenty (36.1%) study participants checked their blood pressure earlier at least once in their life time. Of them, 20 (16.7%) reported that they were told by a health professional to have raised blood pressure and 70 per cent of them were currently taking medication. Eight five (25.6%) participants were found to be hypertensives (men 27.9%; women 22.9%). Sixty five (19.6%) of the 332 participants were newly detected to have hypertension in this survey. Of all the hypertensive individuals in this population, 76.5 per cent were newly detected. Among the 85 hypertensives, 20 (23.5%) were aware of their hypertension, 14 (16.5%) were on treatment and two (2.4%) could adequately control their hypertension.
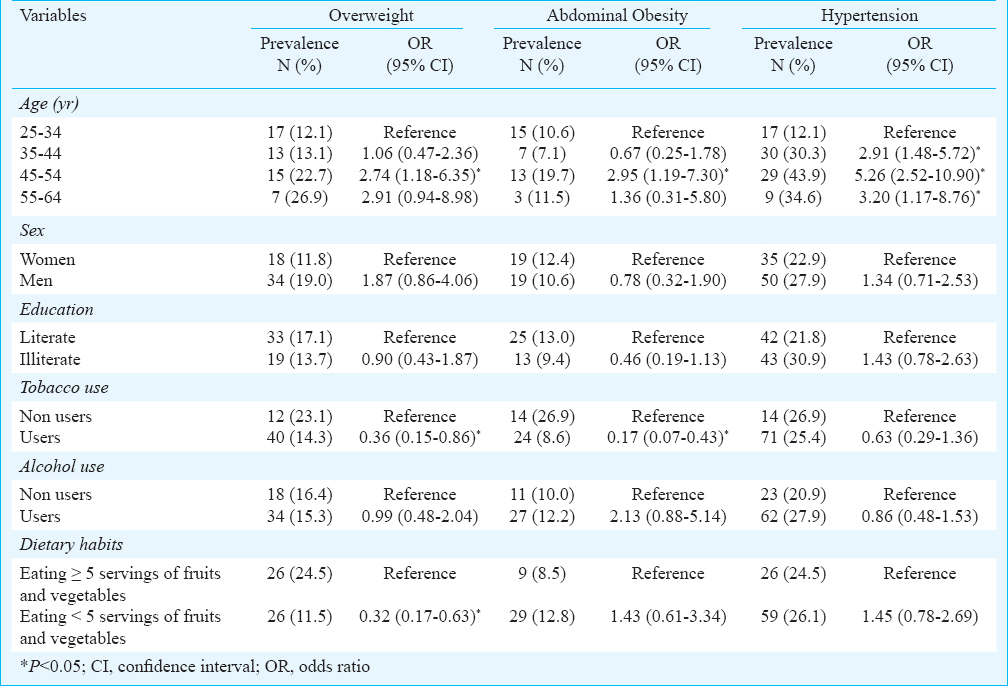
Multivariate logistic regression analysis on STEP 1 predictors of STEP 2 variables was done separately for each variable (overweight, abdominal obesity and hypertension) and the results are presented in Table IV. Participants in the age group of 45-54 yr were more likely to be overweight (OR 2.74, 95% CI 1.18-6.35), had higher abdominal obesity (OR 2.95, 95% CI 1.19-7.30) and hypertension (OR 5.26, 95% CI 2.52-10.90) compared to the lower age group. Tobacco users were less likely to be overweight (OR 0.36, 95% CI 0.15-0.86) and have abdominal obesity (OR 0.17, 95% CI 0.07-0.43) compared to non users of tobacco.
Discussion
This study provides NCD risk factor profile of Mishing tribes in Assam using WHO STEPs approach. Tobacco use of 94 per cent reported by men in the present study was higher than the 72 per cent prevalence among general men population of Assam. Similarly 73 per cent of women in our study reported tobacco use compared to 23 per cent in the general women population of Assam12. Overall smoking prevalence of 36 per cent reported in our study was similar to the 34 per cent reported from the tribes of Madhya Pradesh19, much higher than the 12.5 per cent reported from rural20 and 7.5 per cent among tribal population of Assam13. Smoking prevalence of 63.6 per cent among men in our study was higher than the State average of 36 per cent among 15-49 yr old men12, higher than the 54 per cent among 15- 74 yr old Indonesian men, and lower than the 68 per cent among 25-64 yr old Vietnamese men2122. Smokeless tobacco prevalence of 85 per cent among men in our study was higher than the 59 per cent among 15-49 yr old Assam men12 and slightly lower than the 88 per cent reported among tribal population in Assam13. The 72 per cent prevalence of smokeless tobacco use among women in our study was much higher than the 23 per cent among 15-49 yr old Assam women and lower than the 85 per cent reported by tribal population of Assam13. Overall tobacco consumption of 84 per cent in our study was lower than the 88 per cent reported by the Nicobarese tribes in India15.
