
Translate this page into:
Rhabdomyolysis with cardiac dystrophic calcification
*For correspondence: sanjayvanita@yahoo.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
An 18 yr old boy presented to the emergency medical service in August 2012 at the Postgraduate Institute of Medical Education and Research, Chandigarh, India, with fever and oliguria following vigorous physical exercise. On evaluation, he had elevated serum creatinine (10.4 mg%), phosphate (11 mg%), uric acid (10.97 mg%), creatine phosphokinase (1939 U/l) and urine myoglobin 2765 ng/ml (reference value <0.025 µg/ml). A diagnosis of exertional rhabdomyolysis was made. Renal biopsy showed pigment cast nephropathy which was positive for myoglobin stain and negative for hemosiderin stain. Antinuclear antibody (ANA) and anti-neutrophil cytoplasmic antibody (ANCA) were negative. Serum complement levels were normal. He had hypocalcaemia (5.3 mg%) in early oliguric phase followed by hypercalcaemia (12.5 mg%) in the diuretic phase, a typical biochemical feature of rhabdomyolysis. His intact parathyroid hormone level was 6.52 pg/ml. Chest X-ray and computed tomography showed calcification in the heart (predominantly in the left atrium, Fig. 1a, b, d and e) and skeletal muscles (Fig. 1c). The patient improved with haemodialysis (8 sessions over 20 days) and follow up and showed resolution of skeletal muscle calcification although cardiac calcification persisted (Fig. 2a, b). He had no evidence of chronic kidney disease, and during the three year follow up, there was no recurrence of symptoms. Although dystrophic calcification is common in rhabdomyolysis, cardiac calcification is very rare.
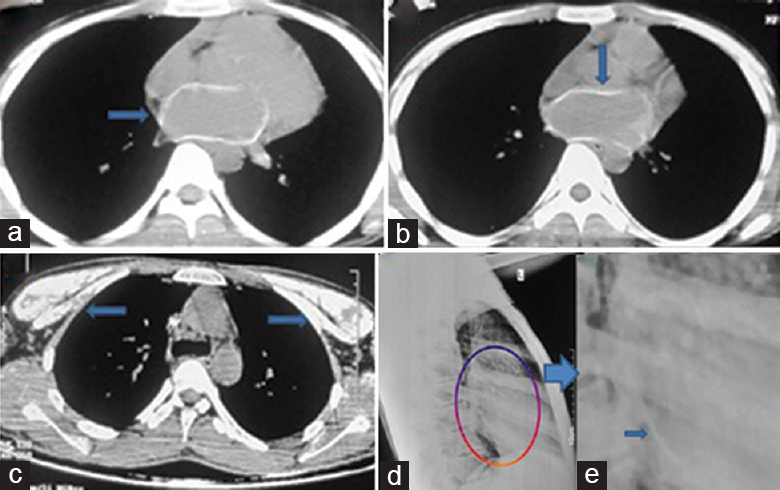
- Computed tomography (a-c) and chest X-ray (d magnified in e) showing cardiac calcification (predominantly in the left atrial) and skeletal muscle (c) calcification (shown by arrows).
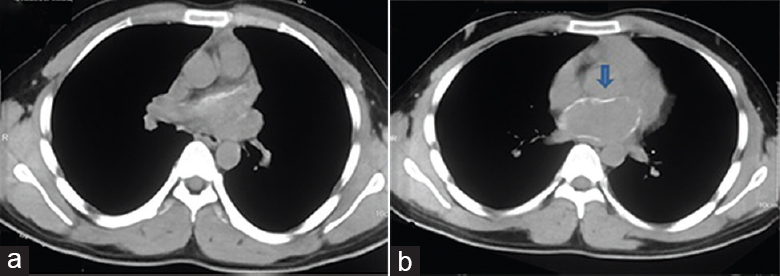
- Computed tomography of chest (a & b) showing resolution of skeletal muscle calcification but cardiac (left atrial) calcification persisted (arrow).