Tobacco consumption in tribal population in India including the Mishing tribes in Assam was very high. Therefore, culturally appropriate tobacco cessation services integrated with health services delivery are urgently required to enhance quit rate in this population.
Alcohol use in 67 per cent population in our study was lower than the 78 per cent reported among tea garden workers in Assam23 and higher than the 13 per cent among Saharia tribes of Madhya Pradesh19, six per cent among tribal population in Gujarat14, 54 per cent among Nicobarese tribes15 and 36 per cent of rural population of Assam13. Prevalence of alcohol use among men in our study (82%) was higher than the 38 per cent prevalence reported among general men population in Assam12. Half of the women in our study reported alcohol consumption which was higher than the eight per cent reported among the general women population of Assam12. Similar to tobacco use, alcohol consumption was also very high in this population. Overall, more than 60 per cent of this population used alcohol and tobacco, the two major NCD risk factors. Both these risk factors are independently associated with several cancers and their simultaneous use is likely to multiply the risk for cancer.
Percentage of participants consuming less than five servings of fruits and vegetables per day (68%) was higher than the 47 per cent reported from general population of Kerala24. Although the study was done in summer season, seasonal variation is unlikely to be a reason for the low intake of fruits and vegetables since their availability is not lower in summer season. They used potato very often which was not considered as a vegetable in our study25. Higher prevalence of consumption of less than five servings of fruits and vegetables per day was reported from rural areas of India (82.1% men and 87.2% women)9.
Mean physical activity reported in the study was higher than that reported from earlier study among migrant groups in India26. Vigorous activity of 86.4 per cent reported in the present study was higher than that reported from Kerala (23.7%)24. As expected from a tribal population, level of physical activity was very high as no one belonged to the group of low level physical activity.
The 16 per cent prevalence of overweight reported in our study was lower than the 37 per cent reported among the Nicobarese tribes15, higher than the six per cent reported among tribes in Assam23. Prevalence of 19 per cent overweight men was higher than the eight per cent in rural Delhi27. Overweight of 12 per cent among women was similar to the 11 per cent reported from rural Delhi9.
Nobody in our sample reported diabetes mellitus which was similar to the National Family Health Survey report of 0.4 per cent for women and 0.5 per cent for men among tribal population in India12. In the ICMR-WHO STEPs study self reported diabetes prevalence was 4.5 per cent ranging from 3.1 per cent in rural areas to 7.5 per cent in urban areas of India28. The low rates of diabetes in our study could be due to high level of physical activity, low rates of overweight and abdominal obesity and low detection rates.
Hypertension was seen in 26 per cent in our study population which was lower than the 61 per cent among tribes in Assam13 and the 51 per cent among Nicobarese tribes15 and lower than the 33 per cent reported from rural Assam20. Hypertension awareness of 24 per cent in our study was higher than 13 per cent reported among tribes in Assam13 and the 12 per cent among Nicobarese tribes15 and similar to the 22 per cent in rural Assam20. Those who were on treatment for hypertension were 17 per cent which was higher than the 2.2 per cent reported among the Nicobarese tribes15 and the 4.3 per cent among other tribes in Assam13.
The relationships between demographic variables and STEP 1 variables, and between STEP 1 and STEP 2 variables were weak because of lack of heterogeneity of the risk factors among the population studied. Tobacco use among men in our population was significantly higher compared to women similar to other studies among tribes and general population in India1224. Alcohol use was also significantly higher among men compared to women similar to previous studies among tribal and non-tribal population in India1224. The increased prevalence of hypertension in higher age groups was similar to previous studies in tribal1315 and non-tribal populations in India924. Lower odds of overweight and obesity among tobacco users was reported in previous WHO STEPs surveys2124.
The major strengths of our study were (i) all interviews and measurements were done by a single investigator at the participants’ households, and (ii) all core risk factors suggested by WHO STEPs were captured in this study. One of the limitations of our study was the low sample size compared to what is recommended by WHO, which restricted our analysis into different age deciles. Future studies with sufficient samples size as recommended by the WHO including all the three steps of data collection (Questionnaire, clinical measurement and biochemical measurement) are likely to provide detailed risk factor profile in different age deciles. However, the overall risk factor estimates for the age group of 25-64 yr for men and women could not have been affected by this sample size.
In conclusion, tobacco and alcohol use, two of the major NCD risk factors were high in this population. Even among women these risk factors were very high unlike non-tribal women in India and other Asian countries. A strong positive behaviour was the high level of physical activity among this population which could be the reason for low level of overweight and abdominal obesity. Unhealthy diet was more prevalent among the illiterates which could be resolved by better education. Hypertension prevalence was lower than other tribal population in India, although similar to general population in India. Awareness on hypertension was higher than other tribal population but lower than the general population. Treatment and control of hypertension was also lower than general population probably due to inadequate access to health care.
References
- Globalisation and the prevention and control of non-communicable disease: the neglected chronic diseases of adults. Lancet. 2003;362:903-8.
- [Google Scholar]
- Embedding non-communicable diseases in the post-2015 development agenda. Lancet. 2013;381:566-74.
- [Google Scholar]
- The burden of non communicable diseases in developing countries. Int J Equity Health. 2005;4:2.
- [Google Scholar]
- The economic implications of non-communicable disease for India. 2010. HNP Discussion paper. Available from: http://siteresources.worldbank.org/HEALTHNUTRITIONANDPOPULATION/Resources/281627-1095698140167/EconomicImplicationsofNCDforIndia.pdf
- [Google Scholar]
- A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224-60.
- [Google Scholar]
- The burden of non-communicable diseases in India, Hamilton ON: The Cameron Institute. 2010. Available from: http://cameroninstitute.com/attachments/044_The%20burden%20of%20non-communicable%20dieases%20in%20India.2010.pdf
- [Google Scholar]
- STEPs country reports. World Health Organization (WHO) Available from: http://www.who.int/chp/steps/reports/en/index.html
- [Google Scholar]
- Surveillance of cardiovascular disease risk factors in India: The need & scope. Indian J Med Res. 2010;132:634-42.
- [Google Scholar]
- IDSP Non-Communicable Disease Risk Factors Survey, Phase-I States of India, 2007- 08. New Delhi, India: National Institute of Medical Statistics and Division of Non-Communicable Diseases, Indian Council of Medical Research; 2009.
- [Google Scholar]
- Inequalities in non-communicable diseases and effective responses. Lancet. 2013;381:585-97.
- [Google Scholar]
- International Institute for Population Sciences (IIPS) and Macro International. In: National Family Health Survey (NFHS-3) India, 2005-06: Assam. Mumbai: IIPS; 2008.
- [Google Scholar]
- Hypertension and its risk factors in tea garden workers of Assam. Natl Med J India. 2002;15:63-8.
- [Google Scholar]
- Epidemiological factors associated with hypertension among tribal population in Gujarat. Natl J Commun Med. 2011;2:133-5.
- [Google Scholar]
- Association of hypertension with risk factors & hypertension related behaviour among the aboriginal Nicobarese tribe living in Car Nicobar Island, India. Indian J Med Res. 2011;133:287-93.
- [Google Scholar]
- Mishing tribes, Assam. Available from: http://www.indianetzone.com/45/mishing_tribe.htm
- [Google Scholar]
- Surveillance of risk factors for non communicable diseases. The WHO STEP wise approach. Non communicable diseases and mental health. 2003. Geneva: World Health Organization; Available from: http://www.who.int/ncd_surveillance/steps/riskfactor/en/index.html
- [Google Scholar]
- Evaluation of nutritional and biochemical aspects of Po:ro apong_(Saimod)-A home made alcoholic rice beverage of Mising tribe of Assam, India. Indian J Tradit Knowl. 2012;11:499-504.
- [Google Scholar]
- Selected risk factors associated with pulmonary tuberculosis among Saharia tribe of Madhya Pradesh, central India. Eur J Public Health. 2012;22:271-3.
- [Google Scholar]
- Hypertension in the native rural population of Assam. Natl Med J India. 2004;17:300-4.
- [Google Scholar]
- Preventable risk factors for noncommunicable diseases in rural Indonesia: prevalence study using WHO STEPS approach. Bull World Health Organ. 2006;84:305-13.
- [Google Scholar]
- Prevalence of risk factors for non-communicable diseases in the Mekong Delta, Vietnam: results from a STEPS survey. BMC Public Health. 2009;9:291.
- [Google Scholar]
- Prevalence of hypertension and its risk factors in a tea garden community of Dibrugarh District, Assam. Indian J Public Health. 2008;52:45-7.
- [Google Scholar]
- Risk factor profile for chronic non-communicable diseases: results of a community-based study in Kerala, India. Indian J Med Res. 2010;131:53-63.
- [Google Scholar]
- Measuring intake of fruits and vegetables, Background paper for the joint FAO/WHO workshop on fruits and vegetables for health, 1-3 September, 2004. Kobe, Japan: World Health Organization; 2005.
- [Google Scholar]
- Socio-demographic patterning of physical activity across migrant groups in India: results from the Indian Migration Study. PLoS One. 2011;6:e24898.
- [Google Scholar]
- Differences in body mass index and waist: hip ratios in North Indian rural and urban populations. Obes Rev. 2002;3:197-202.
- [Google Scholar]
- Urban rural differences in prevalence of self-reported diabetes in India--the WHO-ICMR Indian NCD risk factor surveillance. Diabetes Res Clin Pract. 2008;80:159-68.
- [Google Scholar]




